IJCRR - 8(12), June, 2016
Pages: 21-24
Date of Publication: 20-Jun-2016
Print Article
Download XML Download PDF
CORRELATION OF MICROALBUMINURIA AND C-REACTIVE PROTEIN AS MARKERS OF SEPSIS
Author: Shruti R. Mulgund, Subodhini A. Abhang
Category: Healthcare
Abstract:Sepsis is one of the challenges for the doctors who treat critically ill patients. Delay in diagnosis and late administration of antibiotics have been shown to increase the mortality in this cohort.
Objective: This study was done to evaluate whether microalbuminuria can be used as a marker of sepsis and also to compare with the levels of C-reactive protein (CRP a traditional marker) of patients admitted in ICU. The study was carried out in the department of Biochemistry, B.J. Medical College and Sassoon general hospitals, Pune.
Method: 50 adult patients with ICU stay of more than 24 hrs were included in the study. 50 healthy and age, sex matched controls were also included in the study. Patients with pregnancy, menstruation, anuria, macroscopic hematuria, urinary tract infection, any renal disorder and marked proteinuria were excluded from the study. Blood and spot urine samples were collected on admission and after 24 hrs. Urinary microalbumin was measured in terms of albumin creatinine ratio (ACR) and serum CRP levels were measured on ICU admission (ACR1,CRP1) and after 24 hrs (ACR2,CRP2).
Results and Conclusion: In the study we observed that there was a marked correlation between ACR1 and CRP1 (r=0.786) and also ACR2 and CRP2 (0.787). There was a significant increase in the values of both the parameters on admission as compared to controls (p< 0.001). Out of 50 patients, 35 showed increased levels of ACR and CRP levels whereas 15 showed decreased levels after 24 hrs. Patients showing decreased levels had better prognosis as compared to those showing increased levels. Thus we can conclude that ACR can be an effective marker for early detection of sepsis and can also be used to monitor the severity of the disease.
Keywords: Microalbuminuria, Critically ill, CRP, Systemic inflammation
Full Text:
INTRODUCTION
Sepsis is defined as the presence of the Systemic Inflammatory Response syndrome (SIRS) and a presumed or confirmed infection. It is a condition which is difficult to diagnose as the clinical and laboratory signs are similar to those presented in different severities of SIRS. So the mortality due to severe sepsis remains high, despite advances in its management (1). Sepsis develops when the initial appropriate host response to an infection becomes amplified, and then disregulated (2). In sepsis the endothelium has key roles in regulating vascular tone and permeability and its activation is pivotal in initiating both the inflammatory and coagulation cascades (3). Inflammatory mediators such as tumor necrosis factor, interleukins and oxygen free radicals can dramatically alter the role of the endothelium in acute diseases and in sepsis particularly (4-7). The inflammatory response is associated with an increase in the vascular permeability due to damage of the vascular endothelium. There have been many attempts to augment clinical decision making with diagnostic tests to increase sensitivity and specificity when diagnosing and treating sepsis and bacteremia. Initial studies employed fever and leukocytosis to define sepsis (8,9), though these tests were nonspecific. Subsequent studies focused on erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) to help in the diagnostic algorithm. CRP is commonly used as a marker of an acute inflammatory state. Plasma concentration of CRP has been reported to parallel the clinical course of infection, and the fall of the protein level indicating the resolution of infection (10,11). Inspite of being a traditional marker of sepsis it is not specific enough for clinicians to give their clinical judgement. Microalbuminuria (MA) is known to be a sensitive expression of the increased permeability of the systemic microcirculation (12,13). Microalbuminuria, typically defined as albumin excretion in urine of 30-300 mg/24 hrs, occurs rapidly after acute inflammatory insult and is shown to be associated with outcomes in many clinical settings, including sepsis, multiple trauma and intracranial hemorrhage (14-16). The mechanisms of development of microalbuminuria, have been extensively studied but remain elusive (16). In view of all these facts the present study was planned to estimate the serum CRP levels and urinary microalbumin levels in patients admitted in ICU having SIRS.
