IJCRR - 9(24), December, 2017
Pages: 32-34
Date of Publication: 26-Dec-2017
Print Article
Download XML Download PDF
Post Burn Ductal Carcinoma of Breast- A Rare Case Report
Author: Juhi Khanna, Nandita P. Mehta, Hansa M. Goswami
Category: Healthcare
Abstract:Objective: A 25 years old female presented to outpatient department of General Surgery of Civil Hospital with breast lump. The objective was to investigate and diagnose the case.
Material and Methods: The case was clinically examined in General surgery department. FNAC was done to diagnose swelling. The resected tissue was sent to histopathology for confirmation of the diagnosis. Histological analysis and Immunohistochemical staining was done in Pathology department.
Results: On FNAC-Infiltrating Ductal Carcinoma of breast. The patient was operated and tumor was resected. On gross examination, growth identified measures 4x3.5x2.5cm3, Cut surface
is whitish solid, well defined and firm to hard. On histological examination tumor was diagnosed to be Poorly Differentiated Ductal Carcinoma of Breast. Immuno-histo-chemical
staining revealed that the cells were positive for Estrogen receptor and Progesterone receptor. This case was to be Post burn Ductal Carcinoma of breast.
Conclusion: Malignancy arising from Burn scar is rare, Squamous cell Carcinoma is most common Burn scar neoplasia and adenocarcinoma is extremely rare. So such cases should be thoroughly examined and followed.
Keywords: Post burn, Ductal Carcinoma
DOI: 10.7324/IJCRR.2017.9246
Full Text:
INTRODUCTION:
Malignancy arising from burn scar is extremely rare. Squamous cell carcinoma is the most common, type, other types are basal cell carcinoma, malignant melanoma and rarely sacrcoma. Adenocarcinoma is extremely rare and only 4 cases have been reported till date and only one case of infiltrating Ductal carcinoma of breast has been reported. We report a care case of post burn carcinoma in a young woman.
Case Report:
A 25 years old female presented to outpatient department of General Surgery of Civil Hospital with breast lump. She had sustained thermal burns 14 years back, involving the right side of chest wall, arm and trunk. The burns where left to heal secondarily and no skin grafting was done. On examination, the burn scar was seen at right mammary area, axilla and arm. The right breast was deformed, nipple and areolar region was also unremarkable. Underneath the burn scar a large firm lump measuring4x3cm2 was seen in lower inner quadrant of right breast. The lump was adherent to chest wall but overlying skin was free. In the right axilla no lymph node where palpated. Left breast and axilla were unremarkable.
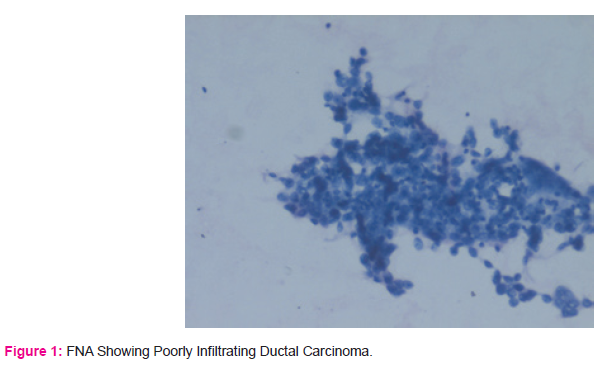
The patient was referred for fine needle aspiration (FNAC) from the lump which was performed as per standard technique. FNA from the lump yielded blood mixed aspirated which was processed as air-dried, hematoxylin and eosin stained smears where prepared.FNA smears show moderate cellularity with ductal cells arranged as irregular clusters and single cells(loss of cohesion). No myoepithelial cells seen. Ductal cells show moderated to severe nuclear atypia, enlargement, pleomorphism with evidence of occasional bizarre forms, irregular nuclear membrane and chromatin. The cytomorphology is of malignant breast lesion-Ductal carcinoma (DC)of breast-Robinsons cytological grade II.[Figure 1]
Patient underwent surgery and the specimen was received for histopathological examination.
Gross examination: Received specimen measured 22x15x2.5cm3.nipple areola was grossly not identified. One growth measuring 4x3.5x2.5cm3was identified. Cut section was whitish, solid, well defined and firm to hard in consistency. Growth is 3 cm away from superior margin,3 cm away from inferior argin,2 cm away from medial margin ,5 cm away from lateral margin,1.5 cm from base. Total 12 lymph nodes where resected size ranging from 0.3x0.2cm2 to 0.8x0.5cm2.
