IJCRR - 9(19), October, 2017
Pages: 37-39
Print Article
Download XML Download PDF
Pleomorphic Adenoma of Breast, Unusual in its Location
Author: Kshitija Wajekar, Silky Patel, Priti Trivedi, Dhaval Jetly
Category: Healthcare
Abstract:Aim: Pleomorphic adenoma (PA) is a common benign mixed tumor of salivary gland. It rarely involves the breast and due to limited yield of tissue samples on fine needle aspiration and core biopsies, it poses a diagnostic difficulty to the pathologist.
Case Report: Here we report a rare case, with clinical suspicion of malignancy of breast in 60 year old lady, which was diagnosed as pleomorphic adenoma on histopathology.
Discussion: PA is grossly well circumscribed and on microscopy shows both epithelial and myoepithelial cells embedded in chondromyxoid stroma. With adequate sampling, it is not difficult to diagnose this rare entity of breast on histopathology.
Conclusion: As PA mimicks malignancy, it is important to identify this benign entity in breast and prevent radical mastectomy surgery in these patients.
Keywords: Pleomorphic adenoma, Breast
Full Text:
Introduction:
Pleomorphic adenoma is also known as benign mixed tumor as it has a mixture of both epithelial and myoepithelial cells embedded in chondromyxoid stroma. It most commonly involves the salivary glands (90% parotid gland) and uncommonly palate, lip, nose, paranasal sinuses, larynx, skin (where it is known as chondroidsyringoma). It rarely occurs in breast. The first case was published in 1906 by Lecene1. Till now less than 80 cases of pleomorphic adenoma of breast have been reported in literature2. Pleomorphic adenoma of breast most commonly presents as a retroareolar mass, mimicking cancer3. As radiology is nonspecific, histopathology is essential for making a final diagnosis 4. Three cases of malignant transformation of pleomorphic adenoma (carcinoma ex-pleomorphic adenoma) have been reported by Hayes et al5.
Case Report:
A 65 year old woman presented with chief complaint of lump in left breast since one month. There was no history of pain or nipple discharge. On examination, a lump was palpated in retroareolar region measuring 1.5x1.0x1.0 cm3 . There was no nipple retraction. Contralateral breast was unremarkable on palpation. No axillary lymph nodes were palpable bilaterally. On routine investigation patient was HCV positive and hypothyroid. On mammography, left breast showed ill defined soft tissue opacity with foci of macrocalcification (Figure 1). It was reported as highly suspicious lesion for malignancy with BIRAD category IVc. Ultrasonography showed 21x18 mm sized ill defined hypoechoic lesion with internal specks of macrocalcification and adjacent parenchymal distortion. FNA showed benign ductal epithelial cells in sheets and in clusters along with lymphocytic inflammatory infiltrate on a haemorrhagic background. Final FNAC report was negative for malignancy. Subsequently patient underwent lumpectomy which was sent for frozen. Total specimen measured 6.0x5.0x3.0 cm3. On gross, breast lump with overlying nipple areola was seen. On cutting, a circumscribed tumor was identified in subareolar region measuring 1.5x1.5x1.0 cm3 having chalky white gritty cut surface (Figure 2). Grossly soft tissue resection margins were away and free from tumor. Frozen section was reported as benign breast tumor with possibility of 1) Fibroadenoma with chondroid and osseous metaplasia 2) Benign mixed tumor (Pleomorphic adenoma). The specimen was then submitted for paraffin embedding. On histopathological examination, a well circumscribed tumor comprising of both epithelial cells (arranged in tubules and cords) and myoepithelial cells embedded in chondromyxoid stroma were seen(Figure 3). Tumor showed osseous and chondroid metaplasia, ductal papilloma and collagen spherulosis like areas (Figure 4). Microscopically nipple and areola were unremarkable and all soft tissue resection margins were free of tumor. Immunohistochemically, epithelial cells were positive for CK7 and myoepithelial cells were positive for S-100, p63 and actin confirming presence of both types of cells. Final histopathological diagnosis of Pleomorphic adenoma of breast was made.
Discussion:
Pleomorphic adenoma of breast is an uncommon neoplasm. The hypothesis postulated is that breast is a modified sweat gland and it shares same embryological ectodermal layer with its counterparts of skin and salivary glands.6
As per previous reports, PA of breast commonly occurs in women and presents as a lump in retroareolar region of breast2,3,7. Only 4 cases have been reported in males8. The tumor ranges in size from 0.6 to 17.0 cm, average being 2.0 cm7. PA of breast has non-specific features on imaging so final diagnosis should be made on histopathological examination.
On histology, tumor is generally well circumscribed and consists of both epithelial and myoepithelial cells embedded in stroma. Stroma can be myxoid, chondroid, osseous or combination of any of these. Due to limited tissue yields on fine needle aspiration and core biopsy and presence of chondroid or myxoid matrix, it can be mistaken for fibroadenoma with calcification, metaplastic or mucinous carcinoma.6,9,10 In a study by Reid Nicholson et al, in all the cases of mucinous carcinoma breast, the extracellular mucin stained positively with alcian blue and was not obliterated by hyaluronidase pretreatment whereas, in PA of breast, hyaluronidase pretreatment obliterated alcian blue staining. Alcian blue staining with concomitant hyaluronidase treatment could therefore serve as a simple stain to help differentiate these two entities6. Metaplastic carcinoma can be differentiated from pleomorphic adenoma of breast by absence of myoeithelial cells and presence of frankly malignant mesenchymal component9. PA can be also confused with intraductal papilloma with osseous and chondroid differentiation, but proliferating myoepithelial cells can differentiate it from
Around 30% cases reported earlier made initial diagnosis of carcinoma due to suspicious mammographic findings11 or misdiagnosis on FNAC12and frozen sections13
PA has pseudopod like extension into adjacent tissue and is susceptible to recur. Treatment of choice is surgical excision with adequate clear margin3,14. Usually pleomorphic adenoma has indolent benign behavior but local recurrence has been reported in two cases14,15. Malignant transformation of PA is rare, with only 3 cases of carcinoma ex pleomorphic adenoma been reported till date. Pleomorphic adenoma has low metastatizing potential5.
