IJCRR - 8(13), July, 2016
Pages: 17-23
Date of Publication: 12-Jul-2016
Print Article
Download XML Download PDF
ASSOCIATION OF SERUM MAGNESIUM WITH GLYCEMIC CONTROL AND INSULIN RESISTANCE IN PATIENTS WITH TYPE 2 DIABETES MELLITUS
Author: A. Velayutharaj, R. Saraswathi, R. Shivakumar, S. Saha, G. Niranjan, R. Ramesh, AR. Sreenivasan
Category: Healthcare
Abstract:Background - Context: Magnesium is an essential intracellular cation involved in many carbohydrate oxidation enzyme reactions and in glucose transporting mechanisms besides its involvement in insulin secretion, binding and activity. Body concentrations of Mg++ lowered by poor glycemic control and may predispose for diabetic complications.
Objective: To compare the levels of serum magnesium in type 2 diabetes patients with glycemic control, insulin resistance and lipid profile.
Design, setting and patients: 90 type 2 Diabetes patients who are undergoing treatment protocol were followed by a tertiary care hospital and the correlation of serum magnesium levels assessed against indicators of glycemic control and insulin resistance.
Main outcome: Since hypomagnesemia is a prime risk factor for the development of micro and macro vascular complications, this study was undertaken to find out the association, if any, between hypomagnesemia, glycemic control, lipid profile and insulin resistance.
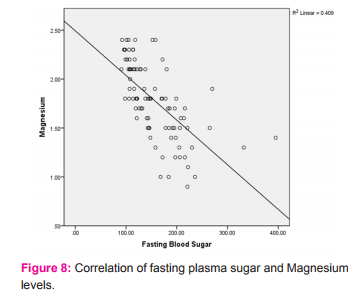
The results: A plasma Magnesium concentration of 40 (out of 90) type 2 diabetes patients in our study were below the reference range (mean 1.4\?0.22 mg %). In patients with hypomagnesemia, the mean Glycated hemoglobin was 9.1\?1.4%, which was 130% higher than the mean Glycated hemoglobin value in normomagnesemic patients (6.98\?1%) and found significant inverse correlationship between GlycatedHb levels and Serum Magnesium levels at a value of -0.713 with a p value less than 0.01 and also showed significant correlationship with HOM Air values, Fasting blood glucose, and HDL-C levels and TAG levels.
Conclusions: There was a high prevalence of hypomagnesemia in patients with T2DM reduces insulin sensitivity and may increase the risk of secondary complications. And there was a direct correlation between HDL-C and Magnesium levels; hence it is advisable to periodically monitor plasma Mg++ concentrations in diabetic patients, especially those with other risk factors such as alcoholism, familial history of CVD, etc. to reduce future complications.
Keywords: Serum magnesium, Insulin resistance, Glucose transporting mechanism, International diabetes association
Full Text:
INTRODUCTION
Diabetes mellitus (DM) is one among the major endocrine disorders that affects South Asians in general and Indians in particular because of the sedentary lifestyle, socio -economic status, ethnicity and the acquired changes in food habits of the Indians. Magnesium is the fourth most abundant cation in the body and plays an important physiological role as a cofactor in various enzymatic reactions involving energy metabolism includes carbohydrate oxidation , glucose transporting mechanism of the cell membrane and also involved in insulin secretion, binding, and activity. Chronic magnesium deficiency has been associated with the development of insulin resistance 1 Homeostatic model assessment for insulin resistance (HOMA-IR) may constitute a useful method for diagnosing insulin resistance as well as to aid the follow-up during the treatment of patients with T2DM and as an indicator of insulin resistance in diabetic patients has been the focus of attention in recent years2 . Glycosylated hemoglobin (HbA1c) measurements are the standard criteria for monitoring longterm glycemic control and reflect control for the previous 3 months. The American Diabetes Association (ADA), European Association for the Study of Diabetes (EASD), and the International Diabetes Association (IDF) recommend the use of HbA1c assay in the diagnosis of T1DM and T2DM 3 . Hitherto, very few reports are available from South India and more specifically in the region of Trichirapalli, Tamilnadu implicating magnesium levels (in serum) glycemic control, lipid profile and insulin resistance hence we conducted this study. Aim and Objectives: The study aims to estimate the levels of magnesium in serum in patients with type 2 DM and find out any correlation, if any, between magnesium levels in serum, glycemic control and Insulin resistance and lipid profile. Materials and Methods: Patients with Type 2 DM were the subjects for the study. A detailed history of the patient was taken and the duration of the disorder documented. Co morbid status and complications of Type 2 DM were also noted. The patients were divided into three groups based on their glycemic control (Glycated hemoglobin), viz., good control, fair control and poor control (n=30 each). Total number of Cases (n) = 90. After informed consent blood sample for fasting plasma glucose (FPG) and insulin (FPI) serum magnesium, lipid profile and HbA1c (EDTA sample). Biochemical parameters are analyzed in BS380 auto analyzer and HbA1c analyzed by NGSP approved method. HOMA-IR calculated by = Fasting plasma glucose (mmol/l) x Fasting plasma insulin (mlU/l) / 22.5. Inclusion criteria: 90 diabetic patients (Type 2) in three groups (n=30 each) undergoing rationale drug therapy as per the established protocol followed in a tertiary care hospital diabetic clinic. Exclusion criteria: Type 1 DM , gestational Diabetes, specific types of diabetes , patients receiving magnesium therapy, diagnosed cases of osteomalacia, patients who are on diuretic therapy, chronic alcoholics and patients with clinically diagnosed / known micro or macrovascular complications . Results: Basic demographics - The present study included 90 patients, 60 males (66.7%) and 30 females (33.3%). The mean patient’s age was 50 years. The youngest patient was 28 years old and the oldest, 82 years old (Fig.1). The sample population had normal distribution of ages.

