 IJCRR
IJCRR International Journal of Current Research and Review
Welcome to IJCRR
Indexed and Abstracted in: Crossref, CAS Abstracts, Publons, Google Scholar, Open J-Gate, ROAD, Indian Citation Index (ICI), ResearchGATE, Ulrich's Periodicals Directory, WorldCat (World's largest network of library content and services)
|
S no |
Origin of peroneal artery |
Number of specimens |
Total number of specimens |
Percentage(%) |
|
1. |
From posterior tibial artery |
38 |
40 |
95 |
|
2. |
Directly from popliteal artery |
2 |
40 |
5 |
Table 2: DISTANCE OF ORIGIN OF PERONEAL ARTERY FROM THE LOWER BORDER OF POPLITEUS
|
Specimen number |
Distance in cm |
Specimen number |
Distance in cm |
|
1. |
4.8 |
21. |
5.0 |
|
2. |
6.4 |
22. |
6.8 |
|
3. |
5.4 |
23. |
4.8 |
|
4. |
5.6 |
24. |
6.4 |
|
5. |
4.5 |
25. |
5.0 |
|
6. |
5.8 |
26. |
5.5 |
|
7. |
5.8 |
27. |
6.2 |
|
8. |
6.4 |
28. |
5.8 |
|
9. |
5.4 |
29. |
6.6 |
|
10. |
5.6 |
30. |
5.4 |
|
11. |
6.6 |
31. |
4.6 |
|
12. |
5.5 |
32. |
4.4 |
|
13. |
6.4 |
33. |
5.2 |
|
14. |
5.2 |
34. |
4.8 |
|
15. |
6.4 |
35. |
4.7 |
|
16. |
7.2 |
36. |
5.4 |
|
17. |
6.8 |
37. |
6.3 |
|
18. |
5.2 |
38. |
5.2 |
|
19. |
5.6 |
39. |
6.3 |
|
20. |
6.4 |
40. |
5.5 |
The average distance of the origin of the peroneal artery from the lower border of popliteus was found to be 5.7 cm and ranging between 4.5cm to 7.2cm. The distance of origin of peroneal artery from the origin of posterior tibial artery was found to be 3.4 cm with the range of 2- 7.2cm.
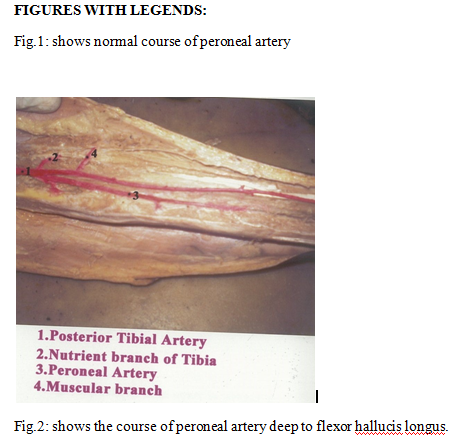
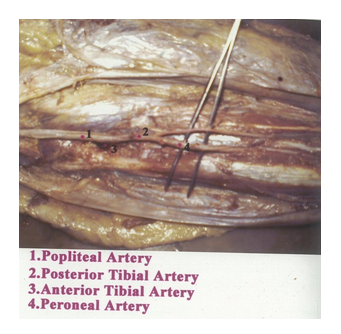
Table 3: Course of peroneal artery:(Fig.1,2,3,4)
|
S. No |
Course of peroneal artery
|
Numberof specimens (n =40) |
Percentage (%) |
|
1. |
Normal course |
34
|
85 |
|
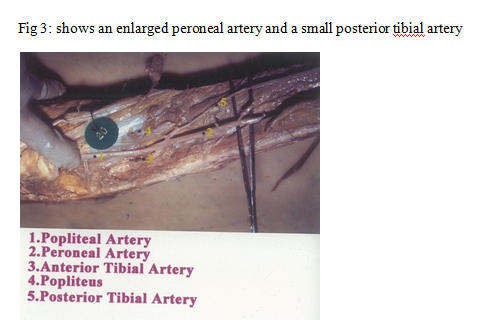
2. |
Enlarged and replaced posterior tibial artery distally
|
4 |
10 |
|
3. |
Arising from popliteal artery with absence of posterior tibial artery.
|
2 |
5 |
BRANCHES:
CIRCUMFLEX FIBULAR ARTERY:
The circumflex fibular branch arose from the peroneal artery in two of the forty specimens, amounting its incidence to 5%. In 95% of specimens, the circumflex fibular artery was a branch of posterior tibial artery.
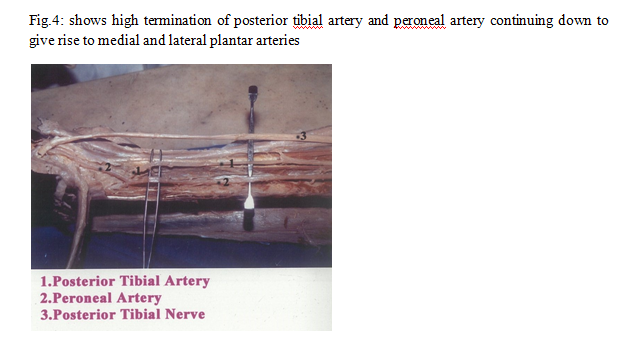
ORIGIN OF TERMINAL BRANCHES:
The terminal branches, medial and lateral plantar arteries arose from the peroneal artery in 15% of specimens (six lower limbs). In the remaining thirty four specimens (85%), the terminal branches were found to originate from the posterior tibial artery.
