IJCRR - 8(12), June, 2016
Pages: 35-38
Date of Publication: 20-Jun-2016
Print Article
Download XML Download PDF
GROSS ANATOMICAL VARIATIONS IN THE THEBESIAN VALVE COVERING THE CORONARY SINUS OSTIUM: A CASE STUDY
Author: Anitha Thillai, Anjana TSR, Sivakami Thiagarajan
Category: Healthcare
Abstract:Objectives: The Coronary Sinus (CS) is a widely employed structure for cannulation during electrophysiologic procedures like catheter ablation of arrhythmias, implantation of resynchronization therapy devices and percutaneous mitral valve repair. The present study aims to evaluate the variations in the Thebesian valve covering the coronary sinus ostium.
Materials and Methods: The present study was conducted in randomly selected 100 human cadaveric hearts from the Department of Anatomy and autopsied bodies of Department of Forensic Medicine, Thanjavur Medical College. The presence or absence of Thebesian valve, shape of the valve, presence or absence of fenestrations in Thebesian valve were noted.
Results: The Thebesian valve was present in 84% and was absent in 16%.The shape of the valve was semicircular in 84.7%, strands in 8.3% and bands in7%.The valve was fenestrated in 20.2%. An interesting variation of double crescentic Thebesian valve was present in one specimen.
Conclusion: This study showed that the Thebesian valve was present in 84% of heart specimens. The prominent Thebesian valve or a fenestrated valve or a large band may be an under recognised problem interfering with cannulation. It may pose a significant challenge with regards to cannulation of coronary sinus ostium during various invasive procedures like catheter ablation for arrhythmias, implantation of resynchronization therapy devices and percutaneous mitral valve repair and coronary lead placement.
Keywords: Coronary sinus, Coronary sinus ostia, Thebesian valve, Cannulation
Full Text:
INTRODUCTION
In the past, the importance of the cardiac venous system had been overshadowed by the proximate presence of the coronary arterial tree. Off late, the venous system has captured wider attention. The veins of the cardiac venous system can be used as a potential conduit in performing coronary artery bypass graft procedures and delivery of stem cells to infarcted myocardium(1). Coronary Sinus (CS) is a short and wide venous trunk of about 2- 3 cm long. It begins as the continuation of Great Cardiac Vein at the confluence of the Oblique vein of the left atrium (Vein of Marshall)(2,3). It lies posteriorly in the coronary sulcus between the left atrium and left ventricle. The sinus opens into the smooth part of right atrium through the Coronary Sinus ostium(CSo)(2,3,4,5). The CS ostium is covered to a variable extent, by the Thebesian valve. It is also called as Thebesius valve or valve of Coronary Sinus. Sometimes the valve may be absent(3,6,7,8,9). The shape of the valve is crescentic or semi-circular in most cases. If the valve is not crescentic, it may be strand shaped or band shaped. Normally the valve covers the superior and posterior surfaces of the ostium. Sometimes it may cover the ostium completely with the formation of fenestrations. Rarely, the valve may cover the inferior hemi-circumference (10,11). These valves with increased coverage may obstruct during cannulation of the CS. If the valve covers about 75% of CS ostium, it may pose difficulty during cannulation of CS. It has been known to display significant variation and it is noteworthy that even as early as 1951, investigators have speculated on the potential of the valve to interfere with cannulation of the coronary venous system(2). Hence the present study aims to analyse and reemphasise the importance regarding the anatomy and variations of the Thebesian valve covering the Coronary Sinus ostium.
MATERIALS AND METHODS
The hearts were removed en bloc from 100 adult cadavers in the Department of Anatomy and at autopsy in the Department of Forensic Medicine, Thanjavur Medical College, during the study period 2009-2011. The hearts thus removed were washed thoroughly in running water and preserved in a solution containing 10% formalin and thymol after numbering them from 1 - 100. The specimens were studied by gross anatomical dissection. The right atrium was opened and the Coronary Sinus ostium and Thebesian valve were identified. The presence or absence of Thebesian valve was noted. The shape of the valve whether it was semi-circular or in the form of strands or band shape was also noted. Presence or absence of fenestration in the valve were also noted.
