IJCRR - 3(1), January, 2011
Pages: 18-27
Print Article
Download XML Download PDF
EFFECT OF SUPERVISED EXERCISE PROGRAM AND HOME BASED EXERCISE PROGRAM IN
OSTEOARTHRITIS OF KNEE JOINT
Author: Vandana J. Rathod Jagatheesan Alagesan, Parthipan Ramasamy
Category: Healthcare
Abstract:Introduction: Osteoarthritis of knee is a most common degenerative joint disease. Exercise programmes have been shown to be effective when patients are closely supervised by physiotherapists; however, data are lacking on the efficacy of an unsupervised home based exercise regimen in subjects with osteoarthritis of knee. Materials and Method: An experimental study was carried out to compare supervised exercise program and home based exercise program in osteoarthritis of knee joint. A convenient sample of 60 subjects with unilateral osteoarthritis of knee joint, age between 45 and 55 years of both sexes were divided in to supervised exercise group (Group-A) and home based exercise group (Group-B). Group-A was receiving exercises under the supervision of physiotherapist at outpatient department of Physiotherapy College and Group-B was doing exercises at home following a specially designed exercise pamphlet. Numeric Pain Rating Scale and Western Ontario and McMaster universities Index were used as outcome measure before and after two months of intervention. Results: There was a significant decrease in pain and also significant improvement in physical function (p< 0.001) in subjects with knee osteoarthritis who received supervised exercises and home based exercises. Both are effective in treatment of osteoarthritis of knee joint. Conclusion: The results of this study indicate that both supervised exercise programme and home based exercises are effective in alleviation of pain and improving physical function in osteoarthritis of knee joint.
Keywords: Knee osteoarthritis, supervised exercises, home based exercises, exercise pamphlet
Full Text:
INTRODUCTION
Osteoarthritis is a chronic joint disorder in which there is a progressive softening and disintegration of articular cartilage accompanied by new growth of cartilage and bone at the joint margins and capsular fibrosis.1 Disease resulting from uncoupling of the balance between the cartilage degeneration and regeneration. Osteoarthritis contributes greatly to disability in the general population, particularly in the elderly.2,3 World Health Organization estimated that it accounts for 14.8 million disability adjusted life years (DALYs) lost, with 80% percent of those afflicted having some degree of limitation of movement and 25% being unable to perform the major activities of daily living. As the incidence and prevalence of osteoarthritis increase with age, the DALYs lost due to this disease are expected to increase by 40% by 2030.4,5,6 Generally the process of clinically detectable osteoarthritis is irreversible and typical treatment consists of medication and other interventions includes physiotherapy in majority.7,8 Management of osteoarthritis is directed towards decreasing the symptoms. Physiotherapeutic treatment, particularly exercise, has been part of the management of knee osteoarthritis for nearly a century and is the second most frequently prescribed treatment after oral medication.9,10 There are many barriers to the uptake of exercises in population and two are of particular importance: (1) Failure in the part of medical practitioners to properly recommend exercises to patients and make appropriate referrals to exercise professionals and (2) failure of patients to comply with prescribed exercises programs. Exercises are underused by medical practitioners as a treatment strategy for osteoarthritis.11 Given the large number of patients who choose to exercise independently where many failed to consult a professional regarding the most appropriate exercise. Thus, it is important to understand prescribing exercises to patients and potential benefits such exercises. Recent researchs12,13,14,15,16 has provided a rationale for the use of muscle rehabilitation as part of overall treatment regimen for knee osteoarthritis. Regular knee strengthening and aerobic exercises shows improvement in functional ability, aerobic capacity and endurance and reduce knee pain. However, the most effective types and combinations of exercise and dosage are unclear. Various studies have examined the effect of different home based exercises in knee osteoarthritis.17,18,19,20 Exercises reduce pain and improve physical function in patient with osteoarthritis knee.17,21 The need for cost effectiveness throughout the health care system emphasizes the importance of knowing whether patients require numerous visits to a physical therapist or whether they might receive a similar benefit from a well-designed home program. The purpose of this study is to determine the effectiveness of a treatment that included exercise under supervision compared with an exercise program performed at home for osteoarthritis of the knee. Home based exercises training require participants to perform different exercises in home in guidance with exercises booklet. The effects of unsupervised exercises are still controversy and need to be proved.
