IJCRR - 4(17), September, 2012
Pages: 160-163
Date of Publication: 14-Sep-2012
Print Article
Download XML Download PDF
INFECTION RISK CONTROL IN \"COMPUTER RADIOGRAPHY IMAGING PLATE\" IN DIAGNOSTIC
RADIOLOGY DEPARTMENT
Author: Suresh Sukumar, Sushil Yadav
Category: Healthcare
Abstract:This study was carried out in order to establish whether infection control measures we?re being undertaken sufficiently on Computer Radiography Imaging plate (CRIP) used in Radio Diagnosis and Imaging Department of our medical college.CRIP is used to obtain the take compuerised radiographic image. This study involved the swabbing of a sample of CRIP used within different Areas of the department. Swabs were taken from the area on the corners and the centre of the plate. Each plate was firstly swabbed to determine the current level Of microorganism contamination (determination of baseline data) and then again after recommended cleaning. Comparisons were then made between the number of microorganisms? present (colony forming units/cm2) pre and post-cleaning at each location. All CRIP were found to be contaminated with microorganisms. Methylated spirit used in the practice of medicine, with water and soap is used to clean the CRIP was found to be significantly reduce the amount of microorganisms present. The results suggest that the All CRIP were not being cleaned sufficiently which has infection control implications for the department. In order for cross contamination to be kept to a minimum an effective infection control policy needs to be employed and this Should be to carry out regular cleaning
Keywords: Infection control; computer Radiography Imaging Plate; Hospital acquired infections; Radiology Department;
Full Text:
Introduction
Infection within healthcare has been in the news and has become a high priority recently, particularly as some infections are becoming harder to treat. The resistance of antibiotics and other antimicrobial agents have been reported on along with concerns regarding the rise of methicillin resistant Staphylococcus aureus (MRSA) (1). Staphylococcus aureus is one of the most common of all bacteria and can cause superficial infections of the skin and serious infections (2).Epidemic strains exist, which spread easily from person to person and can cause ward closure and disrupt hospital services (3). Infection control in hospitals is concerned with decontamination; this prevents microorganisms reaching a susceptible site in sufficient quantities to cause infection or potential harm to patients (4). Hospitals can become contaminated with organic matter and potentially infectious organisms and a safe environment can only be achieved by decontamination in the form of cleaning, disinfection and sterilization, breaking the chain of infection (5). A major reason for the importance of infection control is to prevent the occurrence of Nosocomial or Hospital Acquired Infections. These are infections that occur during a patient?s stay in hospital which were not present or incubating at the time of admission (2). In contrast to community acquired infections these infections usually occur as a result of pathogens taking advantage of patients whose normal defences against infection are contravened (2).
Aim
To establish whether CR plate can become contaminated with microorganisms and become a potential reservoir for cross infection and if simple, regular cleaning can significantly reduce this cross infection risk
Objectives
(1) To determine whether there is currently a detectable Presence of microorganisms on a sample of CRIP (2) To determine any presence of microorganisms after recommended cleaning (methylated spirit used in the practice of medicine with water and soap is used to clean the CRIP). (3) To evaluate the findings and make suggestions for future practice, including recommendations for re-audit.
Method
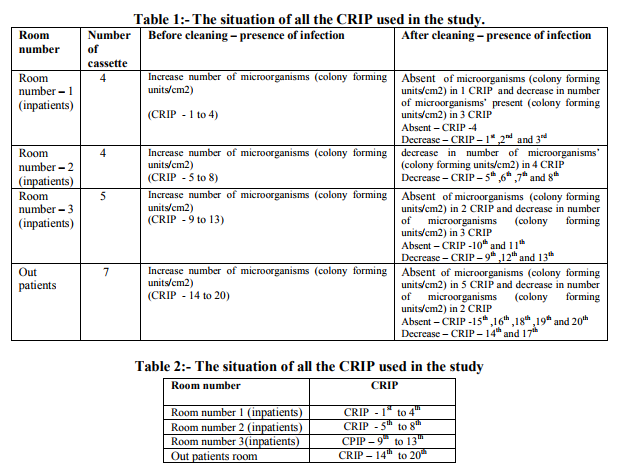
20 CRIP were swabbed, from Different areas within the Radiology department. These included general X-ray rooms for inpatients (room number 1, room number 2, and room number 3) and outpatient?s room. Randomisation of the sample was not practical, as it was necessary to ascertain data from each area. It was possible to swab all of CRIP from general X-ray rooms for in-patients (room number 1, room number 2, and rom number 3) and outpatients. Swabbing was carried out with Tryptic Soy Agar contact plates which are used to sample flat surfaces of equipment. They consist of a domed surface which is placed gently upon the area causing any microorganisms to be transferred onto the agar (10) (13). The plates were taken to the microbiology laboratory for culturing. The current level of microorganism contamination on the sample CRIP is known as baseline data. Following the collection of baseline data, each CRIP in the sample was cleaned according to recommended guidelines and swabbing was repeated. Data collected from this part of the audit was to identify a standard to compare to future practice and any future infection control carried out on CRIP After the data is collected the presence and absence of infection is mentioned as presence in CRIP and absence in CRIP.