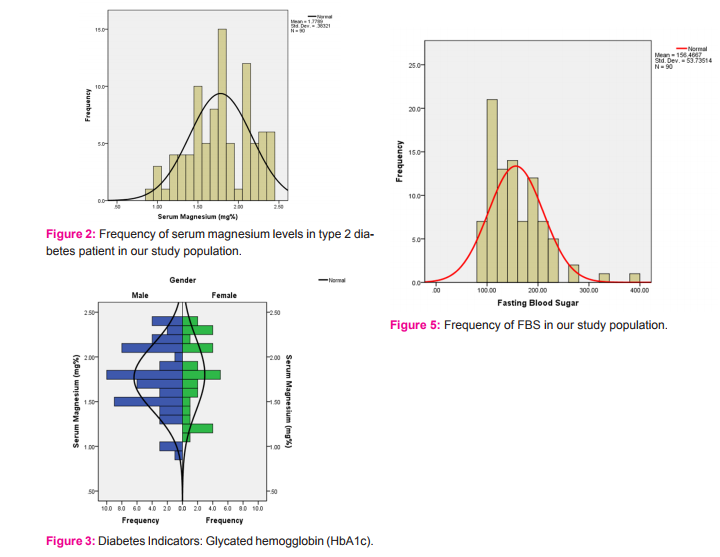
The normal serum magnesium level was considered to be between 1.7 to 2.7 mg/dl. Serum magnesium levels below 1.7 mg/dl were considered to be hypomagnesemia. In the present study, hypomagnesemia was detected in 40 patients out of 90 (44.4%) which is consistent with earlier reports of the prevalence of hypomagnesemia in diabetic patients (Fig.2). Pham et al had reported hypomagnesemia in 47.7% of non-hospitalized patients with diabetes mellitus4 . Most other studies had reported anywhere from 22 to as high as 43% prevalence.
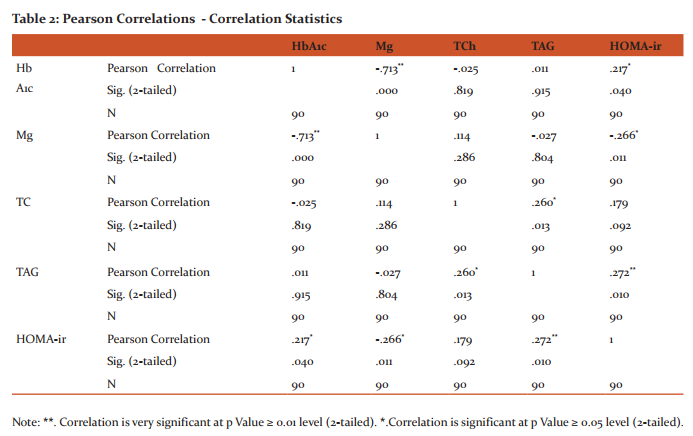
We subjected the data obtained from our study to a vigorous .spearson correlation analysis using SPSS version 19 (IBM, Chicago, 2010) and found significant and very significant correlations between serum magnesium and other studied parameters. A p Value of less than 0.05 is considered significant and P values less than 0.01 were considered very significant. The low serum magnesium value recorded was 0.9 mg%, while the highest value was 2.40 mg%. The mean serum Mg++ value obtained was 1.77 (±0.38) mg%. Frequency of serum magnesium levels with gender (Fig.3). Glycated Hemoglobin levels measured in the whole study population ranged from 4.8 to 13.3% with a mean of 7.9±1.6 In patients with hypomagnesemia, the mean Glycated Hb was 9.1±1.4%, which was 130% higher than the mean Glycated Hb value in Normomagnesemic patients (6.98±1%). Except for one patient, all the rest had elevated Glycated Hb values above 5% of HbA1c (Fig.4). The mean fasting blood glucose was 156.4±53.7mg% and had a normal distribution over the study sample population (Fig.5). Plasma Insulin levels among patients showed a wide variation in our study with a mean of 14.5 and a standard deviation of as high as 13.57. The insulin levels were used to calculate the homeostatic model assessment (HOMA) indices that quantify Insulin resistance and beta cell function using the following formula: HOMA IR = Fasting Plasma Glucose (mg/dl) X Fasting Plasma Insulin (mu/L) / 22.5 A mean HOMA IR value of 5.4±5.1 mg/dL was obtained from our results (Fig.6) When Plasma Insulin was taken into consideration along with Glycated Hb and Serum Mg++, the correlation was strengthened by a factor of 12%). When HDL levels were correlated with Serum Magnesium, significant direct correlationship was obtained (Fig.10)
DISCUSSION
Hypomagnesemia is an important electrolyte abnormality observed in patients with type2diabetes mellitus. Magnesium depletion is described as the most under diagnosed electrolyte abnormality in current medical practice5 . In fact, the intracellular magnesium deficiency appears to be associated with an impaired function of several enzymes involved in glucose metabolism, which need high energy phosphate bonds and thus require Mg as a cofactor6 and this may lead to an impairment in insulin action and worsening of insulin resistance in diabetic and hypertensive patients 7 . A decreased magnesium status contributes to the development of insulin resistance, which in turn attenuates magnesium uptake in insulin-sensitive tissues. Moreover, low serum magnesium is a strong, independent predictor of the development of type 2 diabetes. In the USA, it has been established that 25 to 39 % of outpatient diabetics have low concentrations of serum Magnesium and several studies have shown lower serum concentrations in type 2 diabetics as compared to healthy controls. The results