IJCRR - 9(15), August, 2017
Pages: 45-48
Print Article
Download XML Download PDF
A Review on Quality of Life in Cancer Patients: An Indian Scenario
Author: Reena Kumari, Jaspreet Kaur, Monika Kajal
Category: Healthcare
Abstract:Cancer is a major public health concern among million of people worldwide and claims thousands of life. The main aim of this review article was to assess the Quality of life (QOL) in Indian cancer patients. QOL is a vital health outcome measure that can only be described in individual terms. It integrates several aspects of life and takes into account impact of illness and treatment. According to the available articles and literature reviews it is found that most of the patients were leading unsatisfactory QOL. Various domains such as physical, psychological, social dimensions etc are affected which in turn influenced the QOL of the patient. Factors such as pain, reduced working capability, and disturbed sleep pattern were significantly found to be affecting the QOL of cancer patients.
Keywords: India, carcinogens, QOL (Quality of life)
DOI: 10.7324/IJCRR.2017.9158
Full Text:
Introduction
Cancer is major cause of morbidity and mortality 1,2 and second most common cause of death after heart attack worldwide 3. It is a group of diseases that occurs due to uncontrolled growth and proliferation of abnormal cells which can even lead to death if not controlled 2, 4. It also leads to physical inadequacies and psychological problems with periods of remission and exacerbations 5. Current dogma states that cancer is a multi-gene, multi-step disease which originates from a single abnormal cell (clonal origin) with an altered DNA sequence also known as mutation 2.
Epidemiology
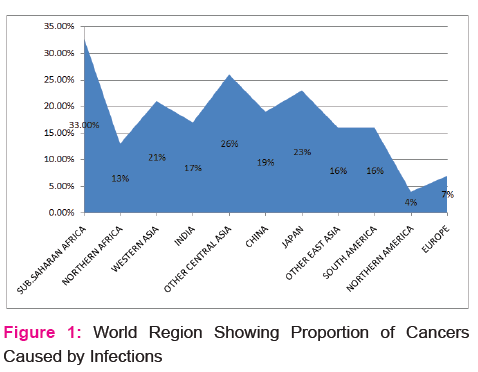
Cancer mortality is higher among men (207.9 per 100,000) than women (145.4 per 100,000). Globally most common cancers in men are cancers of lung, prostate, colorectum, stomach and liver amounting to a total of 4.3 million cancer cases. In women, most common cancers are cancers of breast followed by colorectum, lung, and cervix, and corpus uteri with a total of 3.7 million cases 1. It is highest in African American men and lowest in Asian/ Pacific Islander women 6. Approx 16% of cancer worldwide is caused by infection. Figure 1 shows the world region of cancer caused by infection 7 . The global burden is expected to increase to 21.4 million new cancer cases and 13.2 million cancer deaths by 2030 due to increase in size of population, adoption of western lifestyles such as smoking, poor diet, physical inactivity, and reproductive factor 4.
According to World Health Organization (WHO), 14.1 million cases were diagnosed and 8.2 million cancer-related deaths were estimated in 2012 1, whereas according to the 2016 estimates by National cancer institute new cases are 1,685,210 and 595,690 are cancer-related death in the united states 6 and is expected to increase till 25 million a year in over the next 20 years 3, 8. Cancer is leading cause of death accounting for 27% of all deaths in Americans, Native Hawaiians and Pacific islanders (AANHPTs) and 12% of deaths worldwide which only differ by 4% in Africa to 23% in Northern America. Worldwide cancer deaths are projected to increase by 60% from 2012 to 2030 (SEER cancer statistics review 1975-2013).
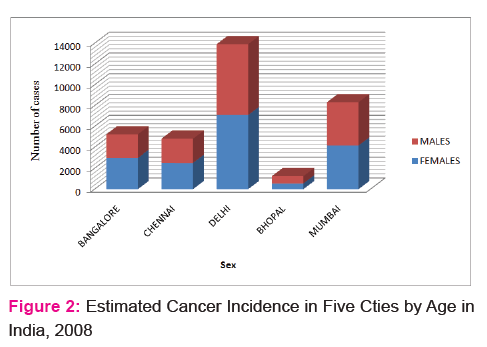
Cancer is a major public health concern in India with 1.01 million new cancer cases per year, indicating India as a single country contributing to 7.8% of the global cancer burden 1,5. Incidence of cancer in India varies from 44-122 per 100,000 populations in males and 52-128 per 100,000 populations in females 5 and according to The International Agency for Research on Cancer GLOBOCAN project, it will nearly double in the next 20 years 2. The number of cancer incidence in five cities of India is shown in FIGURE 2 9.