MATERIALS AND METHODS
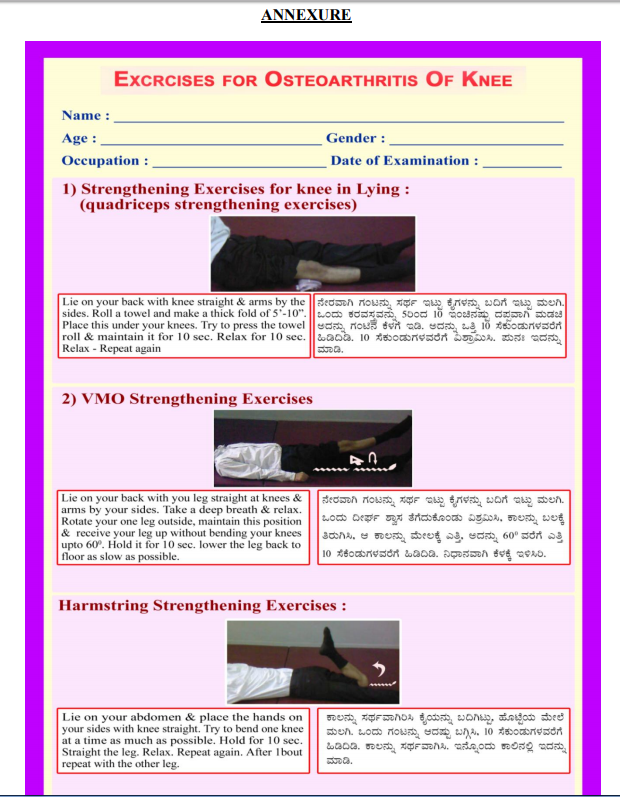
An experimental study was carried out to compare supervised exercise program and home based exercise program in osteoarthritis of knee joint at outpatient department of a physiotherapy college. Ethical clearance was obtained from institutional review board. A convenient sample of 60 subjects with unilateral osteoarthritis of knee joint, age ranging between 45 and 55 years of both sexes were included in the study after obtaining informed consent. Subjects with lower extremity joint replacement, post fracture stiffness, ligament injury of knee joint and secondary osteoarthritis were excluded. Subjects were consecutively assigned in to Group-A or Group-B i.e. first one to Group-A and second to Group-B and so on. The subjects of both groups were explained about the importance of exercise. Subjects of Group-A were put under supervision of therapist during exercises in physiotherapy outpatient department and also taught five joint protection techniques. Subjects of Group-B were advised to do the same exercises at home with the help of exercise pamphlet (Exercise Pamphlet is printed in two pages of standard A4 size paper in both Vernacular [Kannada] and English with diagrams prepared for this study vide Annexure). Exercises consist of Quadriceps strengthening exercise in lying and sitting, Hamstring and VMO Strengthening exercises and proprioceptive training exercises with five joint protection techniques as follows,
1. Quadriceps strengthening exercise in lying- Lie on your back with leg straight at knees and arms at sides. With a thick fold of 5-10? cotton towel roll, subject was advised to place under knee and to press it till 10 seconds. Relax. Repeat.
2. VMO strengthening exercise- Lie on your back with leg straight at knees and arms at sides. Rotate your one leg outside, maintain this position and receive your leg up without bending your knee up to 600 . Hold it for 10 seconds. Lower the leg as slowly as possible. Relax. Repeat.
3. Hamstring strengthening exerciseLie on your abdomen and place hands on your sides with knee straight. Try to bend your knee at a time as much as possible. Hold for 10 seconds. Straight the leg. Relax. Repeat.