from the Atherosclerosis Risk in Communities (ARIC) study indicate low serum Magnesium to be a strong, independent predictor of the development of type 2 diabetes8 . Similar to findings from other countries in Europe, Asia and North America 9,10, the mean plasma Magnesium concentration was significantly lower ( overall ) in our study population of overt diabetes. In the present study, the significant correlation between HOMA IR and serum magnesium levels confirms the strong relationship with Insulin resistance (p< 0.05). The striking finding in this population was the high correlation of low plasma magnesium concentrations with high glycated Hb levels among the diabetic subjects. A plasma magnesium concentration of 40 (out of 90) diabetics in our study were below the reference range (mean 1.4±0.22 mg %), a prevalence of low magnesium status that is similar to that reported in type 2 diabetics from outpatient clinics elsewhere11. Senthil et al observed that hypomagnesemia was present in both controlled and uncontrolled diabetic patients12. Magnesium depletion has a negative impact on glucose homeostasis and insulin sensitivity in diabetics as well as on the evolution of complications such as retinopathy, thrombosis and hypertension13. Studies have shown that oral supplementation of magnesium chloride improves insulin sensitivity and glucose homeostasis 14 In human type 2 diabetics, Sheehan (1991) 15 found a significant inverse correlation between serum Mg and hypertriglyceridemia. In our study, there has been a strong positive correlationship between serum Mg++ levels and HDL levels and negative correlation with triacylglycerol levels when taken together attests to the importance of hypomagnesaemia in overall development of metabolic syndrome and future complications. And studies have shown that there is a direct and significant correlation between HbA1c and cholesterol, triglycerides, LDL-C & VLDL-C and inverse correlation with HDL-C16,17. Increased levels of total cholesterol, triglycerides with Hypomagnesemia are responsible for micro- and macrovascular complications in diabetes 18. And in diabetic patients with micro vascular complications had poorer glycemic control than patients without micro vascular complications19. And it is important to note that dietary intake of magnesium from food plus supplements has been associated with a decreased risk for metabolic syndrome, obesity or overweight, elevated blood pressure, and reduced HDL-cholesterol and with lower odds ratios with dietary supplements for elevated HbA1c, increased waist circumference & C-reactive protein.20
CONCLUSIONS
There was a high prevalence of hypomagnesaemia in patients with T2DM in our study population. Hypomagnesemia had shown a significant correlation with age, gender, Glycemic control, HOMA IR, triglycerides and HDL cholesterol in our study. Because of a decrease in magnesium levels reduces insulin sensitivity and may influence the risk of secondary complications, it is advisable in clinical practice to periodically monitor plasma magnesium in diabetic patients, especially those with other associated risk factors such as alcoholism, familial history of CVD, etc. If plasma Magnesium is low, an intervention to increase dietary intakes may be advisable in patients with DM and therapeutic for the prevention of future sequelae due to T2DM.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. And authors here by declared that no conflict of interest.


