IJCRR - 9(16), August, 2017
Pages: 01-05
Print Article
Download XML Download PDF
A Study on Awareness of Maternal and Child Health Care Schemes under National Health Mission in Majuli, Assam
Author: Bornali Dutta, Manash Pratim Barman
Category: General Sciences
Abstract:Aim: In this paper an attempt has been made to accesses the level of awareness on maternal and child health care schemes among women of reproductive age and to examine the association between different socio-demographic factors and awareness level of the respondents.
Methodology: Data are collected using cluster sampling method. Statistical significance is tested using Chi-square test for independence of attributes and significance level is considered at p- value < 0.05.
Results: Caste of the respondents, order of birth of the children and road communication of the study area has significant association with the awareness level.
Conclusion: Efforts are needed to increase awareness level of the reproductive women in the rural areas like Majuli regarding various free entitlements of NRHM
Keywords: NRHM, Majuli, JSSK, cluster sampling, Reproductive women
DOI: 10.7324/IJCRR.2017.9161
Full Text:
Introduction:
In many parts of India, especially in rural areas, the main role assigned to women is that of child bearer. Thus, pregnancy is one of the most important events in the life of Indian women. Pregnancy –related complications are among the leading causes of death and disability for women age 15-49 years in the developing countries including India [4]. Most of the maternal deaths are preventable with good antenatal care, timely identification and referral of pregnant women with complications of pregnancy and timely provision of emergency obstetric care [1]. Therefore, India government introduced the national population policy (NPP-2000) with defined goal to increase institutional delivery by 80.0%, safe delivery by 100% and reducing Maternal Mortality Rate (MMR) by 100 per 1,00,000 live births[1]. The crucial importance of maternal health is underscored by the 5th goal of the United Nations Millennium Development Goals (MDG) which is aiming at improving maternal health. Millennium Development Goal-5 aims to reduced the Maternal Mortality Rate (MMR) 109 per 1, 00,000 live births by 2015[4]. India has made considerable progress towards the reduction of Maternal Mortality Ratio (MMR) and Infant Mortality Rate (IMR), but the current pace of decline is not sufficient. According to Millennium Development Goal - 2015 report, Maternal Mortality Rate (MMR) in India is 140 per 1, 00,000 live births and the state of Assam shows worst performance in reducing Maternal Mortality Rate (MMR). Still Maternal Mortality Rate (MMR) is highest in Assam at 300 per 1, 00,000 live births [4]. To achieve the Millennium Development Goals (MDG), Ministry of Health and family Welfare, Govt of India launched a nationwide initiative - National Rural Health Mission (NRHM) in 2005 and National Urban Health Mission (NUHM) in 2013 and which is popularly known as National Health Mission (NHM). Under National Health Mission (NHM) Govt. of India as well as our state government Assam introduced various schemes related to maternal and child health care. The central government implemented Janani Shishu Suraksha Karyakram (JSSK) and Janani Suraksha Yojna (JSY) schemes and our state government Assam also implemented various schemes: Majoni, Mamoni, Mamata in order to improve maternal and child health care. However, the key for the successful implementations of these schemes is the level of awareness among the beneficiaries. Awareness regarding various maternal and child health care schemes among the reproductive women is not much studied in Assam. With this background the present study is conducted to assess the level of awareness on maternal and child health care schemes among the women in the reproductive age in Kamalabari block of Majuli district, Assam.
Description of the Study Area:
The researcher collected data from Kamalabari block under Majuli district. Majuli is the world's largest river island and it is a newly announced district by the Assam government.
It is a flood affected area. Due to flood and erosion, the transport and communication system of Majuli is not good. Cultivation is the main occupation of the villagers. Handloom is a major occupation among the women of the villages. The island Majuli has been the hub of Assamese neo-vaishnavite culture, initiated around 15th century by the revered Assamese saint Srimanta Sankardev and his disciple Madhavdev. Many satras or monasteries constructed by the saint still survive and represent the colorful Assamese culture. The Samuguri Satra is famous for the mask making in India.