AIMS AND OBJECTIVES
To evaluate whether microalbumin can be used as a marker of sepsis and the correlation between the levels of microalbumin and CRP ( the inflammatory marker) on the day of admission and at 24 hrs. The aim was achieved by following objectives; estimation of serum CRP levels, estimation of urinary microalbumin and creatinine levels and their ratio. Microalbumin was expressed as the Albumin/creatinine ratio(ACR) to correct for variations in urinary flow rate (17).
MATERIAL AND METHODS
The study was carried out in department of Biochemistry, B.J. Medical College, Pune. Patients admitted in medical and surgical ICU were screened for signs of SIRS and then 50 adult patients (Age >18 yrs) with SIRS and ICU stay for more than 24 hrs from Sassoon General hospitals Pune were included in the study. 50 age and sex matched healthy controls were analyzed for comparison. On admission, the following data was collected for each patient: age; gender; date and time of admission, provisional diagnosis; co-morbid conditions such as diabetes, hypertension and chronic kidney disease. Clinical and laboratory data was collected; cultures sent and antibiotics administered within 24 hours of admission were noted. Exclusion criteria: Patients having anuria, macroscopic hematuria [confirmed with dipstick], female patients with menstruation or pregnancy were excluded. Retrospectively, patients with significant proteinuria [more than 1+ protein on dipstick] due to renal and post renal causes, for example urinary tract infection, were excluded. Pediatric patients were also excluded. The study was carried out after the approval from institutional ethical committee. Collection of serum: 5ml of intravenous blood samples of the subjects was also collected, centrifuged to separate the serum and stored at -20ºC till the analysis was done.
Estimation of CRP
Estimation of CRP was done by Turbilatex kit method. The reagent CRP-Turbilatex agglutination assay is a quantitative turbidimetric assay for measurement of CRP in human serum. (18) CRP levels were also referred as CRP1 and CRP2 i.e. patients sample collected on the day of admission and after 24 hrs of admission.
Estimation of Urinary microalbumin (ACR)
Spot urine samples were collected within 6 hours of admission and again at 24 hours, for quantification of ACR, which were referred to as ACR1 and ACR2 respectively. Urine samples were stored at -20°C till analysis. Urinary microalbumin was measured by the immunoturbidimetric method and urinary creatinine by modified kinetic Jaffe reaction .The methods covered an analytical range of 1.3–100 mg/L for microalbumin and 0-20 mg/dl for creatinine. Microalbuminuria was defined by ACR values between 30 and 299 mg/g. ACR of > 300 mg/g is considered as clinical proteinuria. ACR < 30 mg/g is normal for a healthy population.(14) However, to obtain comparable data, microalbumin was expressed as the microalbuminuria/creatinine ratio to correct for variations in urinary flow rate (17). These threshold values are well accepted for clinical use and have been predefined on the basis of published literature. Statistical analysis: Results are presented as mean ± standard deviation value and statistically analyzed by Student’s t’ test. A ‘p’ value of 0.05 or less was considered significant
RESULTS
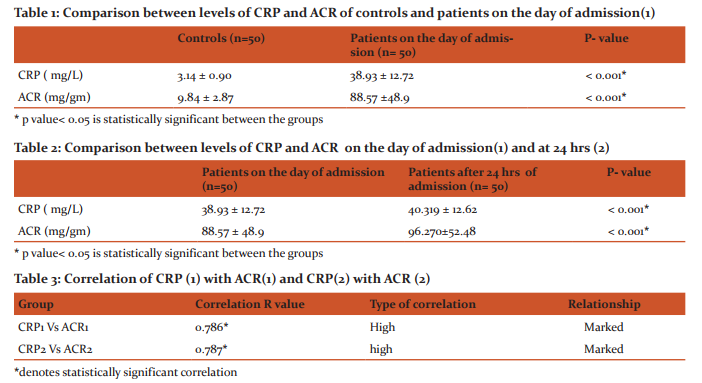
CRP has been known for a long time to be elevated in inflammatory conditions, including infection, and was used widely as an adjunctive test in sepsis and has often been used as a comparator for newer biomarkers (19). Elevated CRP levels in sepsis have been correlated with increased risk of death and organ failure (20), but in part due to the persistence of elevated levels, were unable to predict survival when evaluating CRP trends(21,22). CRP has been used successfully during initial sepsis diagnosis, but its specificity is further reduced later in the course due to persistently elevated levels(23). The present study was aimed to evaluate the levels of CRP and urinary microalbumin and also to see whether ACR can be useful in the diagnosis of sepsis. CRP was done as a marker of inflammatory response and was correlated with ACR. All fifty patients included in the study showed increased levels of CRP1 and ACR1 as compared to controls (p<0.000) (table no.1). CRP2 and ACR2 values were also more than CRP1 and ACR1 (table no.2). 35 patients out of 50 (i.e.70%) showed increased levels of CRP2 and ACR2 as compared to CRP1 and ACR1 whereas the remaining 15 out of 50 showed decreased levels. When CRP1 and ACR1 were compared a marked correlation was seen between the groups (r=0.786) (table no.3). Similarly when CRP2 and ACR2 were compared a marked correlation was seen (r=0.787) (table no.3). A marked correlation which was statistically significant was seen in both the groups.
