IJCRR - 9(22), November, 2017
Pages: 26-30
Print Article
Download XML Download PDF
Management of Non Vital Teeth with Open Apex Using Endosequence Root Repair Material, Mineral Trioxide Aggregate and Biodentin - A Case Series
Author: Dasarathan Duraivel, Abdullah Fayeez, Saravanan Poorni, Davidson Diana, Manali Ramakrishnan Srinivasan
Category: Healthcare
Abstract:Immature tooth with necrotic pulp and periapical pathosisis a major challenge and requires a tailored treatment plan. Success of an endodontic treatment in such a case requires closure of the root apex. There is a plethora of research going on in dentistry with the focus not only on the treatment rationale but also on the materials. These endeavors have led to the development of some new materials like Biodentine, Endosequence Root Repair Material, etc. which have revolutionized Endodontics. This article is a case series presenting apexification done using three different materials; Endosequence root repair material, Mineral trioxide aggregate and Biodentin.
Keywords: Bioceramic material, Immature teeth, Novel apexification
DOI: 10.7324/IJCRR.2017.9226
Full Text:
INTRODUCTION
Traumatic injuries to the teeth are most common among all facial injuries. Though this can occur in any age group, thirty percent of traumatic injuries to the dentition occurs during childhood (1). Majority of these injuries occur before the completion of root formation(2). Premature loss of vital pulp results in a frail tooth with a compromised crown-root ratio, thin dentin walls and an open apex (3). Open apex often requires pretentious effort by a dentist as roots are more susceptible to fracture and the obturating material can impinge on the periodontal tissues (4).
Management of a non-vital tooth with open apex requires stimulating the formation of a natural or an artificial apical barrier which can act as a stop for the obturating material. Apexificationis defined as “a method to induce a calcified barrier in a root with an open apex or the continued apical development of an incomplete root in teeth with necrotic pulp” (5).Considered to be the Gold standard material, Calcium Hydroxide is widely used to induce apical barrier (6-8). But the major limitation with this material is the micro leakage occurring during the formation of hard tissue barrier(which is comprised of irregularly arranged cementum-like tissue, soft tissue and calcified tissue) (9). The current approach is to form an artificial apical barrier by the placement of an apical plug using biocompatible materials.
Literature reveals a number of materials that have been used for creating an artificial apical barrier such as Tricalcium phosphate, Surgicel/amalgam, Freeze-dried bone or dentin, Biodentin and Mineral Trioxide Aggregate (MTA) (10, 11). Endo Sequence Root Repair Material(ERRM) is a novel bioceramic material commonly used for management of perforation. It is composed of calcium silicates, zirconium oxide, tantalum oxide, calcium phosphate monobasic and filler agents. It is produced with nanosphere particles that allow the material to pass into the dentinal tubules and interact with the moisture present in the dentin. This creates a mechanical bond on setting and renders the material with exceptional dimensional stability. ERRM simulates tissue fluid, phosphate buffered saline and consequently resulting in precipitation of apatite crystals depicting its bioactive nature (12-14). In a study by Jeevani et al. (15), ERRM showed better sealing ability when compared to MTA and Biodentine as furcation repair materials.But there is paucity in the literature citing the use of ERRM for apexification.
This article describes a series of cases with non-vital pulp with open apex in maxillary incisor managed successfully using Endosequence Root Repair Material, Mineral Trioxide Aggregate and Biodentin.
CASE REPORTS
CASE 1
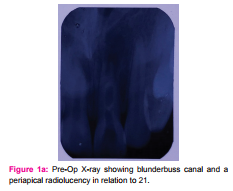
A 26 year old female patient reported to the Department of Conservative Dentistry and Endodontics, Sri Venkateshwara Dental College, Thalambur with a chief complaint of pain in her upper front tooth region for past two days. Patient gave history of dull throbbing pain for the past 6 months in the same region. Past medical and dental history were noncontributory. Clinical examination showed Ellis Davis Class IV Fracture in upper left central incisor (21). Sensibility test showed no response in 21.Radiographic examination showed blunderbuss canal and a periapical radiolucency in relation to 21. (Figure 1a)
Based on the clinical examination, sensibility test and radiographic findings, a provisional diagnosis of Ellis Davis Class IV fracture with open apex and periapical pathology was made. Apexification was planned with Mineral Trioxide Aggregate (Angelus, Andheri, Mumbai). A written consent was taken from the patient after explaining the treatment protocol.