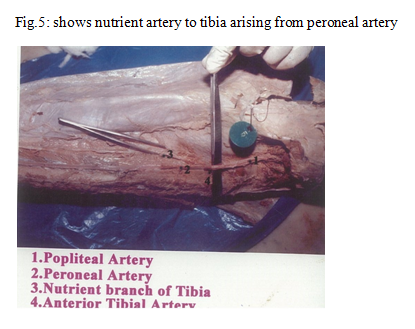
NUTRIENT ARTERY TO TIBIA(Fig.5):
In two specimens, where the posterior tibial artery was absent, the tibia received its nutrient artery from peroneal artery. In rest of the specimens, the tibia derived its nutrient artery from posterior tibial artery.
NUTRIENT ARTERY TO FIBULA(Fig.6):
The nutrient artery to fibula arose from the peroneal artery in all the specimens. It was two in number in 5 specimens (12.5%). There were three branches in two specimens (5%). There was a single nutrient artery in 33 lower limbs. The distance of the nutrient branch from the point of origin of the peroneal artery ranged between 7cm to 12cm. The origin was also measured from the styloid process of fibula and the distance varied between 13cm to 18cm.
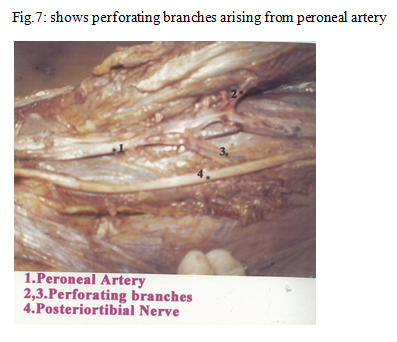
PERFORATING BRANCHES(Fig.7):
The perforators arising from the peroneal artery varied between two to three in number. The perforators reached the anterior compartment of leg. The mean + standard deviation of the distance of the perforator from the lateral malleolus was 6.6 + 9.2cm.
DISCUSSION:
The observations made in relation to the origin, course and branches was compared with those of the results of the previous authors. The majority of studies including those by J.E.Frazer (1937), J Parsons Schaffer(1953), Russell T Woodburne(1961) have shown that the peroneal artery arose from the posterior tibial artery. G J Romanes(1964) had described the division of popliteal artery into anterior tibial and peroneal artery. In the present study, the peroneal artery originated directly from the popliteal artery with absence of posterior tibial artery in 6% of specimens. Henry Gray(1858), G J Romanes and Samendra Mitra (1973) had reported incidence of trifurcation of popliteal artery. In the present study, the trifurcation of popliteal artery into posterior tibial artery, peroneal artery and anterior tibial artery was not observed in any specimen.
The distance of the peroneal artery from the origin of posterior tibial artery was compared with those of the previous studies.
Table 4: Distance of peroneal artery from the origin of posterior tibial artery.
|
S NO |
AUTHORS |
DISTANCE (CM) |
|
1. |
Russell T Woodburne(1961) |
2-3 |
|
2. |
Keith.L.Moore (2005) |
2-3 |
|
3. |
BerishStrauch et al(1993) |
3 |
|
4. |
Harold Ellis (1980) |
4 |
|
5. |
Thomas Walmsley (1934) |
5 |
|
6. |
Henry Gray( 1858) |
7-8 |
|
7. |
Present study |
2-7.2 |
The present study coincides with that of Henry Gray's observations with regards to the distance of origin of peroneal artery from the commencement of posterior tibial artery. The fibula can be used in bone grafting in avascular necrosis of hip bone, mandibular reconstruction etc. In such instances, the location and distance of nutrient artery to fibula will help surgeons during usage of fibula as a bone graft.
The perforators arsing from the peroneal artery were located predominantly in the distal two-quarters of the leg. The knowledge of perforators is essential for raising skin flaps based on these branches. Since the flaps of these regions are considered to be reliable and easy to dissect, they are preferred even in primary centres also. Sometimes these branches may be enlarged and may continue down as the dorsalis pedisartery. (Taser F).
CONCLUSION:
The revascularization procedures done as foot salvage surgeries require a detailed knowledge of the origin, course and relations of the blood vessels of lower limb. The peroneal artery being the predominant source of nutrient supply to fibula gains clinical importance especially during bone grafting procedures. The fibula is one of the bones commonly selected for bone grafting. Accessibility to these vessels is essential for the success of revascularization procedures. Hence the knowledge of the course, branching pattern and location of perforators enables surgeons and radiologists in achieving better results in surgeries or procedures involving the leg.

ACKNOWLEDGEMENT:
Authors acknowledge the immense help received from the scholars whose articles
are cited and included in references of this manuscript. The authors are
also grateful to authors / editors / publishers of all those articles, journals
and books from where the literature for this article has been reviewed and
discussed.
References:
Indexed and Abstracted in






Antiplagiarism Policy: IJCRR strongly condemn and discourage practice of plagiarism. All received manuscripts have to pass through "Plagiarism Detection Software" test before forwarding for peer review. We consider "Plagiarism is a crime"
IJCRR Code of Conduct: To achieve a high standard of publication, we adopt Good Publishing Practices (updated in 2022) which are inspired by guidelines provided by Committee on Publication Ethics (COPE), Open Access Scholarly Publishers Association (OASPA) and International Committee of Medical Journal Editors (ICMJE)
Disclaimer: International Journal of Current Research and Review (IJCRR) provides platform for researchers to publish and discuss their original research and review work. IJCRR can not be held responsible for views, opinions and written statements of researchers published in this journal.
International Journal of Current Research and Review (IJCRR) provides platform for researchers to publish and discuss their original research and review work. IJCRR can not be held responsible for views, opinions and written statements of researchers published in this journal
148, IMSR Building, Ayurvedic Layout,
Near NIT Complex, Sakkardara,
Nagpur-24, Maharashtra State, India
editor@ijcrr.com
editor.ijcrr@gmail.com
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
Copyright © 2026 IJCRR. Specialized online journals by ubijournal