Methodology:
The design of the study is cross sectional and it is based on household investigation. The study is conducted in the Kamalabari block of Majuli District of Assam during 2016. Reproductive women residing in the study area during the study period constituted the study subjects. The researcher set inclusion and exclusion criteria for the study subjects to be included in the sample. The inclusion criteria are: (i) women in the reproductive age group (ii) the women who have children in the last three years. The exclusion criterion is: (i) the women who are not present in the study area during the study time. In the present study the sample size is 216; which is reasonable as WHO (World Health Organization, 2005) developed a 30 by 7 cluster sampling method for conducting similar type of study [6]. In this study, the Kamalabari block of Majuli district is selected randomly. In the selected block, 12 villages are selected by using probability proportional to size sampling method. Again from each of 12 selected villages, 18 women satisfying inclusion criteria are selected using systematic sampling method in the survey. During the survey, local ASHA helped in locating the houses. In the survey, data on awareness about different maternal and child health care schemes of NRHM are collected. The response is recorded into three categories viz, spontaneously answered, answered after probing and no awareness. If the respondent spontaneously answered about the facility; it is put in the spontaneously answered category and if the respondents answered any facility after recall by the investigator then it is put into answered after probing category and the respondent who are unable to answer by probing and spontaneously; it is put into no awareness about the facility.
Socio-economic status of the study subjects are collected by using instrument developed by Parasuram S.et al [3]. All the data are analyzed in SPSS, version 17.0 software. Statistical significance are tested using Chi-square test for independence of attribute and significance level is considered at p- value <0.05.
Key Findings:
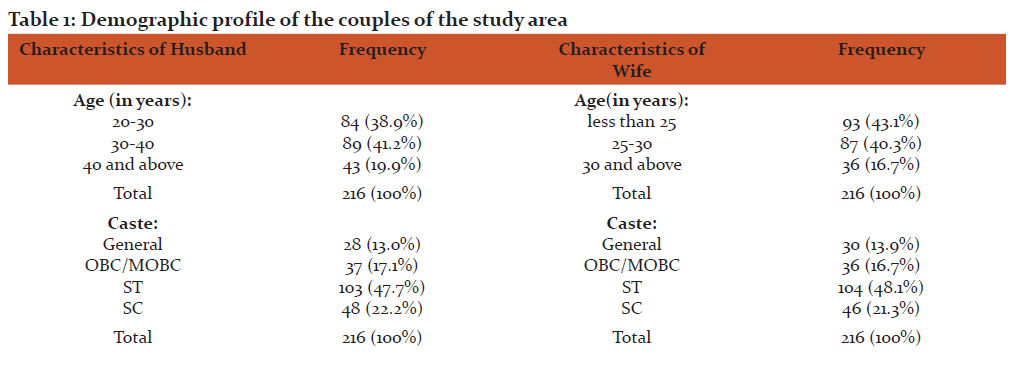
A total of 216 women are enrolled in the study. Information about different socio- economic characteristics of the enrolled women and their household, information on their birth history, awareness on different facilities on maternal and child healthcare schemes are also collected. The details demographic information of the couples is shown in table1.
Table 1: Demographic profile of the couples of the study area:
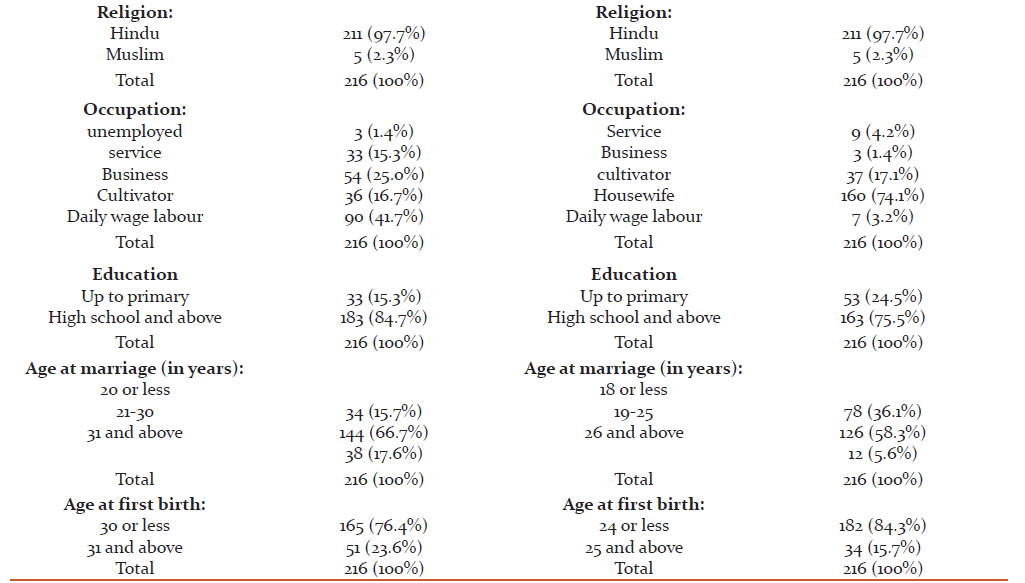
In the present study, good awareness level is observed about the scheme Mamoni as compared to the other schemes. About 31.9% of the respondents spontaneously answered about the facility "an amount of Rs 1000 which is given to pregnant women during the Antenatal care". The Government of Assam has introduced Mamoni scheme under which a booklet having tips of safe motherhood are provided to the pregnant women. Awareness about the Mamoni scheme is found to be moderate. About 30% of the study subjects responded spontaneously that they are aware about this booklet; while about 60% responded after probing.