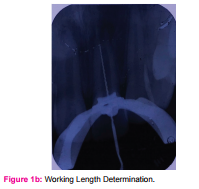
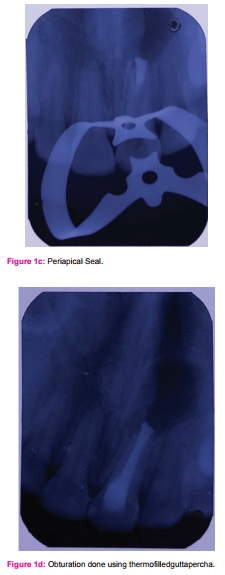
In the first visit, Access opening was done under rubber dam (Hygenic, Coltène/Whaledent, Altstätten, Switcherland) isolation using endo access bur #1 (Dentsply, Pennsylvania, United States).Canal patency was checked using a #10 K file (Mani, Brussels, Belgium)and working length was determined using Ingle’s Radiographic method (Figure 1b). Biomechanical preparation was done using K files using step back technique. Irrigation was done using 5.25 % NaOCl(Prime Dental Products Pvt. Ltd, India) and saline (Polyamp DuoFit, South Wales, Australia). Chlorhexidine (AnabondAsep-RC, Chennai, India) was used as a final irrigant. Calcium Hydroxide (Voco Calcicur, Cuxhaven, Germany) was placed using a Lentulo spiral (Mani, Brussels, Belgium) and tooth was temporized. Patient was recalled after a week. In the second visit, access cavity was reestablished, canal was irrigated copiously following the same protocol and dried with sterile paper points (Mani, Brussels, Belgium).ERRM (Brasseler, Georgia, USA) was mixed according to the manufacturer’s protocol and was carried to the access cavity using a messing gun (Mani, Brussels, Belgium) and packed to a thickness of 4 mm in the apical third using a hand plugger (Mani, Brussels, Belgium) (Figure 1c). A sterilecotton pellet was placed in the canal andthe tooth was temporized. Patient was recalled after two days.
In the subsequent visit, obturation was done using thermoplasticized guttapercha (Obtura™ Max, Algonquin, Canada) and Composite resin restoration (Magma NT) was placed to seal the access cavity (Figure 1d). Patient was recalled after a month for follow up.
CASE 2
An 18 year old male patient reported to the department with a chief complaint of pain in her upper front tooth region for past two days. Patient gave history of acute sharp pain in the same region. Past medical and dental history were noncontributory. Clinical examination showed Ellis Davis Class IV Fracture in upper left central incisor (11). Sensibility test showed no response in 11. Radiographic examination showed blunderbuss canal and a periapical radiolucency in relation to 11.
Based on the clinical examination, sensibility test and radiographic findings, a provisional diagnosis of Ellis Davis Class IV fracture with open apex and periapical pathology was made. Apexification was planned with Biodentin. The written consent was taken from the patient after explaining the treatment protocol.
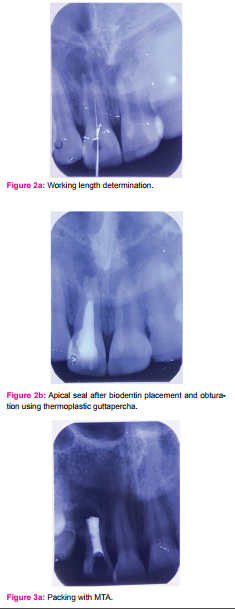
In the first visit, Access opening was done under rubber dam and Canal patency was checked as mentioned in the previous case. Working length was determined using Ingle’s Radiographic method (Figure 2a) and Biomechanical preparation was done. Calcium Hydroxide was placed using a Lentulo spiral and tooth was temporized. Patient was recalled after a week.
In the second visit, access cavity was reestablished, canal was irrigated copiously and dried with sterile paper points. Biodentin (Septodont,Saint-Maur-des-Fossés, France) was mixed according to the manufacturer’s protocol and was carried to the access cavity using a messing gun and packed to a thickness of 4 mm in the apical third using a hand plugger. A sterile cotton pellet was placed in the canal and the tooth was temporized. Patient was recalled after two days.