Result
From this work all CRIP pre cleaning were contaminated with microorganisms. Table shows pre and post-cleaning results for location general X-ray rooms for in-patients (room number 1, room number 2, rom number 3) and out-patients x ray room. Post-cleaning data demonstrates that on most of the CRIP the number of colony forming units was reduced after cleaning. All plates were inspected by microbiology staff to identify the range of microorganisms present. Species of microorganisms found across the samples included most significantly Gram positive cocci in the form of Staphylococci Both coagulases positive and negative.
Discussion
Despite the fact that no Methicillin resistant strains exist was present upon the CRIP sampled, microorganism growth was found on all CRIP. This compares with other studies (6- 9) Coagulase-negative staphylococci are found as normal skin flora and include for example Staphylococci epidermis. These bacteria rarely cause infection (2, 4, 13). It has however recently been recognised that Staphylococci epidermis can be an important cause of HAIs as it produces an extracellular polysaccharide, a type of slime that enables it to adhere to plastics and metals(2,11). Staphylococcus aureus was also identified and is a coagulase Positive staphylococci. One-third of the population carry it on their skin or in their nose and throat asymptomatically (3). However, it is an important pyogenic pathogen, causing pus to form, which can cause a range of superficial infections of the skin if it penetrates the dermis such as septic spots, boils and abscesses and other more serious problems such as osteomyelitis, septicaemia and pneumonia (2,3,11, 13) It is also an important cause of HAIs, being responsible for around 40 to 50% of surgical wound infections and approximately 25% of blood stream infections(2,13), and is particularly capable of developing resistance to antibiotics. Methicillin resistant strains exist (MRSA), which are found in greatest abundance In the hospital setting as many patients receive antimicrobial therapy and are vulnerable to serious infection (2), it is also becoming recognised as an important pathogen due to its ability to colonise and cause infection of biomedical devices.1 Staphylococci released in skin scales will collect in dust and survive for long periods of time in the environment (2, 13). Swain and Flint on (7) compared the use of soap and water with alcohol wipes and phenolic disinfectant for the infection control of X-ray cassettes and concluded that all cleaning methods had a significant reduction in bacterial numbers. However, the alcohol wipes were found by the authors to be 100% effective, because of this and ease of use they were recommended as the cleaning method of choice. Another study shed doubt on The use of alcohol wipes, forensic tools were used to look for the presence of blood on seemingly clean cassettes and results suggested that if alcohol wipes were used universally to clean cassettes they are ineffective in cleaning any that are blood soiled (12). In our study use of methylated spirit used in the practice of medicine (especially for cleansing the skin before injections or before surgery) with water and soap is more effective method of cleaning the CRIP.
Conclusion
The results of the audit suggest that the CRIP were not cleaned effectively. Although the microorganisms identified are quite harmless in the majority of cases, all have the potential to be pathogenic when coming into contact with the variety of patients that present for examination in the Radiology department. This possibility is increased in cases where for example, there are damaged sites of skin such as wounds or cannula insertion sites (2). An effective infection control policy for the cleaning of CRIP should be established as an essential method to reduce cross contamination. It can be concluded that cleaning with methylated spirit used in the practice of medicine (especially for cleansing the skin before injections or before surgery) with water and soap is more effective method of cleaning CRIP can significantly reduce the number of microorganisms present and it should be carried out routinely.
ACKNOWLEDGEMENT
Author acknowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. The author is highly thankful to the referees for their very constructive, valuable suggestions and useful technical comments, which led to a significant improvement of the paper.
References:
1. National Audit Office. The Management and control of hospital Acquired infection in acute NHS trusts in England. London: National Audit Office; 2000.
2. Wilson J. In: Infection control in clinical practice. 3rd Ed.Edinburgh: Elsevier Limited; 2006.
3. Gould D, Brooker C. Applied Microbiology for Nurses. Basingstoke: Macmillan Press Limited; 2000
4. McCulloch J, editor. Infection control, science, management and practice. London: Whurr Publishers; 2000.
5. Horton R, Parker L. In: Informed infection control practice. 2nd ed. Edinburgh: Churchill Livingstone; 2002.
6. Fox M, Harvey J. An investigation of infection control for X-ray Cassettes in a Diagnostic Imaging Department. Radiography 2008; 14:306e11.
7. Swain JA, Flinton DM. X-ray cassettes: a potential crossinfection Risk? Journal of Diagnostic Radiography and Imaging 2000; 3:121e5.
8. Smith A, Lodge T. Can radiographic equipment be contaminated? By microorganisms to become a reservoir for cross Infection? Synergy 2004; Dec: 12e7.
9. Hodges A. Radiographic markers: friend or fomite? Radiologic Technology 2001; 73:183e5.
10. Booth C. Microbe monitoring. Cleanroom Technology 2006; Oct: 18e20.
11. Meers P, Sedgwick J, Worsley M. The microbiology and epidemiology of infection for health science students. London:Chapman and Hall; 1995
12. Study on blood contamination reveals disturbing results.Society of Radiographers. Available from: www.sor.org/members/snnarchive/SNRAug0 3p07.pdf; 2003 [accessed 16/04/09].
13. „„Do lead rubber aprons pose an infection risk??? Helen Boyle, Ruth M. Strudwick (2010).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





