IJCRR - 4(15), August, 2012
Pages: 43-48
Date of Publication: 15-Aug-2012
Print Article
Download XML Download PDF
POSTPONEMENT OF ELECTIVE SURGERIES: CAUSES AND PREVENTION
Author: Ashok Sharma, Savitri Sharma, Rajan Nanda, Atul Tiwari, Usha Daria
Category: Healthcare
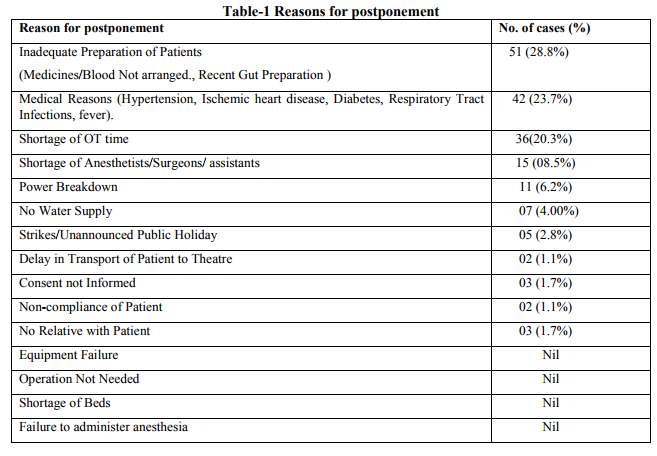
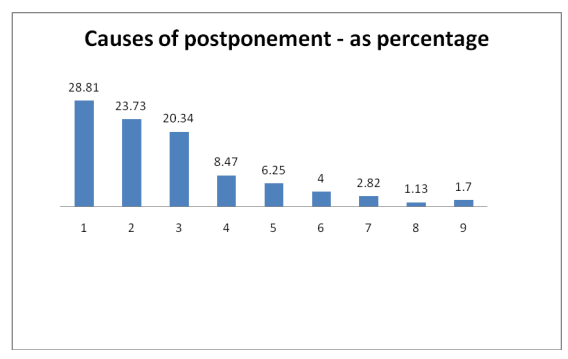
Abstract:Aims of study: To identify the factors pertaining to such postponements and to find out a workable solution to prevent postponements caused due to avoidable reasons. Postponement of elective surgery puts financial and psychological pressure on patients. Methods: This study was planned to analyse reasons for postponement of elective surgeries.Duration of study was one year from December 2007 to November 2008 Results: Total number of elective surgeries as recorded were 1245, out of these 177 were postponed. Highest number of postponed cases was due to inadequate preparation of patients 28.8%. Next main cause included multiple Medical reasons 23.7%. Another important reason was shortage of OT time (20.3%) for various reasons. Few other causes were, less number of anesthetists and surgeons15 (08%),
power cut11 (6.2%), interrupted water supply7 (4.00%), sudden declaration of holydays and strikes5 (2.8%) etc were also recorded. Conclusion: Two factors appeared\for postponement of surgeries. First were unexpected medical emergencies that constrained surgeons to postpone surgeries and second included holidays that were declared late or strikes of workers, too accounted for detention of 26.55 % of cases. It can not be controlled by any mean. Postponements due to inadequate preparation and shortage of OT time were more than 50 % (60 %) identifying these two areas to be intervened first, specifying the areas where maximum improvement is required. Still other reasons that occupy small spaces on scale of
percentage, individually, appear big when combined together (27.2 %) suggesting that small efforts are required.
Keywords: OT, NPO, postponement, surgical operations, CCU
Full Text:
INTRODUCTION
Postponement of surgical cases has been likened to adverse events that require routine monitoring because of its effect on utilization of health system resource,1,2. Furthermore, it is inconvenient and stressful for patients as it results in loss of their working days and disruption of daily life 3, 4 . Every institution strives to be recognized for its efficiency, but a high postponement rate of elective procedures keeps it difficult to accomplish 5 . However operation theatres are underutilized and lie idle many times and many patients who are called for operations from waiting list are not operated upon 6 . Planned operations that are cancelled (on that day) reflect inefficiency in management 7 . It increases theatre costs and decreases the efficiency 8 . It also causes emotional trauma to patient as well as to their families. Jhalawar hospital and medical college is 500 bedded hospital catering services to tribal and low
socioeconomic population reaching here from far flung areas. The study was conducted in order to find out the rate of postponement of the scheduled cases on an operation day in departments of surgery and orthopedics where maximum number of surgeries are performed and, to evaluate the causes of such postponements which in turn would help in figuring out workable solutions to avoid such incidences. The National Health Service (NHS), UK through its ?Modernization Agency Theatre Program? identified ?case postponement? as an incidence that occurs after patient has been notified for operation (9). An efficient surgical service should have a low rate of postponement of operations. If operations are cancelled, the operation theatre is underused, its efficiency jeopardized, waiting list increased and cost is also raised (10). It is well known fact that if resources are not properly utilized, the general population, specially the lower income groups, that depends more on public or government systems for most of their health care needs, suffers a lot. The cost of under utilized facilities and equipments also adds to cost of health care services which ultimately passes on to patients. Avoiding such postponement is an essential step to make health care system cost effective. The National Audit Office in Britain Examined five district health authorities in detail and concluded that Operation Theatres were used only to half of their capacities in spite of huge waiting lists 11. Most of the operations are postponed at 24 hour notice (12). The patients and relatives feel disappointed, frustrated and anxious(5) . Since this institute was upgraded as medical college hospital from District Hospital in 2007 so this was an effort for better functioning of this institute and to provide baseline data for future studies, specially when such study was not conducted in this area, before.
