IJCRR - 8(12), June, 2016
Pages: 06-13
Date of Publication: 20-Jun-2016
Print Article
Download XML Download PDF
SUBSTANCE ABUSE DISORDER AMONG YOUTH: A CROSS-SECTIONAL STUDY FROM A SLUM IN MUMBAI
Author: Abhishek V. Raut
Category: Healthcare
Abstract:Background: Many of the common causes of morbidity and mortality for today and tomorrow can be prevented by reducing certain categories of behavior among youth with health promotion against tobacco use, alcohol and substance use being one of them. Objective: The objective of the study was to study the magnitude, patterns and various determinants of substance abuse disorders prevalent in the youth population in a slum of Mumbai Materials and Methods: This was a cross-sectional study conducted in Malvani slum area of Mumbai among 540 youth between 15 to 24 years of age. Two stage systematic random sampling method was used with individual household being the sampling unit. Results: 43.5% of the study participants had habit of abusing one or more than one substance. 22.6% of female participantsalso indulged in substance abuse. 28.9% of all substance abusers were consumers of alcohol. The habit of substance abuse began early, with 14% beginning before 13 years of age. Majority (78.3%) had taken to substance abuse in adolescence. Around 1/5th of the monthly wages in 40% of substance abusers was spent on substance abuse.
Conclusion: The gap between knowledge and practice was marked in case of substance abuse. Alternative approaches will have to be tapped to find out the effective strategies to prevent the youth from indulging in substance.
Keywords: Youth, Substance abuse, Tobacco, Smoking, Alcohol
Full Text:
INTRODUCTION
Youth are critical to the development of the society. They have a right, as well as duty, to be a part of this development. The international health agenda focuses on the achievement of the Millennium Development Goals (MDGs). Each of these goals is related directly or indirectly to the health and development of youth.(1) Almost half of the current global population is under the age of 25, making it a very youthful world. There are around 1.2 billion young people in the world today, and the next generation of youth, children less than 15 years of age will be soon a part of this vulnerable group swelling the population to 1.8 billion. Poverty, illiteracy, unemployment, high-risk behavior, substance abuse make a clear case for investing in young people. (2) Youth are defined as women and men age 15-24. The youth of India, representing a fifth of our population, constitutes a vital and vibrant human resource.(3)The youth population in an urban slum area is a vulnerable population with lack of access to appropriate health information. There is global concern for the rising premature morbidity and mortality due to non-communicable diseases (cardiovascular diseases, diabetes, obesity, cancers, non-communicable lung diseases etc).(4) Since non-communicable diseases(NCDs) are slowly evolving diseases, their early clinical recognition is difficult. These diseases are very closely related to changing lifestyle patterns and hence, early detection of some parameters will help in preventing the progress of disease. These parameters have been labeled as ‘risk factors’, since their presence or absence directly influences disease occurrence. A group of risk factors may influence the occurrence of more than one disease. The basis of non-communicable diseases prevention is the identification of these major common shared modifiable risk factors and their prevention and control.(5) The major risk factors for these non-communicable diseases are smoking, alcohol abuse, a sedentary lifestyle, and an unhealthy diet. As a result, 40-50% of non-communicable disease related, premature deaths are preventable.(6) Small changes or modifications made in the lifestyles of youth done today will determine the health of these youth in the future and indirectly will reflect on the development and betterment of community. (1) Apart from the obvious effects that substance abuse have either in terms of morbidity and mortality, the burden of indulgence in substance abuse to the economy of a nation is often substantial in terms of loss of productivity, increased absenteeism, loss of employment, and health care expenditures. (6) Hence we thought it prudent to conduct a study on youth population focusing on the substance abuse with an objective to study the magnitude, patterns and various determinants of substance abuse disorders prevalent in youth population, as substance abuse especially tobacco and alcohol are one of the most important shared modifiable risk factors for noncommunicable diseases prevention besides rendering the youth vulnerable for psychological dependence and antisocial activities.