DISCUSSION
These observed changes in the parameters indicate that sepsis itself is associated with induction of a "systemic inflammatory response", which is characterized by the release of pro-inflammatory mediators and the activation of different types of cellular elements (15,24). Endothelial cells of the microcirculatory areas are primarily involved in this response. The endothelial cells themselves may be injured by an intense inflammatory reaction, and one of the main effects of this injury is increase in endothelial permeability (15). The observed increase in CRP levels were due to an increase in the inflammatory response and thus might be the cause of increased microalbumin levels which was the result of increased systemic endothelial permeability. It was also observed that the patients having increased CRP2 and ACR2 as compared to CRP1 and ACR 1 levels had a poor prognosis, whereas patients showing decreased levels of CRP2 and ACR2 as compared to CRP1 and ACR 1 showed a better prognosis. Several studies in various groups of critically ill patients have unequivocally established microalbuminuria as a significant prognostic marker of morbidity and mortality in the ICU (25). the study of Thorevska et al (26) and Gosling et al(27) also showed similar type of results with specific cut off values on ICU admission. The rapid increase in renal permeability to plasma proteins after trauma, surgery or ischemia, which is proportional to the severity of the insult, led to the suggestion that increased renal and vascular permeability occur simultaneously, and may share common pathways during the early stages of the acute disease process (4).
CONCLUSION
It can be concluded that there is a good positive correlation between CRP and ACR. Increase in ACR levels with increased severity of the disease and decreased values of ACR observed in patients showed a better prognosis. These results suggest that ACR can be a good marker of early detection of sepsis as well as can be used to monitor the severity of the disease. A further study with a larger sample size is required to show the role of ACR as a diagnostic marker.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Angus DC, Pereira CA, Silva E : Epidemiology of severe sepsis around the world. Endocr Metab Immune Disord Drug Targets 2006,6:207-212.
2. Jonathan Cohen: The immunopathogenesis of sepsis: Nature; Vol 420, December 2002; 885-891.
3. Aird WC: The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome. Blood 2003,101: 3765-3777.
4. Omar Abid, Qinghua Sun, Kerji Sugimoto, Dany Mercan, and Jean Louis Vincent: Predictive value of microalbuminuria in medical ICU patients. Chest/120/6 December,2001;1984-1988.
5. Remick DG, Kunkel RG, Larrick JW. Acute in vivo effects of human recombinant tumour necrosis factor. Lab invest 1987; 56; 583-590.
6. McCord J. Oxygen derived free radicals. New Horiz.1993;1: 70- 76. 7. Astiz ME, Degent GE, Lin RY et al. Microvascular function and rheologic changes in hyperdynamic sepsis. Crit Care Med 1995;23: 265-271.
8. Bone RC, Balk RA, Cerra FB. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. THE ACCP/SCCM consensus conference committee. Chest.1992;101:1644-1655.
9. George E. Nelson, Vidya Mave, and Amita Gupta : Biomarkers for sepsis : A Review with special Attention to India ; Biomed Res Int.2014;2014:264351.