The most common cancer in Indian men are tobacco related whereas for Indian women, cervical cancer (122,844 diagnosed and 67,477 death) 10 is the second most incident cancer, breast cancer being the first 2.
Types
More than 100 types of cancer are present worlwide and are named according the the organs, tissue(histological types) or sites involved. On the basis of histological types they are grouped into six major categories: carcinoma, sarcoma, leukemia, lymphoma, myeloma and mixed types. Carcinomas result from altered epithelial cells, which cover the surface of our skin and internal organs and accounts for 80-90% of all cases. Sarcomas result from changes in muscle, bone, fat, or connective tissue and resemble the tissue in which they grow. Example: Osteosarcoma, Kaposi sarcoma, malignant fibrous histiocytoma, liposarcoma, dermatofibrosarcoma protuberans etc. Leukemia results from overproduction of malignant white blood cells. It is 4 types, acute or chronic based on how quickly the disease gets worse and lymphoblastic or myeloid based on types of blood cells involved. Lymphoma is a cancer of the lymphatic system cells in which abnormal lymphocytes proliferate in lymph nodes and lymph vessels, as well as in other organs of the body. They may also occur in brain, stomach and breast. Myelomas also known as plasma cell myeloma and kahler disease are cancers of specialized white blood cells that make antibodies. The abnormal Plasma cells build up in the bone marrow and form tumors in all bones of the body. When two or more components of cancer are involved they come under mixed types. Carcinosarcoma, teratocarcinoma etc are categorized into Mixed types11,12,13,14.
Aetiology
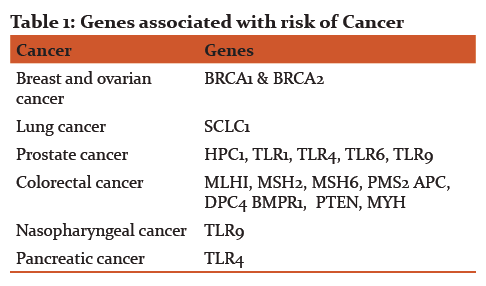
There are multiple causes of cancers which involves both environmental and Genetic/Hereditary factors 12. Cancer is a genetic disease that is caused by mutation in genes and can be inherited from our parents. The genetic changes that causes cancer tend to affect, proto-oncogenes, tumor suppressor genes, and DNA repair genes .These changes are sometimes called “drivers” of cancer 8. Different types of genes associated with risk of most important and common cancer are shown in Table 1 3.
Environmental factor include X-rays(radon), UV light, viruses (human papillomavirus, hepatitis B, Epstein-Barr virus, human T-cell leukemia virus and herpes virus) 8,12 , tobacco products, pollutants, chemicals (benzene, arsenic and organic solvents) 12, alcohol consumption 15. Cancer deaths in the U.S., including cancers of the lung, esophagus, bladder and pancreas are caused by tobacco smoking which contributes to half of cancer deaths in U.S. UV light is associated with most skin cancers, including the deadliest form, melanoma. These factors probably act directly or indirectly on the genes that are already known to be involved in cancer 12. Many causes of cancer are still unknown16.
Risk factors
Tobacco use, Alcohol use, Dietary factors, including insufficient fruit and vegetable intake, Age (older people are at greater risk), Overweight and obesity, Physical inactivity, Chronic infections from helicobacter pylori, hepatitis B virus (HBV), hepatitis C virus (HCV) and some types of human papilloma virus (HPV), exposure to chemicals 5,19,21 are considered among the main risk factors of cancer.
Discussion
According to WHO, Quality of life (QOL) is defined as ‘individuals’ perception of life, values, objectives, standards, and interests in the framework of culture 1,19 of the social environment in which they live and in relation to their goals, expectations, standards and concerns 5. It is a multidimensional construct that includes several aspects of life such as physical health status, psychological wellbeing including people’s emotion, social and cognitive functioning and take into account impact of disease and treatment based on patient’s life experiences6, 11, 12. When the hopes of an individual are fulfilled by experience in accordance to their goals, expectations, standards and concerns, he is said to be having a good quality of ife19 and it is usually expressed in terms of satisfaction, contentment, happiness and fulfilment and the ability to cope impact of illness and treatment20. Quality of life should be taken into account so that it can help in selecting more suitable treatment alternatives5.