MATERIALS AND METHODS
This was a cross-sectional study conducted in Malvani slum area of Mumbai. The study population included youth between 15 to 24 years of age as defined by the United Nations Population Fund (United Nations, 2009) and as has been used while describing the profile of youth in National Family Health Survey-3. (3), (7) Two stage systematic random sampling method was used with household being the sampling unit. The population of entire slum area was approximately 1,41,900. The study area was divided into six areas based on the geographical boundaries. The areas were numbered from I to VI. In stage I, by using simple random sampling method, one area (Patel compound) was selected for the study purpose with approximate population of 23720 and 4651 households. In stage II, every 10th house was selected for the study purpose. The first household was selected randomly, after which every 10th household was included in the study. The next household moving in the right-hand side direction was selected in the study when either a household was locked or when there were no eligible study participants in a household. Ethical approval was taken from the Institutional Ethical Committee while written informed consent was taken from the youth. The total numbers of households interviewed for the study purpose were 466. In the 466 households 586 potential study participants were found. 46 (7.9%) who did not consent for participation were excluded from the study and hence the sample size was 540. All the eligible population in a household between the age group of 15 to 24 years who were living in the study area for more than 6 months of age, were included in the study. Data collection instrument was designed by using standard, validated questionnaires based on National Family Health Survey 2005-06. (8) It was pilot-tested and suitably modified to meet the study objectives. It contained questions on baseline demographic information about individuals in households (age, gender, education, occupation etc), knowledge, attitudes and practices regarding patterns of substance abuse. The Alcohol Use Disorders Identification Test (AUDIT) tool was used for assessment of alcohol dependency in study participants. (9)Statistical analysis was done using Statistical Package for the Social Sciences (SPSS) 16 software. Univariate and bivariate analysis was performed to find out the variables having significant associations. A multivariate logistic regression was performed to find out the predictors for substance abuse among the youth.
RESULTS
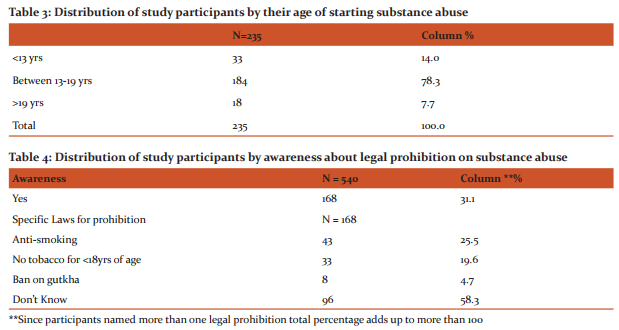
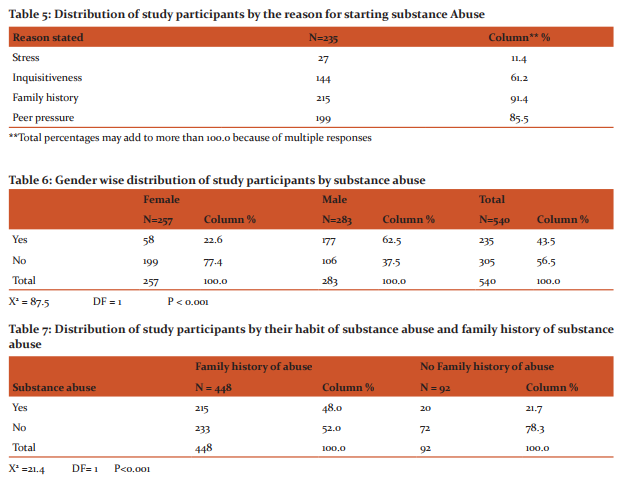
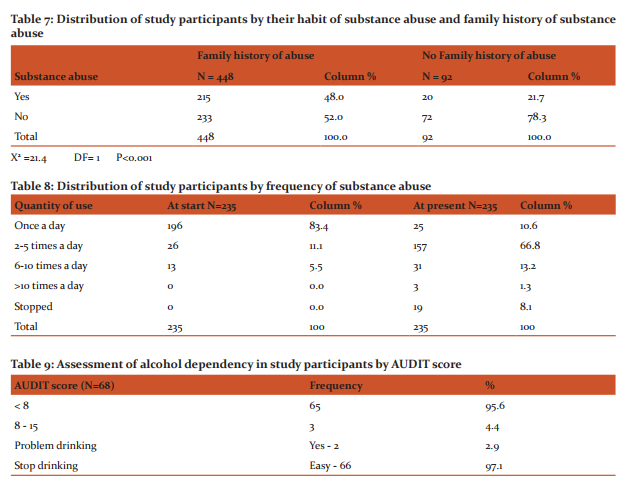
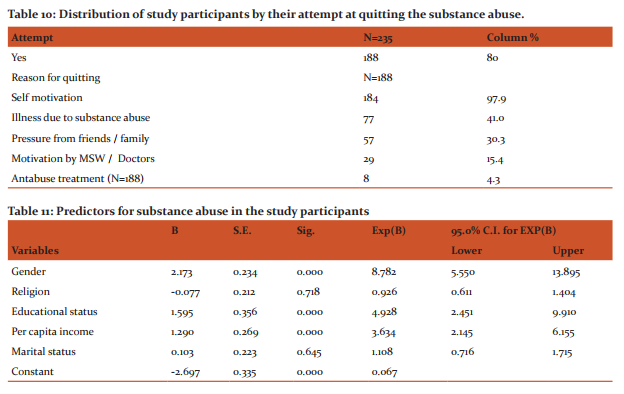
540 youth were found in the 466 household interviewed for study purpose. 37.7% of the youths were in the adolescent age group (10-19 years). 283 (52.4%) participants were males while 257 (47.6%) were females. 61.1% of the participants were Muslims, 38.1% were Hindus while other religions constituted 0.8% of study participants. 206 (38.1%) of the participants were married. 72.8% of the study participants lived in joint families, 8.7% lived in nuclear families while 18.5% of the population was living either with some of their relatives or staying at their work place e.g. ‘jarikarkhana’. 37 (6.9%) of participants were illiterate and had never gone to school. As compared to males (34.6%) more females (58.4%) had received primary education however 15.3% males had received higher education as compared to 5.1% among females. 85.6% females were unemployed while majority of males (48.4%) were involved in semiskilled jobs.81.5% of the participants belonged to the poor socio-economic class by modified B G Prasad’s socio-economic classification while only 1.1% belonged to upper high category. As shown in Table 1,43.5% of the participants had history of substance abuse. Tobacco chewed in raw form was the most common (91.5%) substance abuse seen followed by smoking (46.4%). 