RESULTS
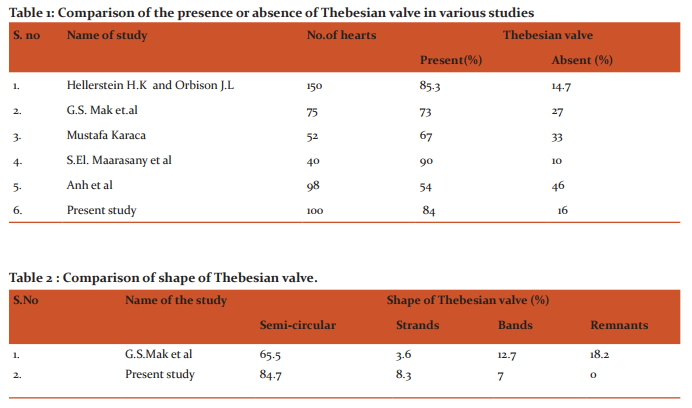
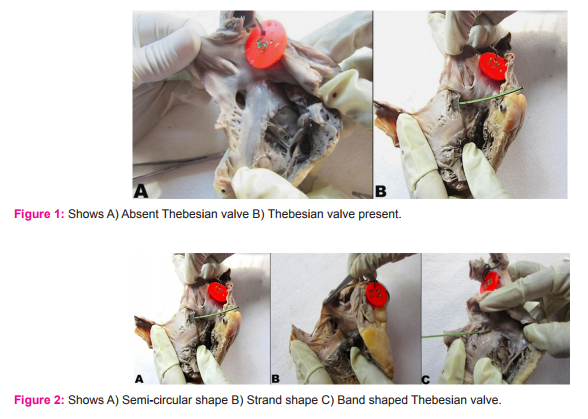
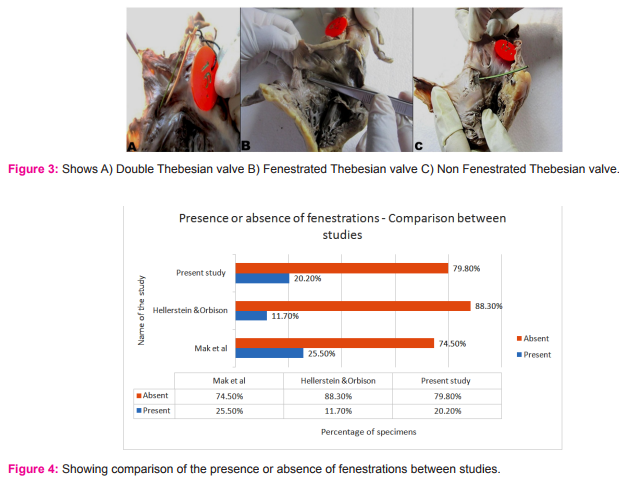
Variations in the Thebesian valve: In the present study, Thebesian valve was present in 84% of specimens and was absent in 16% of specimens(Fig. 1). Variations in the shape of Thebesian valve : The Thebesian valve was found to be semi-circular in 84.7% of specimens, in the form of strands in 8.3% specimens and in 7% of specimens it was band shaped (Fig. 2). Remnants were not found in any of the specimens. Among the 100 specimens in the present study, a rare and significant variation of double Thebesian valve was observed, constituting 1% of the total study specimens. It was semicircular in shape and was devoid of fenestrations (Fig.3A) Presence or absence of fenestrations in Thebesian valve: Usually the Thebesian valve was not fenestrated. Sometimes it may be fenestrated and it was classified based on the presence or absence of fenestrations. In this study, fenestrations in the Thebesian valve were found in 20.2% of specimens and it was absent in 79.8% of specimens (Fig.3B and 3C).