MATERIAL AND METHOD
The study period was 1 year (December 2008 to November 2009). All patients who were scheduled to undergo elective surgeries in two main operation theatres of Jhalawar hospital and medical college were included in this perspective study. Final OT lists were prepared after pre anesthetic checkups by surgeons at 2.00 P.M., a day before the surgery. Any operation that was either already scheduled or was subsequently added to the final list and than was not operated on that day was considered as postponed and was included in the study. Observations regarding causes for postponement were recorded on sheets then transferred to master chart and data analysed.
RESULTS
In duration of 1 year 1245 cases of planned General Surgery and Orthopedic surgery were studied. Out of these 1245 cases, 177 were found postponed on the day of surgery, which is 14.2% of total cases. Maximum cases postponed in this study 28.81% were due to inadequate preparation of patients prior to surgery, inadequate arrangement of medicines and / or, surgical gazettes like suture material, mesh, drains etc. In this category patients who could not arrange blood required for operation or could not follow instructions for keeping NPO were also included, Next highest number of cases 23.7% postponed were due to medical reasons like uncontrolled hypertension, sudden cardiac problems, Acute respiratory diseases and fever. 20.3% cases were postponed due to shortage of available OT time. 08.5% postponement were due unavailability of anesthetists and surgeons on the day of surgery. In contrast to other studies no case was postponed in our institution due to shortage of beds in post operative ward / CCU. One more cause that accounted in other studies i.e. operation not needed was not included in this study. Power failure (6.2%) and interrupted water supply (4%) were among other reasons for postponing surgeries. Rarely some surgeries were postponed for weird reasons like delay in transport of patients to and from OT in between two surgeries (1.7%), uninformed consent, non compliance of patient (1.1%) and/ or no relative with patient, No case was postponed in our study due to failure to administer anesthesia.
DISCUSSION
In our study we found 14.2% operations postponed. The numbers are higher than found in any other study 6,7,13. In UK 8% of scheduled operations were postponed nationally within 24 hours of surgery. (14). The most important cause for postponement in our study was Inadequate preparation of patients 51 cases (28.8%) that was quite high as compared to other studies.
Inadequate availability of medicines, surgical gazettes (mesh, suture material, prosthesis, nails, plates etc.) appeared as clear cut cause for postponing surgeries and was related with poverty in this region. Though, government helps by supplying these materials to enrolled BPL patients but many patients who were not enrolled in BPL category were also found unable to cope up with situation without financial assistance. Lack of such assistance many time resulted in postponing surgeries. We have noted that though voluntary organizations and blood banks support patients by providing stored blood for surgery but since number of thallesemia patients is a more in this south western zone of Rajasthan, requirement of repeated blood transfusions increase the demand. Additionally, requirement of blood is high in Obstetrics & Gynecology department for emergency operations and blood banks could rarely match the demand by supplying stored blood for planned surgeries. This made planned surgeries to depend on blood donation by relatives only. Popular false believe of becoming weak after a blood donation keeps illiterate relatives from donating blood and many times it becomes a reason to postpone a planned surgery. Inadequate management of some other but important medical conditions was second most important cause for postponing surgeries and accounted for 42 (23.7%) cases. Though pre anesthetic check up of all elected cases is a routine but certain medical warnings like sudden ECG changes, angina, uncontrolled blood pressure, uncontrolled and fluctuating diabetes, acute respiratory infections and fever etc forced surgeons to postpone the surgery till the emergent ailment was controlled. Non utilization of emergency operation theatre? for emergency surgeries was also a cause for shortage of operating time in main operation theatre which was avoidable simply by appointing required number of anesthetists, for each operation theatre separately. Shortage of operating time was the third most important factor, accounted for 36 (20.3%) surgeries, postponed. Lots of OT hours were found wasted due to delayed beginning of operations. Time spent in preparing cases, cleaning