14.5% abused other substances like ‘bhang goli’, whitener solution, charas etc. Most of them abused more than one substance simultaneously. 98.5% of the participants said that they are aware that health hazards could be caused by such substance abuse, as is depicted in Table 2. Cancer was the most common condition named by 46.9% followed by Tuberculosis. 14.1% who had answered in affirmative for health hazard awareness couldn’t specify any particular condition or disease. 10.4% named conditions like chest pain, cough, and abdominal pain as hazards that could be caused by substance abuse. Table 3 shows the age of initiation for substance abuse, 14% of those who had a history of substance abuse had began before 13 years of age. Majority (78.3%) had taken to substance abuse in adolescence. As shown in Table 4, 31.1% of the participants said that they knew of legal prohibitions for preventing substance abuse. However 58.3% could not specify any specific law, 25.5% were aware of ban on smoking in public places. Table 5 shows the reasons stated by the study participants for initiating the habit of substance abuse.91.4% who had taken up to substance abuse had at least one family member who abused similar substance in their homes. Peer pressure was identified as the cause for starting substance abuse by 85.5% of abusers. 61.2% owed their habit of substance abuse to inquisitiveness. Table 6 shows gender wise distribution of study participants by substance abuse.22.6% of the females had substance abuse history. The association between male gender and substance abuse was found to be statistically significant, Chi square value was 87.5 with DF = 1 and P < 0.001. As shown in Table 7, the association between substance abuse by participants and substance abuse in their families was found to be statistically significant (Chi square value 21.4 with DF=1 and P<0.001).Of the 92 participants who did not have any substance abuse history at their homes, history of abuse was found in 21.7% of participants. Of those who had history of abuse at home 48% of them took up to substance abuse. Table 8 reflects the distribution of study participants by frequency of substance abuse. 83.4% of abusers started at once a day that was only 10.6% at present. There was increase in the quantity of substance abused over the period of time. 8.1% had stopped their habit of substance abuse. 40% of substance abusers spent around 1/5th of their monthly wages on substance abuse. As shown in Table 9, assessment of alcohol dependency in study participants was done by using Alcohol Use Disorders Identification Test (AUDIT)tool.28.9% of all substance abusers were consumers of alcohol. AUDIT score of 95.6% of drinkers was <8 indicating no addiction. 2.9% of the alcohol consumers thought of their drinking as a problem. 97.1% of alcohol drinkers predicted that it would be very easy for them to stop consuming alcohol. Table 10 shows the distribution of study participants by their attempt at quitting the substance abuse. Any attempt on part of the participant was taken as attempt to quit. 80% of abusers had attempted to quit their habit of substance abuse. Self-motivation was the most common reason given by 97.9% of abusers for any such attempt. 