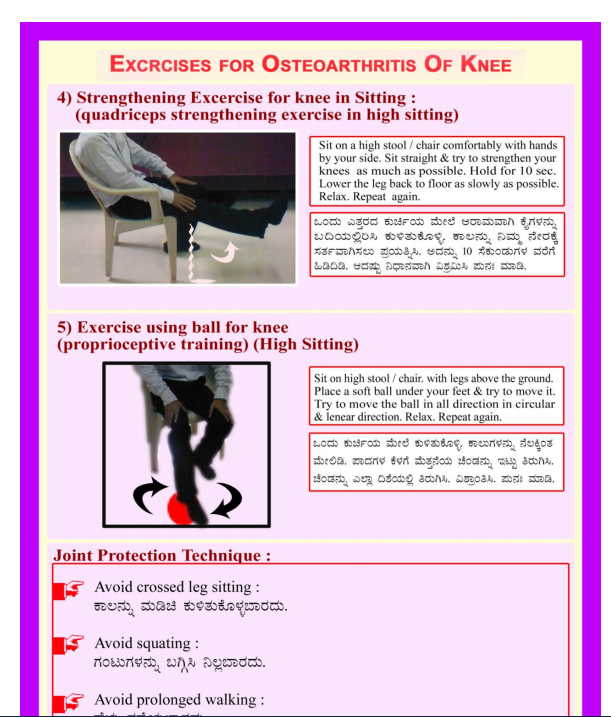
4. Quadriceps strengthening exercise in sitting- Sit on chair or high stool. Sit straight and try to straighten your knee as high as possible. Hold for 10 seconds. Lower the leg to floor as slowly as possible. Relax. Repeat.
5. Proprioceptive training exercise- Sit on chair or high stool with leg above the ground. Place a soft ball under your feet and try to move the ball in all direction in circular and linear direction. Do it for 10 seconds. Relax. Repeat.
Joint protection techniques
1. Avoid crossed leg sitting.
2. Avoid squatting.
3. Avoid prolonged standing.
4. Avoid prolonged walking.
5. Avoid stair climbing.
Subjects of both the groups were advised to do each exercise 10 times with 10 seconds hold and 10 seconds relaxation, once a day for six days in a week for two months. The outcome measures used were Numeric Pain Rating Scale (NPRS) and Western Ontario and McMaster universities (WOMAC) Index; all subjects of both groups were assessed before and after two months of intervention.
RESULTS
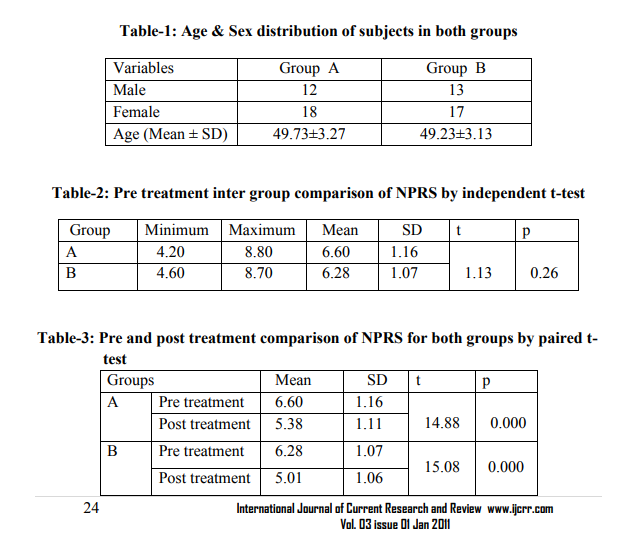
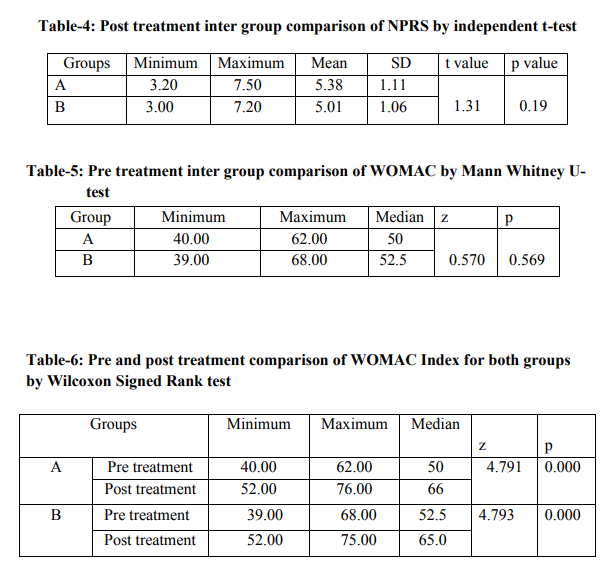
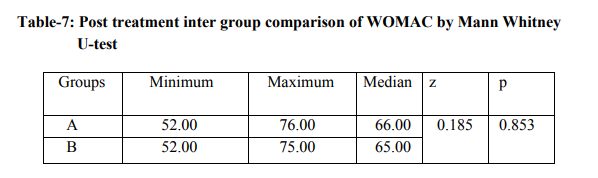
The data collected were analyzed for demographic variables and significance by using SPSS-17 for windows. Significance was tested by independent t-test and paired t-test for NPRS and Mann Whitney U-test and Wilcoxon Signed Rank test for WOMAC index with p < 0.05. Table-1 shows age and sex distribution of both groups, the Mean SD for age in Group-A is 49.73 3.27 and group-B is 49.23 3.13. Inter group comparison at baseline was done by independent t-test for NPRS shown in table-2. The Mean SD for Group-A is 6.60 1.16 and Group-B is 6.28 1.07 with p=0.26 proves homogeneity of both groups before intervention. Intra group comparison was done by using Paired t-test shown in table-3, the Mean SD of post treatment for Group-A is 5.38 1.11 and Group-B is 5.01 1.06 with p value < 0.001 for both groups confirms that there is significant reduction of pain in both groups after intervention. Table-4 shows post treatment comparison between groups by independent t-test with t=1.31 and p=0.19 proves no significant difference between groups after intervention. WOMAC Index scores at baseline were compared by Mann Whitney U test for homogeneity shown in table-5. The median for Group-A is 