operation theatres, and transportation of patients to operation theatre also emerged as reasons for the same. Schedule of hospital duty hours also surfaced as one of other causes. Implementing a District hospital schedule of morning (8 am to 12 pm) and evening (5 to 6.30 pm) here, permitted OT to work only for 4 hours in morning, decreasing OT time by 2 hours as compare to other Medical Colleges. Other causes of shortage of OT time included delayed start of operations due to surgeons taking rounds of there wards first then reaching OT late for surgery. Postponement due to shortage of anesthetists, Surgeons, and paramedical assistants in our study was 15 cases (8.5%).11 and 7 cases (6.2% and 4.0%) were documented as postponed due to power failure & interrupted water supply respectively, in this study. No case was postponed due to equipment failure in our study as was seen in other studies. If we consider medical (23.7%) and late announced holidays/strikes (2.8%) as genuine reasons for postponing surgeries even than, remaining 76.16% (121 cases) were postponed for the reasons that could have been managed by administrative will. CONCLUSION The intention of study was to identify factors responsible for postponements of planned surgeries. Two, of all factors appeared as genuine for postponement of surgeries. First were unexpected medical emergencies that constrained surgeons to postpone surgeries and, second included holidays that were declared late or strikes of workers that involved OT staff too. Both of these factors combined to account for detention of 26.55 % of cases. Though, this percentage is a sounding one but it is concluded that nothing could be done to decrease this figure as it can not be controlled by any mean. Out of remaining, just two factors displayed data almost at par with previous two factors and these were, the causes related to preparation of patients for surgery (28.8%) and shortage of actual operation theatre hours for numerable reasons (20.3%). If we add both of these, popped up figure touches almost a halfway mark (49.1 %) specifying the areas where maximum improvement is required. Still other reasons (all, other than above 4) that occupy small spaces on scale of percentage, individually, appear big when combined together (27.2 %) suggesting that small efforts are required everywhere to change the scenario. To evaluate it further when analyzed the cases postponed due to avoidable reasons only, the combined share of postponements due to inadequate preparation and shortage of OT time was more than 50 % (60 %) identifying these two areas to be intervened first, in order to control postponements immediately.
References:
1. Schofield WN, Rubin GL, Piza M, Lai YY. Cancellation of operation on the day of intended surgery at a major Australian referral hospital. . MJA 2005; 182 (12): 612- 15.
2. Garg R Bhalotra AR, Bhadoria P, Gupta N and Anand R. Reasons for cancellation of cases on the day of surgery- A Prospective study. Indian j Anaesth 2009;53:35-9.
3. Tait AR Voepel- Lewis T, Munro HM, Gutstein HB and Reynolds PI.Cancellion of pediatric out patient surgery ; economic and emotional implications and for patients and their families. J Clin Anaesth 1997; 9:213-9.
4. Chamisa I. Why is surgery cancelled? A retrospective evalution.S Afr J Surg 2008; 46(3):79-81. 5. Ivarsson B, Kimblad PO, Sjoberg T, Larsson S. Pati-ent reactions to cancelled or postponed heart operations. J Nurs Manag. 2002; 10 (2): 75-81.
6. Morrissey S, Alun -Jones T, Leighton S. Why are operations cancelled? BMJ. 1989; 299:778.
7. Vinukondaiah K, Ananthakrishnan N, Ravishankar M. Audit of operation theatre utilization in general surgery. Natl Med J India, 2000; 13(3):118
8. Weinbroum AA, Ekstein P, Ezri T. Efficiency of the operating room suite. Am J Surg, 2003; 185(3):244-50
9. .National Health Services, Modernisation Agency.Theatre Programme.StepGuide to Improving Operating Theatre Performance.London: NHS, 2002. (Assessed on 25th January 2011). Available at http://www.cancerimprovement.nhs.uk.
10. Mangan JL, Walsh C, Kernohan WG, Murphy JS, Mollan RA, McMillen R et al. Total joint replacement: implication of cancelled operations for hospital costs and waiting list management. Qual Health Care, 1992; 1(1):34-7.
11. Dudley H. Empty theatres. BMJ. 1988; 297(6662):1490.
12. Koppada B, Pena M, Joshi A. Cancellation in elective orthopaedic surgery. Health Trends. 1991;23(3):114-5.
13. Lacqua MJ, Evans JT. Cancelled elective surgery: an evaluation. Am Surg, 1994; 60(11):809-11.
14. Sanjay P, Dodds A, Miller E, Arumugam PJ, Wood-ward A. Cancelled elective operations : An observa-tional study from a district general hospital. J Health Organ Manag. 2007; 21 (1): 54-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