4.3% had received anti-abuse treatment at some point or other. Table 11 shows the predictors of substance abuse among study participants. We used logistic regression analysis to determine predictors of substance abuse. All variables were entered in model by using ENTER method in Statistical Package for the Social Sciences (SPSS). P-value of 0.05 was considered as significant. Omnibus test for model coefficients was significant (P-value < 0.001). Nagelkerke R Square was 0.30 indicating that independent predictor variables viz. sex, education and per capita income can explain 30 % variation in substance abuse. Hosmer Leme show goodness of fit test was non-significant (P=0.16) indicating that model fits the data. The predictors for substance abuse in study participants were gender and education and per capita income at P<0.01. Males were associated with higher substance abuse than females, having 8.7 times more likelihood of having substance abuse than females (Odds Ratio 8.7, 95% C.I. 5.5 – 13.8). Illiteracy was associated with higher prevalence of substance abuse in study participants by 4.9 times (Odds Ratio 4.9, 95% C.I. 2.4 – 9.9). Participants who belonged to poor socioeconomic class had 3.6 times higher odds of having substance abuse than who belonged to nonpoor class (Odds Ratio 3.6, 95% C.I. 2.1 – 6.1).
DISCUSSION
Tiwari Rajnarayan in a study on tobacco use and cardiovascular disease in Kerala found that only 22.5% knew about the effects of tobacco in causing cardiac problems. Most of the participants knew its harmfulness in causing cancer. Electronic and print media were more common sources of knowledge, as compared to health education provided by healthcare workers. (10) In our study we found that 62.4% named alcohol and tobacco as the liable products for substance abuse. 13.3% also named other products like ‘bhang goli’, whitener solution etc as liable products for abuse. 96.1% of participants said that friends were the source of information for awareness regarding liable products for substance abuse while 57.5% identified television as the possible source. Gajalak Shami et al in their study also found that only about half of the students reported that they had been taught about the harmful effects of tobacco use in school (11). Sinha et al reported that merely 3% students were taught in school about the harmful effects of tobacco. (12) In our study we found that 98.5% of the participants were aware of the health hazards of substance abuse. Cancer was the most common condition, named by 46.9% followed by Tuberculosis.31.1% of the participants said that they knew of legal prohibitions for preventing substance abuse. 58.3% could not specify any specific law, 25.5% were aware of ban on smoking in public places. 4.7% knew of the ban which state government had imposed on Gutkha. The gap between ‘practice’ and ‘knowledge’ was wide with 98.5% having awareness that substance abuse will lead to deleterious effects on health but still 43.5% of the participants had history of substance abuse. Chewed tobacco in raw form was the most common (91.5%) substance abused. Most of them abused more than one substance at a given time. Kotwal A et al in a study on correlates of tobacco-use pattern amongst adolescents in two schools of New Delhi, India. 2005 found that almost 42% of tobacco users started before the age of 12 years. Peer pressure, general stress, and media were important influencers. (13) In the present study it was found out that 14% of those who had a history of substance abuse had started before 13 years of age. Majority (78.3%) had taken to substance abuse in adolescence. Kadri A.M et al in a study of socio-demographic profile of substance abusers attending a de-addiction centre in Ahmedabad city found that alcohol was most commonly used (70.2%) followed by brown sugar (13.8%). 146 (26.1%) of them gave history of drug addiction in family member(s) while as many as 73.9% were the first reported abusers in their family. In a family with at least one abuser present, early age of initiation was seen in the abuser as 73.7% of them showed 20 years of age or earlier age of starting compared to the abusers not having positive family background (36.4%). (14) In our study it was found that 91.4% who had taken up to substance abuse had at least one family member who abused similar substance in their homes. Peer pressure was identified as the cause for starting substance abuse by 85.5% of abusers. 