50 and group-B is 52.5 before intervention in WOMAC Index with p=0.569 and z=0.570 proves the same. Intra group comparison was done by Wilcoxon Signed Rank test for both groups shown in table-6 with p value is <0.001 indicating a statistically significant improvement in physical function in subjects with osteoarthritis of knee after intervention. Table-7 shows post treatment comparison between groups by Mann Whitney Utest with z= 0.185 and p=0.853 proves no significant difference between groups after intervention.
DISCUSSION
Osteoarthritis is a degenerative progressive disorder. To answer the question of optimal type, frequency, and also dose of exercises, head to head comparisons in which participants are randomly assigned to receive different exercises are highly needed. There was numerous theories proposed effectiveness of various exercises in treatment osteoarthritis of knee.9,10 Physical therapy interventions might be useful for the people with osteoarthritis of knee, but for some of interventions the effect is unclear. Exercises are considered as the mainstay in the treatment of osteoarthritis of knee. Many treatment modes have been developed in the form of exercises, orthosis, mobilization and modalities.19,22,23 Some studies proved the effectiveness of unsupervised exercises showing small but significant reduction in knee pain.9,14 In this study supervised exercises and home based exercises were given with joint protection techniques. The result of this led to inference that both supervised exercises and home based exercises are effective in reducing pain and improving physical function in subjects with osteoarthritis of knee, when given with proper dosage. Numerous studies have come up with effective home based exercises in treatment of osteoarthritis of knee.17,18,19,20 Although the dosage of exercises with proper guidance provided additional benefits to the subjects in the present investigation. It would be useful to determine the long term effectiveness of such interventions in future studies. The result of this study may be applied to a population with secondary osteoarthritis of knee. This study did not include long-term follow up period, though exercises are effective with long term benefits.12,23 Other limitations of this study are convenient sampling and inclusion of both dominant and non dominant side.