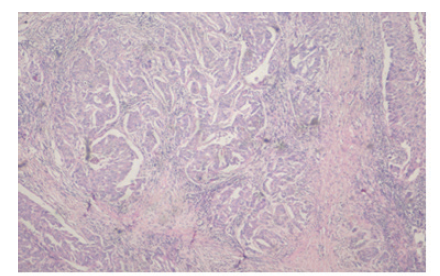
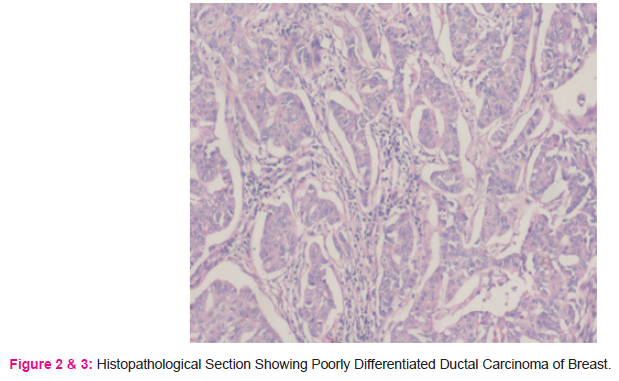
Microscopic examination: Sections showed histology of Poorly differentiated Ductal Carcinoma of Breast [Figure 2,3] with lymphovascular permeation by tumor cells. Stroma showed desmoplasia, lymphoplasmacytic infiltration, hemorrhage and necrosis. Surrounding breast showed fibrocystic changes. Section from all resected 12 lymph node does not show evidence of metastasis with histology of sinus histiocytosis. Section from resected surgical margin(superior, lateral, medial and inferior ) and base do not show evidence of tumor cells.
Conclusion: Poorly Differentiated infiltrating ductal carcinoma(IDC) of breast with tumor free resected surgical margins and base.
Modified BR grade III, TNM STAGING:T2NOMX,AJCC Stage grouping :stage IIA.[Figure 2 and 3].
Immunohistochemistry showed positivity for Estrogen receptor and progesterone receptor.
DISCUSSION:
Cancers arising in old burn scar is rare. 30years is the average latent period for development of malignancy. Most common cancer is Squamous cell carcinoma(71%),followed by basal cell carcinoma(6%),malignant melanoma(5%) and scarcomas(4%)[1]. Also rare case of malignant fibrous histocytoma, dermatofibrosarcoma protuberans, pleomorphic liposarcoma and verrucous carcinoma have been reported in post burn patient [1,2,3,4]. Adenocarcinoma in burn scar is extremely rare, total 5 cases have been reported and one case out of 5 was of IDC breast. This is the second case of IDC Breast developing in post burn.[5,6,7,8]
It has been seen that majority of burn scar carcinoma occur in burns that have not been grafted. It may also arise from chronic ulceration, but 50% patient had burn scar. The relatively avascular scar tissue with no lymphatic channels in scar may then act as immunological privileged site that allow the tumor to resist the body’s usual defenses[9,10].It is speculated that a carcinogenic toxin is produced from burned tissue and cicatrical tissue which prevents mechanism from checking the new tumor formation[11,12] .
As the breast is a modified sweat gland, DC post burn scar suggest that adnexal elements and adjacent subcutaneous tissue can also show malignant change.[7]
Promotion of rapid epithelisation and early grafting are the principles of treating initial burn.[9,10]
Conclusion:
Burn scar Malignancy is rare and Adenocarcinoma can occur in the burn scar although squamous cell carcinoma is most common. So patients need to be thoroughly examined and followed up. Skin grafting should be encouraged after burn as it might help in prevention of cancer.
References:
1.Kowal-vern,criswell BK. Burn scar neoplasm: A literature and review and statistical analysis.
2.Tanaka A, HatokoM, Tada H, Kuwahara M, lioka H, Nitsuma K Dermatofibrosarcoma protuberans arising from a burn scar of axilla. Ann Plast Surg.2004:52:423-5
3.Nishimoto S ,Matsushita T, Matsumolo K, Adachi S . A rare case of burn scar malignancy. Burns 1996;22:497-9.
4. Hunag CY, Feng CH, HSIAO YC, Chuang SS, Yang JY. Burn Scar Carcinoma J Dermatology Treat 2010,21:350-6.
5.Losanoff JE, Konard A, Sauter ER. Breast Cancer after severe burn in injury co incidence or consequence? Breast J. 2008:14:87-9.
6.Balakrishnan C, Noorily MJ Prasad VK, Wilson RP. Metastatic adenocarcinoma in a recent in a recent burn scar. Burns 1994;20:371-2.
7.Vogelin E Feichler G, Luscher NJ .Breast cancer in previously burned skin:A Post Burn skin adenexal malignancy? Burns 1997;23:366-8.
8.Neha Singh, Seena Rao and Shyama Jain J.Cytol.2013 Apr-Jun;30(2):139-141.doi:10.4103/0970-9371.112660.
9.Futrell JW Myers GH Jr.The burn scar as an immunologically privlleged site .Surg forum 1972;23:129-131
10.Dellon AL, Potvin, Chretin PB, Rogentine CN. The immunobiology of skin cancer. Plast reconstruct surg.1975;55:341-354.
11.Kennawa EC Hieger J. Carcinogenic substances and their fluorescence BMJ 1930:I:1044-6.
12.Castillo JL, Goldsmith HS burn Scar malignancy in possible depressed immune setting. Surg forum 1968:19511.
13.Bostwich J. Pendergrast WJ, Vasconez LO. Marjolinsulcer: An immunologically privileged tumor? Plast Reconstruc surg. 1876:57:66-9
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