Only 2.8% of the respondents spontaneously answered about the facility free drop back from institute to home. About 11.1% of the respondents spontaneously answered about the facility free treatment during delivery. The details of the results are shown in table 2.
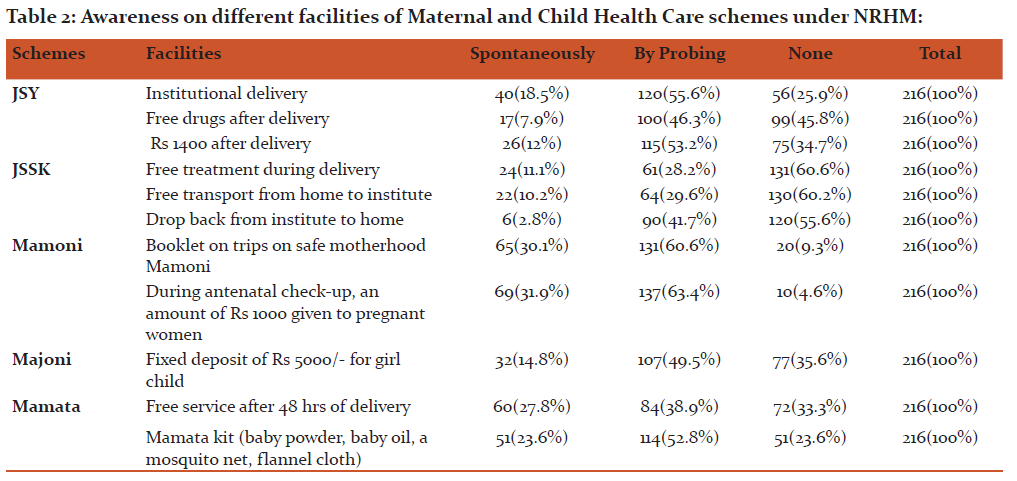
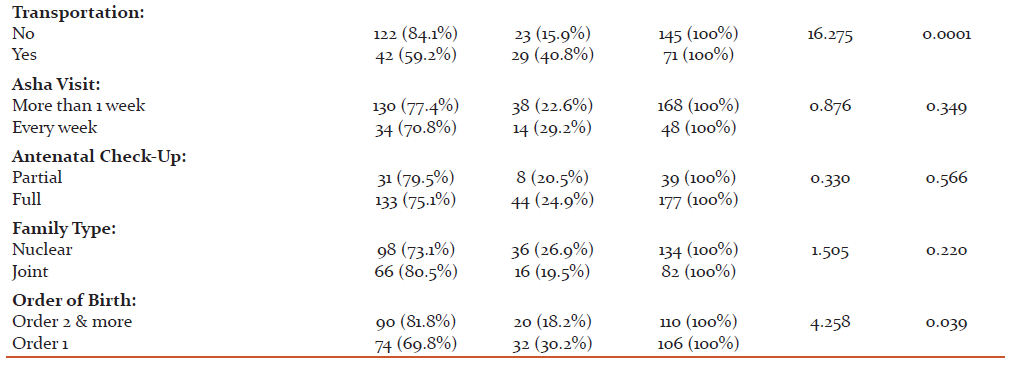
Further, chi- square test for independence of attributes is used to study the association between awareness level and different socio-demographic factors of the respondents regarding various entitlements of JSSK. The study shows that caste of the respondents has significant association with the awareness level. The respondents belong to ST/SC community have less awareness on different facilities provided by the scheme JSSK as compared to the respondents belong to other communities. The study also shows that awareness level is high w.r.t. the education level of the respondents. The respondents who have completed education up-to high school and above are much aware as compared to the respondents who have completed their education up-to primary school level. But, it is not statistically significant. The study shows that distance from Primary Health Center (P.H.C) to the respondent's home have significance association with the awareness level of the respondents. The respondents who have less than 3.5 k.m. distance from P.H.C.to their home are more aware as compared to the respondents who have distance from PHC to their home is 3.5 k.m. and above. It is also seen that good road communication and transportation facility of the study area have significant association with the awareness level of the respondents. The study also shows that the respondents who have completed full antenatal check-up (ANC) are more aware on different facilities provided by the scheme Janani Shishu Suraksha Karyakram (JSSK) as compared to the respondents who have partially completed their antenatal check-up (ANC). But, this association is not statistically significant. The study shows that order of birth have significant association with the awareness level of the respondents.