61.2% owed their habit of substance abuse to inquisitiveness. Pandey GK et al in a study on patterns of tobacco use amongst school teachers found that as high as 51.0% teachers consumed tobacco in one form or the other. Smoking was the most popular form of tobacco use (72%). Marked gender differences were noted with 73.9% male teachers hooked to tobacco habit in comparison to 13.9% of female teachers. (15) A similar study was conducted by Ali Yawar Alam investigating socio-economic-demographic determinants of tobacco use in Rawalpindi, Pakistan found out that 16.5% of the study population (33% men and 4.7% women) used tobacco on a daily basis (16). In the present study, 22.6% of the females had substance abuse history. The association between male gender and substance abuse was found to be statistically significant. In our study it was found that among the 92 participants who did not have any substance abuse history at their homes, history of abuse was found in 21.7% of participants. Of those who had history of abuse at home, 48% of the participants took up to substance abuse. The association between family history of substance abuse at home and that in participant was statistically significant. In a study on economic factor in context of health care in Madhya Pradesh the data revealed that 64% of their expenditure was on food, 12% on intoxicants, 9% on clothing and 4% on medicine (9). In our study we found that 58.7% of the participants spend from their savings while 52.8% of the participants spend from their daily wages. Family members of 91.9% of the participants had tried to stop their habit of substance abuse. 80% of abusers had attempted to quit their habit of substance abuse. Self-motivation was the most common reason given by 97.9% of abusers for any such attempt. Counseling against substance abuse by medical or paramedical professionals was seen in 15.4% of participants. 30.3% had attempted to quit substance abuse because of pressure from friends or family. 41% of the participants had attempted to quit substance abuse after some illness. 4.3% of the participants had received anti-abuse treatment at some point. 39.5% of the participants were ready to leave their habit of substance abuse in next 30 days while 16.6% were not ready to quit in next 6 months. As per the National Family Health Survey-3 data one-third of men drank alcohol, urban and rural men are about equally likely to consume alcohol. The majority of men who drank alcohol (64 percent) drank less than once a week. (4) In our study it was found that 28.9% of all substance abusers were consumers of alcohol. Alcohol Use Disorders Identification Test (AUDIT) score of 95.6% of drinkers was < 8 indicating no addiction. 2.9% of the alcohol consumers thought of their drinking as a problem. 97.1% of alcohol drinkers predicted that it would be very easy for them to stop consuming alcohol.
CONCLUSION
The gap between knowledge and practice was marked in case of substance abuse. Youth indulged in addiction in spite of knowing the ill effects. Almost half of the study participants had habit of abusing one or more than one substance. The proportion of females indulging in substance abuse was also high. The habit of substance abuse began early. Despite the efforts for creating awareness through mass-media campaigns and the legislations against sale and use of tobacco products there is a substantial gap that needs to be bridged. Alternative approaches will have to be tapped for percolating the messages to the vulnerable youth population in a slum if we intend to prevent them from indulging in substance abuse. The youth also will have to be provided with correct knowledge and enabling environment for behavior change, to stop their undesirable practices and lead them to the road to healthy life. For this further health action research to find out the effective strategies will have to be undertaken.