DISCUSSION
The variability of the coronary venous system has been studied by the anatomists, radiologists, electro physiologists and cardiologists. In their studies, they emphasized the views related to their own field of interest. The present study was done in 100 human cadaveric heart specimens which showed significant variations and the results were compared with those of the previous studies. Presence or absence of Thebesian valve: The Thebesian valve was present in 84% of specimens and this result correlated with the studies by various authors including Hellerstein and Orbison(12) (1951), Mak et al(2)(2009), Mustafa Karaca(13)and S.El. Maarasany et al(14). According to Anh et al(15) (2009) where the study was conducted using fibre optic technology, the thebesian valve was noted only in 54% of subjects. The lower prevalence of the presence of the valve in their study could be attributed to the limitations of the technology used in visualizing smaller valves(2). The comparison of the percentage of presence or absence of Thebesian valve by different authors and in the present study is shown in table 1. Shape of the Thebesian valve: The predominant shape of the Thebesian valve was found to be semi-circular in 84.7% of specimens and the least common shape was band shape seen in 7% of specimens in the present study. There were no remnants observed in the present study. This pattern of shape distribution correlated with that of Mak et al (2)(2009) study except for the presence of remnants in their study(Table 2). A rare variation of double crescentic Thebesian valve was seen in 1 % of specimens in the present study. According to Hellerstein H.K and Orbison J.L(12) double crescentic fold was seen in 2% of cases. C. Presence or absence of fenestrations in Thebesian valve: The majority of the Thebesian valves were devoid of fenestrations in the present study and the results correlated with those of other authors including Mak et al(2) and Hellerstein and Orbison.(12)
CONCLUSION
In the present study, the predominant shape of the Thebesian valve was found to be semi-circular and fenestrations were seen only in 20% of specimens. The rare possibility of the presence of double Thebesian valve was observed in 1% of specimen. A prominent Thebesian valve may be an under recognised problem which may interfere during cannulation procedures. They may also pose a significant threat in coronary venous lead placement done for cardiac resynchronization therapy. The knowledge of variations in the shape, number and type of the Thebesian valve may help in preventing inadvertent injury during catheterization procedures.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to the authors/editors/publishers of the journals, articles and books from where the literature of this article was reviewed and discussed.
Source of Funding: Nil
Conflict of Interest: None
References:
1. Singh J.P, Houser S, Heist E.K, Ruskin J.N, The Coronary Venous Anatomy, A Segmental Approach to Aid Cardiac Resynchronization Therapy. American College of Cardiology J; 2005; 46:48-74.
2. Mak G. S, Hill A.J, Moisiuc F, Krishnan S.C, Variations in Thebesian valve anatomy and Coronary Sinus Ostium Implications for Invasive Electrophysiology Procedures Europace J;2009;11: 1188–1192.
3. Gray’s Anatomy, The Anatomical Basis of Clinical Practice, 40th Edition, Churchill Living Stone; 2008; 964,978-82.
4. Snell R.S, Clinical Anatomy by systems, Edition, Philadelphia, Williams and Wilkins; 2007: 145-147.
5. Willerson J.T, Cohn.Jn, Cardiovascular Medicine, NewYork, Churchill Livingstone; 1995; 55-58.
6. Grant B.J.C,A, Method of Anatomy Descriptive and Deductive, 6th Edition, Baltimore: Williams and Wilkins; 1959; 555-561.
7. Skandalakis J.E, Surgical Anatomy, The Embryologic and Anatomic Basis of Modern Surgery, 1stEdition,Paschalides Medical Publication; 2004; 305-07.
8. Sinnatamby C.S, Last’s Anatomy Regional and Applied, 11th Edition, Edinburg; Churchill Living Stone; 2006:206-213.
9. Hollinshead H.W, Anatomy for Surgeons Vol-2, 2nd Edition, New York: Harperand; 1966; 112-119,124,125.
10. Habib A, Lachman N, Kevin N, Christensen and Asirvatham S.J, The Anatomy of the Coronary Sinus Venous System for the Cardiac Electrophysiologist, Europace; 2009; vol 11:v15–v21.
11. Topol E.J, Text book of interventional cardiology 5th Edition, Philadelphia , Saunders.
12. Hellerstein H.K, Orbison J.L, Anatomic Variations of the Orifice of the Human Coronary Sinus Circulation, American Heart Association.J:1951; 3:514-523.
13. Karaca , M et al, The anatomic barriers in the coronary sinus: implications for clinical procedures. J Interv Card Electrophysiol. 2005;14:89–94.
14. El-Maasarany, et al, The Coronary Sinus Conduit Function: Anatomical Study (relationship to adjacent structures). Europace J.2005,7, 475-481.
15. Anh et al, Characterization of human coronary sinus valves by direct visualization during biventricular pacemaker implantation. Pacing Clin Electrophysiol J. 2008;31:78-82.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