In the subsequent visit, obturation was done using thermoplasticized gutta-percha and Composite resin restoration was used to seal the access cavity (Figure 2b). Patient was recalled after a month for follow up.
CASE 3
A 22 year old female patient reported to the department with a chief complaint of black discolouration in her upper front tooth region for past two days. Patient gave history of traumatic injury in the same region 10 months back. Past medical and dental history were noncontributory. Clinical examination showed Ellis Davis Class IV Fracture in upper left central incisor (12). Sensibility test showed no response in 12. Radiographic examination showed blunderbuss canal and a periapical radiolucency in relation to 12.
Based on the clinical examination, sensibility test and radiographic findings, a provisional diagnosis of Ellis Davis Class IV fracture with open apex and periapical pathology was made. Apexification was planned with MTA (Angelus, Londrinas, Brazil). The written consent was taken from the patient after explaining the treatment protocol.
The same procedure was followed as done in the earlier cases; in the first visit, Access opening was done and canal patency was checked. Working length was determined using Ingle’s Radiographic method. Biomechanical preparation was done and Calcium Hydroxide was placed and tooth was temporized. Patient was recalled after a week.
In the second visit, access cavity was reestablished, canal was irrigated copiously and dried with sterile paper points. MTA was mixed according to the manufacturer’s protocol and was carried to the access cavity using a messing gun and packed to a thickness of 4 mm in the apical third using a hand plugger (Figure 3a). A sterile wet cotton pellet was placed in the canal and the tooth was temporized. Patient was recalled after two days
In the subsequent visit, obturation was done using thermoplasticized guttapercha and Composite resin restoration was used to seal the access cavity. Patient was recalled after a month for follow up.
DISCUSSION
Traumatic injury to a tooth before root development results in destruction of hertwig epithelial root sheath as it is most sensitive to inflammatory reaction. (16) This does not however mean that there is an end to deposition of hard tissue in the region of the root apex as hard tissue formation by cementoblast cells can be stimulated (17). Also the fibroblasts of the dental follicle and periodontal ligament can undergo differentiation after an injury to become hard tissue producing cells (1,18).
Apexification procedure intends to form a mineralized barrier in the root apex against which gutta- percha can be condensed in the canal space. With the passage of time many materials have been modified by research in material sciences that has evolved dentistry to prove, disprove or facilitate treatment approaches in management of cases. Practitioners need to always be aware of changes in scientific studies that occur from time to time supporting or disproving these treatment rationales.
MTA introduced by Torabinejad in the present has been exclusively used in pulp capping, pulpotomy cases, and sealing accidental perforations of the root canal (19,20), it became the material of choice for apexification therapy because of excellent biocompatibility and sealing ability (21). The mechanism of action of MTA lies in releasing calcium ions that activate cell attachment and proliferation, and at the same time, the high pH creates an antibacterial environment. But the major drawback with MTA is its long setting time and presence of toxic elements in its composition (22).
Biodentine is a new bioactive dentin substitute cement. It is avalaible in a powder-liquid system; powder composed of Tri-calcium silicate, Di-calcium silicate, Calcium carbonate and oxide, Iron oxide, Zirconium oxide. Liquid consist of Calcium chloride, Hydro soluble polymer. Biodentine has a shorter setting time of 12 minutes, as compared with that of MTA, which is 2 hours 45 minutes (23, 24). Zanini et al suggested that Biodentine is bioactive because it induces differentiation of odontoblast-like cells and increases murine pulp cell proliferation and biomineralization(25). The major disadvantage of biodentine is its high alkalinity which induces denaturing of the organic matrix (26).
EndoSequence is a novel bioceramic material. It has a working time of more than 30 minutes and a setting reaction initiated by moisture with a final set achieved in approximately 4 hours. It is composed of calcium silicates, zirconium oxide, tantalumoxide, calcium phosphate monobasic and filler agents. It contains nanosphere particles that allow the material to enter into the dentinal tubules and interact with the moisture present in the dentin. This creates a mechanical bond on setting and renders the material with exceptional dimensional stability, along with this the material has superior biocompatibility characteristics due to its high pH (12,13). Endosequence root repair material simulates tissue fluid, phosphate buffered saline and results in precipitation of apatite crystals that become larger with increasing immersion times concluding it to be bioactive (14).