Various studies there are several therapeutic modalities for cancer treatment such as surgery (curative, palliative) chemotherapy, and radiation therapy, which may be used alone or in combination and may have impact on the quality of life of those being treated 1,6,8,10,12,21,26.has been done to assess the QOL of patient in India and worldwide and
Kannan et al (2011) conducted a study on “Assessment of quality of life of cancer patients in a tertiary care hospital of South India” in which the aim of the study was to assess the QOL of cancer patients by using a validated questionnaire. Eleven types of cancer were identified. Study concluded that among the total samples, 80% of them has average and below average QOL, suggesting that an increasing importance should be given to the incorporation of Quality of Life as an outcome, in addition to other clinical endpoints12.
Sunderam et al (2016) conducted a study
to assess the quality of life among cancer patients in relation to type of treatment (chemotherapy vs. radiotherapy) and to determine the quality of life in relation to number of chemotherapy cycle.113 cancer patients (64 undergoing chemotherapy and 49 undergoing radiotherapy) were selected and interviewed by a validated questionnaire. Study concluded that cancer patients undergoing treatment had poor quality of life and among them patients undergoing chemotherapy had lower quality of life compared to patients undergoing radiotherapy 1. Treatment modalities due to their long term side effects has impacts on QOL in patients 10,22.
Dehkordi et al (2009) 23 conducted a study on “Quality of Life in Cancer Patients undergoing Chemotherapy” in which the aim of the study was to assess the quality of life in cancer patients with solid tumours and at different chemotherapy (CT) cycle. He concluded that cancer patients should be encouraged to complete a CT course as it plays an important role in the treatment outcome and the QoL in cancer patients undergoing CT. The result was similar to the study done by the same author in 201119. In a study done by Elsaie et al (2012) most function dimensions of QOL for colorectal cancer patient significantly decreased post the first chemotherapeutic session and all symptom dimensions except fatigue and overall symptoms have been increased post the first chemotherapeutic session21. There is a strong correlation between QOL and number of treatment cycles and the various cancer related factors can affect the QOL 19.
The most frequently seen cancer among women are breast cancers and are ranked third among all cancer deaths. A study was done by Akca et al (2014) to evaluate the changes in quality of life of the female patients who had undergone surgical treatment for breast cancer. Female patients with breast-preserving surgery (BPS), modified radical mastectomy (MRM), simple mastectomy (SM) aged between 28-55 years were included in the study. Validated Turkish versions of EORTC QLQ-C30, and EORTC–BR23 questionnaires were used for all patients. The study concluded that MRM group was found to be more adversely affected than the BPS group 5. In a similar study performed by Dubashi et al (2010), overall QOL in younger patients with breast cancer appeared to be overall good. The QOL and sexual function were marginally worse in the breast conservation group when compared to mastectomy group24.
Cervical cancer is the most common cancer and Hemavathy et al (2016) conducted a study to explore the quality of life among women with cervical cancer in which 280 samples were included. According to her, QOL among cervical cancer patients is very important aspects in developing country like India and there is a need to assess the QOL and implement the relevant measures to cervical cancer survivors 10.leading cause of death for Indian women which affects the QOL of women.
Jyothi D. Souza et al 2013 conducted a study to assess the QOL and performance status of Head and Neck Cancer patients to find relation between domains of QOL and to find association between QOL and demographic and disease variables in which Karnofsky Performance Status (KPS) scale was used to assess performance status. Subjects with all stages of HNC and primarily diagnosed with HNC and undergoing disease specific treatment. Study concluded that physical, psychological, social, spiritual, functional domains are affected in patients with HNC. The impact on one domain area of well being, significantly affects the other domain of QOL and there is relationship between the performance status and QOL 25.
According to our knowledge scarce studies are available on the quality of life in different types of cancer in India. Most of the studies are done on breast cancer. Cancer can lead to different types of changes in the life of cancer patient which can be the general well being or physical, psychological and social status of the patient. Various studies shows that there is no correlation between the QOL and age, sex, marital status, educational status, duration of disease, economic condition, and occupational functions of the cancer patient 1, 19. Problem in the case of long term survivors in the areas of support i.e social or emotional, spiritual and philosophical views of life and health status was also prominently seen. The gap between expectation and reality should be reduced, and the patient should be satisfied with what he\ she have to improve their QOL20.
Conclusion
The present review concluded that cancer is an important health issue which influences QOL in cancer patient. It is necessary to narrow the gap between hopes, aspiration, dreams and reality to improve their QOL. Further studies need to be done as there is need to understand the causes and impact of cancer related factors on QOL and also the impact of cancer treatment and implement strategies accordingly.