The association between socio-demographic factors and awareness level of the respondents regarding Janani Shishu Suraksha Karyakram (JSSK) are shown in table 3.
Discussion:
In this study, good awareness level is noticed about the facilities provided by the scheme Mamoni as compared to other schemes. In other parts of India, different studies are conducted to assess the level of awareness regarding various maternal and child health care schemes. Most of the other studies that have explored awareness of maternity benefit schemes mainly concentrated on awareness regarding Janani Suraksha Yojna (JSY). According to study by Kannan et.al awareness level about JSY is about 62.3% [2]. The study by Chavan et. al. it is about 52.7% and only 17.24% of the respondents are able to answer the correct name of the scheme JSY [1]. The study by Chatterjee et.al had reported that none of the respondent able to utter the correct name of the scheme JSY. According to the study by Chatterjee et.al about 18.75% 0f the respondents aware of the facility free normal delivery and none of them are aware of free caesarean section. The study by Barua K. reported that about 88.1% of the respondents aware about the facility free service given to the women after delivery which is good as compared to the findings of the present study. In the present study only 27.8% of the respondents aware about the facility free service after delivery. The study by Baruah K, had reported that about 85% of the respondents aware about the facility free drugs which is given to the women during delivery and according to study by Chatterjee et.al, about 18.75% of the respondents aware about this facility [1]. In the present study only 7.9% of the respondents aware about the facility free drugs which is given to the women during delivery.
According to the study by Chatterjee et.al about 14.58% of the respondents aware about no user charge during delivery and according to the study by Baruah K, about 85% of the respondents aware about no user charge during delivery [1].In the present study only 11.1% of the respondents aware about no user charge. There is a difference between the findings of Barua K and the present study regarding awareness about no user charge during delivery. The findings of the present study shows lower awareness level about the facility no user charge as compared to the findings of the Baruah K. According to the study by Baruah K, awareness on free transport from home to health institution is about 82.7% whereas in the present study only 10.2% of the respondents are found to be aware about the free transportation facility provided to the mother. According to Baruah K. [2] study, about 72.4% of the respondents aware about the facility drop back from institute to home after delivery and according to the study by Chatterjee et.al about 35.42% of the respondent aware about this facility. In the present study only 2.8% of the respondents aware about the facility free drop back from health institution to home.
Overall awareness level among the respondents in the present study regarding various entitlements of maternal and child health care schemes are poor as compared to Chatterjee et.al and Baruah K study.
Conclusion and suggestions:
Efforts are needed to increase awareness level of the reproductive women in the rural areas like Majuli regarding various free entitlements of NRHM to increase the utilization of the benefits of the schemes.
For enhancing the awareness level about the different health care schemes provided by state and central government, awareness programmed has to be organized. The Public-Private-Partnership (PPP) may be encouraged in these areas. ASHA: the village health worker should take initiative steps to bring more awareness among the masses. She can play a very vital role in communicating between the masses and public health system. The different forms of print, electronic and social media may play a very pro-active role for increasing the awareness level about different health facilities provided by the government among the beneficiaries. Finally, it may be conclude that the co-operation from govt. as well as the people in general will certainly lead to the better awareness in these areas. The key for the successful implementation of these schemes, programmed of mass awareness are necessary.
Acknowledgement: The researchers acknowledge SAP DRS for their financial support during data collection.
References:
1. Begum Rasida (2014): "Maternal Health care services in India with special reference to Suraksha Yojna in Assam"- A peer-reviewed indexed International Journal of Humanities and Social Science, ISSN: 2278-5264(Online), volume-III, Issue-II
- Chatterjee S.et al (2015): "Awareness about Janani Shishu Surakha Karyakram (JSSK) among pregnant mothers - a community based study in a rural area of West Bengal, India" IOSR Journal of Dental and Medical Sciences, p- ISSN: 2279-0861. Volume14, Issue 9.
- Parasuram S.et al (1999): "Role of Women's Education in India: Evidence from National Family Health Survey", Himalaya Publishing House, Mumbai.
- Millennium Development Goals India Country Report 2015, social statistics division ministry of statistics and programme implementation government of India.
- International institute for population sciences and macro international, National Family health survey (NFHS-3), 2005-06 India, Mumbai.
- World Health Organization (2005).Immunization coverage cluster survey-Reference manual. Geneva, Switzerland: Department of Immunization, vaccines and Biological, Family and community Health. World Health Organization.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