10. Clyne B, Olshaker JS: The C-Reactive Protein. J. Emerg Med. 1999; 17: 1019-1025.
11. Aldo Luzzani, Enrico Polati, RomoloDorizzi, AlessioRungatscher, RaffaellaPavan, Alberto Merlini: Comparison of procalcitonin and C-reactive protein as markers of sepsis. Crit Care Med. 2003 vol 31,no.6; 1737-1741.
12. Yoshiaki Terao, Masafumi Takada, Takahiro Tanabe, Yuko Ando, Makoto Fukusaki, Koji Sumikawa : Microalbuminuria is a prognostic predictor in aneurysmal subarachnoid hemorrhage : Intensive Care Med ; 2007; 33; 1000-1006.
13. Nakamura M, Onoda T, Itai K, Ohsawa M, Satou K, Sakai T, Segawa T, Sasaki J, Tonari Y, Hiramori K, Okayama A, (2004). Association between serum C-reactive protein levels and microalbuminuria: A population based cross-sectional study innorthern Iwate, Japan. Intern Med.43: 919-925.
14. Basu S, Bhattacharya M, Chaterjee TK, Chaudhari S, Todi SK, Majumdar A. Microalbuminuria: A Novel biomarker of sepsis. Indian J Crit Care Med. 2010; 14(1): 22-28.
15. De Gaudio AR, Adembri C, Grechi S, Novelli GP. Microalbuminuria an early index of impairement of glomerular permeability in post-operative septic patients. Intensive Care Med. 2000; 26(9) 1364-1368.
16. Zhongheng Zhang, Baolong Lu, Hongying Ni, Xiaoyan Sheng, NiJin: Microalbuminuria can predict the development of acute kidney injury in critically ill septic patients. J Nephrol 2013; 26(4):724-730.
17. Dezier JF, Le Reun M, Poirier JY (1988) Usefulness of the urinary albumin / creatinine ratio in screening for microalbuminuria. La PresseMedicale 17/18: 897-900.
18. Lars-Olof Hanson et al. Current opinion in infect diseases 1997; 10; 196-201 Chetana Vaishnavi. Immunology and infectious diseases 1996; 6; 144
19. Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret G-Y. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis. Critical Care Medicine. 2006;34(7):1996–2003.
20. Lobo SMA, Lobo FRM, Peres Bota D, et al. C-reactive protein levels correlate with mortality and organ failure in critically III patients. Chest. 2003;123(6):2043–2049.
21. Tschaikowsky K, Hedwig-Geissing M, Braun GG, RadespielTroeger M. Predictive value of procalcitonin, interleukin-6, and C-reactive protein for survival in postoperative patients with severe sepsis. Journal of Critical Care. 2011;26(1):54–64.
22. Tschaikowsky K, Hedwig-Geissing M, Schmidt J, Braun GG. Lipopolysaccharide-binding protein for monitoring of postoperative sepsis: complemental to C-reactive protein or redundant? PLoS ONE. 2011;6(8)e23615
23. Sakr Y, Burgett U, Nacul FE, Reinhart K, Brunkhorst F. Lipopolysaccharide binding protein in a surgical intensive care unit: a marker of sepsis?Critical Care Medicine.2008;36(7):2014–2022.
24. Parillo JE (1993) Pathogenic mechanisms of septic shock. N Engl J Med 328: 1471-1477.
25. Gopal S, Carr B, Nelson P. Does microalbuminuria predict illness severity ill patients on the intensive care unit ? A systematic review. Crit Care Med.2006;34:1805-10.
26. Thorevska N, Sabahi R, Upadya A, Manthous C, AmoatengAdjepong Y. Microalbuminuria in critically ill medical patients: Prevalence, predictors, and prognostic significance. Crit Care Med 2003;31:1075-81
27. Gosling P, Czyz J, Nitingale P, Manji M. Microalbuminuria in the intensive care unit: Clinical correlates and association with outcomes in 431 patients. Crit Care Med 2006;34(8):2158-66.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