Acknowledgements
I would like to acknowledge my co-authors for their immense support and guidance and helping me find my literature for this review article. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: none
Conflict of interest: There is no conflict of interest
References:
- Sunderam S, Jeseena KJ, Kashyap V, Singh SB, Kumar M. Study on Quality Of Life of Cancer Patients In Relation To Treatment Modality in a Tertiary Health Institute of Jharkhand. IOSR Journal of Dental and Medical Sciences 2016; 15(5):16-20
- Mallath M.K, Taylor DG, Badwe RA, Rath GA, ShantaV , C S Pramesh CS et al. The growing burden of cancer in India: epidemiology and social context. SERIES 2014; 1-8
- Anand P, Kunnumakara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS, Sung B, and Aggarwal BB. Cancer is a Preventable Disease that Requires Major Lifestyle Changes. Pharmaceutical Research 2008; 25(9): 2097-2116
- American Cancer Society. Global Cancer Facts and Figures 2nd Edition.2011
- Akca M, Ata A, Nay?r E, Erdo?du S, Ar?can A. Impact of Surgery Type on Quality of Life in Breast Cancer Patients. J Breast Health. 2014; 10: 222-8.
- Manandhar S, Shrestha DS, Taechaboonsermsk P, Siri S, Suparp J. Quality of Life among Breast Cancer Patients Undergoing Treatment in National Cancer Centres in Nepal. Asian Pac J Cancer Prev 2014;15(22): 9753-9757
- American cancer society. Global facts and figures. 3rd edition. 2015
- Bukhtoyarov OV, Samarin DM. Pathogenesis of Cancer: Cancer Reparative Trap. Journal of Cancer Therapy 2015; 6: 399-412.
- Marimuthu P. projection of cancer incidence in five cities and cancer mortality in India. Indian journal of cancer 2008; 45(1): 4-7
- Hemavathy V, Julius A. A study to assess the quality of life among women with cervical cancer in selected hospitals at Chennai. Int J Pharm Bio Sci 2016; 7(4): 722–724
- Subathra V. A Study on Quality of Life of Patients Receiving Palliative Care Services. Paripex- Indian journal of research 2012; 1(10): 26-27
- Kannan G, Rani V, Ananthanarayanan RM1 Palani T, I Nigam N, Janardhan V, Reddy UM . Assessment of quality of life of cancer patients in a tertiary care hospital of South. India. Journal of Cancer Research and Therapeutics 2011; 7(3):275-279
- SEER Training modules, U.S. National institutes of health, national cancer institute. 6, May.2017
- Mandal A. Cancer classification. Medical news. 2012
- Connor J. Alcohol consumption as a cause of cancer. Society for the Study of Addiction. 2016; 112: 222–228
- Clapp R, Howe G, Lefevre MJ. Environmental and Occupational Causes of cancer. Lowell Center for Sustainable Production. 2005: 1-50.
- Chemicals, Cancer, and You. American Cancer Society Fact Sheet “Occupation and Cancer”; International Agency for Research on Cancer. 2009
- World Health Organization. NMH Fact sheet January 2010
- Haydarnejad MS, Hassanpur Dehkordi A, Solati Dehkordi K. Factors affecting quality of life in cancer patients undergoing chemotherapy. African Health Sciences 2011;11(2):266-270
- Calman KC. Quality of life in cancer patients – an hypothesis. Journal of medical ethics. 1984; 10: 124-127
- Elsaie OA, Elazazy HM, Abdelhaie SA. The Effect of Chemotherapy on Quality Of Life of Colorectal Cancer Patients before and 21 Days after the First Chemotherapeutic Sessions. Life Science Journal 2012; 9(4): 3504-3514.
- Nemati M, Alhani F, Zandshahdi R. Quality of life in cancerous adolescences undergoing chemotherapy. 1st congress in quality of life. Tehran, Iran: Book of Abstracts 2003;25
- Dehkordi A, Heydarnejad MS, Fatehi D. Quality of Life in Cancer Patients undergoing Chemotherapy. Oman Medical Journal. 2009; 24(3)
- Dubashi B, Vidhubala E, Cyriac S, Sagar TG. Quality of life among younger women with breast cancer: study from a tertiary cancer institute in south India. Indian J Cancer 2010; 47: 142-147.
- Prima Jenevive Jyothi D.Souza, Chakrabarty J, Sulochana B, Gonsalves J. Quality of Life of Head and Neck Cancer Patients Receiving Cancer Specific Treatments. Journal of Krishna Institute of Medical Sciences University. 2013; 2(1): 51-57.
- Damodar G, Gopinath.S, Kumar SV, Rao AV. Reasons for Low Quality of Life in South Indian Cancer Patient Population: A Prospective Observational. Indian Journal of Pharmaceutical Sciences. 2014; 76(1): 2-9.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