References:
1. Chaudhary DP, Sharma R, Bansal DD. Implications of magnesium deficiency in Type 2 Diabetes. Biol Trace Elem Res 2010; May: 119 – 29.
2. Akira Katsuki, MD Yasuhiro Sumida, MD Esteban C. Gabazza, Shuichi Murashima Masahiko Furuta, Rika Araki-Sasaki, Yasuko Hori, Yutaka Yano. Homeostasis Model Assessment Is a Reliable Indicator of Insulin Resistance During Follow-up of Patients With Type 2 Diabetes; Diabetes Care February 2001 vol. 24 no. 2 362-65.
3. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care. Jul 2009; 32(7):1327-34.
4. Pham, P.C., P.M. Pham, P.A. Pham, S.V. Pham, H.V. Pham and J.M. Miller, 2005. Lower serum magnesium levels are associated with more rapid decline of renal function in patients with diabetes mellitus type 2. Clin. Nephrol., 63(6): 429-36.
5. Paul Marino: Fluid and electrolyte disorders– Magnesium. The ICU Book, 2nd ed., Philadelphia, Lippincott, Williams and Wilkins 2004; 660-72.
6. Rosolova H, Mayer O, Jr. and Reaven G (1997) Effect of variations in plasma magnesium concentration on resistance to insulin-mediated glucose disposal in nondiabetic subjects. J Clin Endocrinol Metab 82, 3783-85.
7. Paolisso G and Barbagallo M (1997) Hypertension, diabetes mellitus, and insulin resistance: the role of intracellular magnesium. Am J Hypertens 10, 346-55.
8. Kao WH, Folsom AR, Nieto FJ, Mo JP, Watson RL and Brancati FL (1999) Serum and dietary magnesium and the risk for type 2 diabetes mellitus: the Atherosclerosis Risk in Communities Study. Arch Intern Med 159, 2151-59.
9. Nadler JL, Malayan S, Luong H, Shaw S, Natarajan RD, Rude RK. Intracellular free magnesium deficiency plays a key role in increased platelet reactivity in type II diabetes mellitus. Diabetes Care 1992;15:835–41
10. Ma J, Folsom AR, Melnick SL, Eckfeldt JH, Sharrett AR, Nabulsi AA, et al. Associations of serum and dietary magnesium with cardiovascular disease, hypertension, diabetes, insulin, and carotid arterial wall thickness: the ARIC study. Atherosclerosis Risk in Communities Study. J Clin Epidemiol 1995; 48:927–40.
11. Nadler JL, Rude RK. Disorders of magnesium metabolism. Endocrinol Metab Clin North Am 1995; 24:623–41.
12. Senthil Manikandan Thirumanilayur Jayaraman, Kannan Rajendran, Prasanna Karthik Suthakaran, Lal Devayani Vasudevan Nair, Lokesh Rajaram, Rajiv Gnanasekar, Rajendran Karuthodiyil.Study on serum magnesium levels and glycemic status in newly detected type 2 diabetes patients. Int J Adv Med. 2016; 3(1): 11-14
13. Mather HM, Levin GE, Nisbet JA. Hypomagnesemia and ischemic-heart-disease in diabetes. Diabetes Care 1982; 5:452–3.
14. Martha Rodriguez Moran, Fernando Guerrero –Romero .Diabetes care vol.26:4.April 2003 15. Sheehan JP (1991) Magnesium deficiency and diabetes mellitus. Magnes Trace Elem 10, 215-19.
16. Jain Meenu , Jadeja Jayendrasinh M , Mehta Neeta. Correlation between HbA1c Values And Lipid Profile In Type 2 Diabetes Mellitus. International Journal of Basic and Applied Physiology . 2013;Vol. 2 Issue 1;47-50
17. Netravathi Sajjan et al. A study of serum magnesium and dyslipidemia in type 2 diabetes mellitus patients. International Journal of Clinical Biochemistry and Research 2016;3(1):36-41.
18. Asha S Khubchandani*, Hiren Sanghani**Study of Serum Magnesium and HbA1C in Diabetic Patients along with Changes in their Lipid Profiles. Indian Journal of Clinical Practice, Vol. 23, No. 11, April 2013
19. Ramachandra Prabhu .H .D1 , Sruthi Kunche2 . Study of Serum Magnesium and HbA1c in Type 2 Diabetes Mellitus Patients .International Journal of Science and Research (IJSR).2013; Volume 4 Issue 6, June 2015 (2521-24).
20. Papanikolaou Y, Brooks J, Reider C, Fulgoni VL (2014) Dietary Magnesium Usual Intake is Associated with Favorable Diabetes-Related Physiological Outcomes and Reduced Risk of Metabolic Syndrome: An NHANES 2001-2010 Analysis. J Hum Nutr Food Sci 2(3): 1038.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