The findings in this case report suggest that Endosequence Root Repair Material can be used as an alternative for MTA and biodentine. Since there is a paucity in the literature on the use of ERRM for apexification, long term follow up is required to implicate a difference among these three materials.
CONCLUSION
ERRM can be considered as a suitable alternative to other materials used in apexification procedure. Further scrutiny through clinical trials are required for comparison with other materials and to determine long term success rate.
References:
- Andreasen JO, Andreasen FM. Textbook and color atlas of traumatic injuries to the teeth, 3rdedn. Copenhagen: Munkasgaard 1994
- Moore A, Howley MF, O’Connell AC. Treatment of open apex teeth using two types of white mineral trioxide aggregate after initial dressing with calcium hydroxide in children. Dent Traumatol 2011 Jun;27(3):166-73
- Ahlawat B, Kumar A, Chaudhary N, Vijaylaxmy, Bhardwaj V. Apexification with Rapid MTA Plug Technique. Indian J.Sci.Res 2015;6(2):153-6
- Trope M. Treatment of the Immature tooth with a Non-Vital Pulp and Apical Periodontitis. Dent Clin North Am 2010 Apr;54(2):313-24
- American Association of Endodontists. Glossary of endodontic terms, 7thedn. Chicago; 2003
- Ghose LJ, Baghdad VS, Hikmat YM. Apexification of immature apices of pulpless permanent anterior teeth with calcium hydroxide. J Endod 1987;13:285-90
- Kerekes K, Heide S, Jacoben I. Follow up examination of endodontic treatment in traumatized juvenile incisors. J Endod 1980;6:744-8
- Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha; A retrospective clinical study. Endod Dent Traumatol 1992;8:45-55
- Bortoluzzi EA, Broon NJ, Bramante CM, Consolaro A, Garcia RB, Moraes IG, Bernadineli N. Mineral Trioxide Aggregate with or without Calcium Chloride in Pulpotomy. J Endod 2008, Feb;34(2):172-5
- Amandeep SU, Mandeep KB, Jagat B, Gulsheen. Apexification. DJAS 2013;1(16)
- Harbert H. One step apexification without calcium hydroxide. J Endod 1996;22:690-2
- Damas BA, Wheater MA, Bringas JS, Hoen MM. Cytotoxicity Comparison of Mineral Trioxide Aggregates and Endo Sequence Bioceramic Root Repair Materials. J Endod 2011;37(3):372-5.
- Nasseh A. The rise of bioceramics. Endodontic Practice 2009;2:17-22
- Shokouhinejad N, Nekoofar MG, Razm H, Sajadi S, Davies TE, Saghiri MA, et al. Bioactivity of Endo Sequence Root Repair Material and Bioaggregate. IntEndod J. 2012;45:1127-34
- Jeevani E, Jayaprakash T, Bolla N, Vemuri S, Sunil CR, Kalluru RS. Evaluation of sealing ability of MM-MTA, Endosquence and Biodentine as furcation repair materials: UV spectrophotometric analysis. J Conserv Dent. 2014;17(4):340-43
- Bhasker SN. Orban’s oral histology and embryology, 11thedn. St Louis:Mosby-Year Book; 1991
- Torneck CD. Effects of trauma to the developing permanent dentitiion. Dent Clin N Am 1982;26:481-504
- Andreasen JO, Ravn KK. Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surj 1972;1:235-9
- Torabinejad M, Hong Cu, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root end filling material. J Endod 1995;21:349-53
- Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of mineral trioxide aggregate when used as a root end filling material. J Endod 1993;29:591-5
- Lantz B, Persson P. Periodontal tissue reactions after root perforations in dog’s teeth: a histologic study. Odonto Revy 1967;75:209-20
- Kratchman SI. Perforation repair and one-step apexification procedure. Dent Clin North Am 2004;48:291-307
- Priyalakshmi S, Ranjan M. Review of Biodentine- a bioactive dentin substitute. IOSR Journal of dental and medical sciences 2014;13(1):13-15
- Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J. 2011;44:1081-7
- Zanini M, Sautier JM, Berdal A, Simon S. Biodentine induces immortalized murine pulp cell differentiation into odontoblast-like cells and stimulates biomineralization. Journal of Endodontics 2012;38(9):1220-6
- Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. Journal of Dental Research 2012;91(5):454-9
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