Limitations
Although this was a community-based cross-sectional study, as the predominant population in the study belonged to a minority community it might not be representative of the general population.
ACKNOWLEDGEMENT
• Dr S R Suryawanshi, Professor and Head, Dept. of Preventive and Social Medicine, TN Medical college, Mumbai, for guiding me to complete the research.
• Dr A P Pakhare, Assistant Professor, Dept. of Community Medicine and Family Medicine, AIIMS, Bhopal, for helping me out with the analysis.
• Author acknowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript.
The author is also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of Funding – None Conflict of interest – None
References:
1. United Nations. Guide to the Implementation of the World Programme of Action for Youth. 2006.
2. United Nations. World Youth Report 2005. Young people today, and in 2015. [Internet]. United Nations publication. 2005. Available from: http://www.un.org/esa/socdev/unyin/documents/wyr05book.pdf
3. Sulabha Parasuraman, Sunita Kishor, Shri Kant Singh and YV. A Profile of Youth in India [Internet]. Mumbai; 2009. Available from: http://www.rchiips.org/nfhs/youth_report_for_ website_18sep09.pdf
4. Alwan A, Armstrong T, Bettcher D, Branca F, Chisholm D, Ezzati M, et al. Global status report on noncommunicable diseases 2010 [Internet]. World Health Organization. 2011. Available from: http://www.who.int/nmh/publications/ncd_report_full_ en.pdf
5. World Health Organization. Preventing Chronic diseases - a vital investment: WHO Global report [Internet]. World Health Organization. 2005. Available from: http://www.who.int/chp/ chronic_disease_report/full_report.pdf?ua=1
6. D. Wayne Taylor. The Burden of Non-Communicable Diseases in India [Internet]. Hamilton, Ontario, Canada; 2010 [cited 2015 Jul 15]. Available from: http://www.cameroninstitute.com/wpcontent/uploads/2014/11/044_The-burden-of-non-communicable-dieases-in-India.2010.pdf
7. United Nations. Definition of youth [Internet]. 2014. Available from: http://www.un.org/esa/socdev/documents/youth/factsheets/youth-definition.pdf 8. International Institute for Population Sciences (IIPS) and Macro International. National Family Health Survey (NFHS-3), 2005- 06: India: Volume I. 2007.
9. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The alcohol use disorders identification test [Internet]. World Health Organization. 2001. Available from: http://whqlibdoc.who.int/ hq/2001/who_msd_msb_01.6a.pdf
10. Tiwari R. Tobacco use and cardiovascular disease. A knowledge, attitude and practice study in rural Kerala. Indian J Med Sci 2006; 60:271-6.
11. Gajalakshmi V, Asma S, Warren CW. Tobacco survey among youth in South India. Asian Pac J Cancer Prev 2004; 5:273-8.
12. Sinha D N, Gupta P C, Pednekar M. Tobacco use among students in Bihar (India). Indian J Public Health 2004; 48:111-7.
13. Kotwal A, Thakur R, Seth T. Correlates of Tobacco-use pattern amongst adolescents in two schools of New Delhi, India, Indian J Med Sci, Vol. 59, No. 6, June 2005, 243-252.
14. Kadri A. M, Bhagyalaxmi A: A Study of Socio-Demographic Profile of Substance Abusers Attending a De-Addiction Centre in Ahmedabad City. Indian Journal of Community Medicine, Vol. 28, No. 2 (2003-04 - 2003-06).
15. Pandey G K, Raut D K, Hazra S, Vajpayee A, Pandey A, Chatterjee P. Patterns of tobacco use amongst school teachers. Indian J Public Health. 2001 Jul-Sep; 45(3):82-7.
16. Alam A Y, Iqbal A, Khalif B M, Laporte R E, Ahmed A, and Nishtar S. Investigating socio-economic-demographic determinants of tobacco use in Rawalpindi, Pakistan, BMC Public Health. 2008; 8: 50. PMCID: PMC2268929.
17. A study on economic factor in context of curative health care in Saharia tribe of Madhya Pradesh: Annual report 2002, ICMR Jabalpur.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