Conclusion:
Pleomorphic adenoma of breast are rare tumors, more common in females and occur in retroareolar region. Complete surgical resection with wide margins is the treatment of choice. Since it mimicks malignancy, it is important to identify this benign entity in breast and prevent radical mastectomy surgery in these patients. Our patient on three months follow up showed no recurrence and is in good health.
Source of Funding: Nil
Conflict of Interest: No author has any competing interest.
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Address corresponds to: Dr Silky Patel, Department of Pathology, Gujarat Cancer And Research Institute, Ahmedabad(India).
Email: silky.patel92@gmail.com
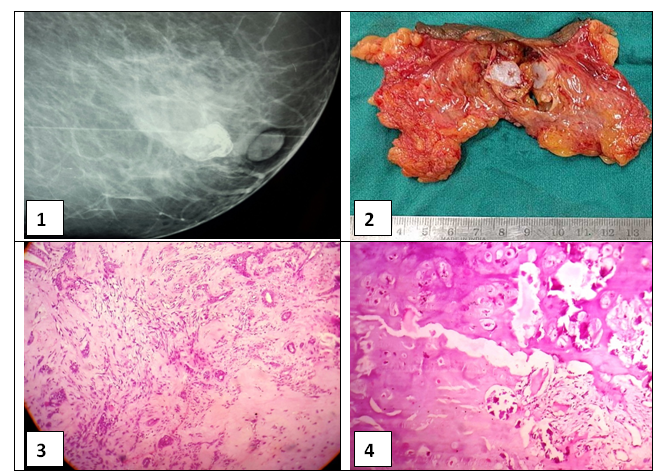
Figure 1: Retroareolar soft tissue opacity with foci of macrocalcification on mammography
Figure 2: Gross- Circumscribed tumor having chalky white cut surface
Figure 3: Epithelial cells and myoepithelial cells embedded in chondromyxoid stroma (H and E, 10x)
Figure 4: Tumor showing osseous metaplasia (H and E, 40x)
References:
1. Lecène AL. Observation d'un cas de tumeur "mixte" du sein. Revue de Chirurgie 1906; 33: 434-468.
2. Pleomorphic adenoma of the breast: a report of two cases and a literature review Yunan Han , Qingfu Zhang, Shawn Xiang Li , Liang Feng , Lei Zhan , Zhan Li1 , Xueshan Qiu2, Feng Jin , Bo Chen: Int J Clin Exp Pathol 2016;9(2):2459-2465
3. Pleomorphic Adenoma of Breast-A Case Report and Review of Literature: Nitin Leekha, Madhu Muralee, Anitha Mathews, T. R. Preethi, M. Iqbal Ahamed: Indian Journal of Surgical Oncology, June 2014, Volume 5, issue 2, pp 152-154
4. Pleomorphic adenoma of breast Iulian Radu, Ioana Petcu, Andrian P?nu??, Drago? Scripcariu, Mihaela Buna-Arvinte, Karina Bilavschi, ViorelScripcariu: Archives of clinical cases, December 2016, Volume 3, issue 4, pp 144-148
5. Carcinoma ex-pleomorphic adenoma of the breast. Report of three cases suggesting a relationship to metaplastic carcinoma of matrix-producing type. Malcolm M. Hayes, David Lesack, Christophe Girardet, Marina Del Vecchio, Vincenzo Eusebi: Virchows Archive February 2005, Volume 446, issue 2 , pp 142-149
6. Reid-Nicholson M, Bleiweiss I, Pace B, Azueta V, Jaffer S. Pleomorphic Adenoma of Breast. Archives of Pathology and Laboratory Medicine 2003;127(4):474-7.
7. Diaz NM, McDivitt RW and Wick MR. Pleomorphic adenoma of the breast: a clinicopathologic and immunohistochemical study of 10 cases. Hum Pathol 1991; 22: 1206-1214.
8. Molland JG, Morgan GJ, Walker DM and Lin BP. Pleomorphic adenoma of the parotid and breast in a male patient. Pathology 2005; 37: 263-265
9. Pleomorphic adenoma of breast - a case report and distinction with metaplastic carcinoma D Gupta, S Agrawal, N Trivedi, A Tewari: Journal of Diagnostic Pathology 2014;9(2)33-37
10. Pleomorphic Adenoma of the Breast - Surgical Pathology Criteria [Internet]. California: Stanford University School of Medicine; 2005. Available from: http://surgpathcriteria.stanford.edu/breast/pleoadbr/printable.html.
11. Sheth, M.T. , D. Hathway, and M. Petrelli., Pleomorphic adenoma("mixed tumor") of human female breast mimickin carcinoma clinico-radiologically: Cancer 1978:41:659-665.
12. Parham, D.M. and A.Evans. Pleomorphic adenoma of the breast; a potential for misdiagnosis of malignancy on fine needle aspiration(FNA). Cytopathology 1998,9:343-348
13. Chen, K.T. Pleomorphic adenoma of breast. Am J Clin Pathol.1990;93:792-794
14. John BJ, Griffiths C and Ebbs SR. Pleomorphic adenoma of the breast should be excised with a cuff of normal tissue. Breast J 2007; 13: 418-420.
15. Soreide JA, Anda O, Eriksen L, Holter J and Kjellevold KH. Pleomorphic adenoma of the human breast with local recurrence. Cancer 1988; 61: 997-1001.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