CONCLUSION
This study concludes that home based exercises with proper guidance, exercise pamphlet and dosage are as effective as supervised exercise program in Physiotherapy outpatient department in reducing pain and improving physical function in treatment of unilateral osteoarthritis of knee joint.
References:
1. Apley's system of orthopaedics and fractures, 7th edition, Butterworth - Heineman, Page 80-81.
2. Felson DT, Naimark A, Anderson JJ, Kazis L, Castelli W, Meenan RF. The prevalence of knee osteoarthritis in the elderly: the Framingham osteoarthritis study. Arthritis Rheum 1987; 30:914-918.
3. Badley EM, Tennant A. Disablement associated with rheumatic disorders in a British population: problems with activities of daily living and level of support. Br J Rheumatol 1993; 32: 601-608.
4. Clinical practice guidelines. Osteoarthritis of knee, MOH clinical practice guidelines. Singapore Society of Rheumatology, College of Family Physicians, Singapore, Ministry of Health, Singapore, Chapter of Rheumatologists, College of Physicians, Singapore. 4/May,2007
5. American College of Rheumatology. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines: recommendations for the medical management of osteoarthritis of the hip and knee. Arthritis Rheum. 2000; 43:1905-1915
. 6. Thumboo J, Chew LH, Lewin-Koh SC. Socioeconomic and psychosocial factors influence pain and physical function in Asian patients with knee or hip osteoarthritis. Ann Rheum Dis 2002, 61:1017-20.
7. Felson D T, Lawrence R C, Hochberg M C, et al. Osteoarthritis: New insights. Part 2: Treatment approaches. Annals of Internal Medicine 2000;133:726-737.
8. Jordan K M, Arden N K, Doherty M, et al. EULAR Recommendations: an evidence based approach to the management of knee osteoarthritis: Report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Annals of the Rheumatic Diseases 2003;62:1145- 1155.
9. C. J. McCarthy, P. M. Mills1, R. Pullen, C. Roberts, A. Silman and. A. Oldham Supplementing a home exercise programme with a classbased exercise programme is more effective than home exercise alone in the treatment of knee osteoarthritis. Rheumatology 2004; 43:880-886.
10. Tallon D, Chard JA, Dieppe PA. Exploring the priorities of patients with osteoarthritis of the knee. Arthritis Care Res 2000;13:312-19.
11. DeHaan MN, Guzman J, Bayley MT, et al.Knee osteoarthritis clinical practice guidelines-how are we doing? J Rheumatol 2007;34(10):2099-105.
12. Roddy E, Zhang W and Doherty M. Aerobic walking or Strengthening Exercise for Osteoarthritis of the Knee? A Systematic Review. Annals of Rheumatic Disease 2005;64:544- 548.
13. Fransen M, McConnell S and Bell M. Exercise for osteoarthritis of the hip or knee. The Cochrane Database of Systematic Reviews 2005;4.
14. Thomas et al., Home based exercises programme for knee pain and knee osteoarthritis; Randomized controlled trial.BMJ oct.5,2002 ;325: 752-5.
15. Evick, D. Sonel B., Effectiveness of a home based exercises therapy and walking programme on osteoarthritis of knee.Rhematol.Int.2002, July:22(3) ; 103-06.
16. La Mantia K, Marks R. The efficacy of aerobic exercises for treating osteoarthritis of the knee. New Zealand Journal of Physiotherapy. 1995;23:23-30.
17. Christensen R, Astrup A and Bliddal H. Weight loss: the treatment of choice for knee osteoarthritis? A randomized trial. Osteoarthritis Cartilage 2005;13:20- 27.
18. Adedoyin R, Olaogun M O B and Fagbeja O O. Effect of Interferential Current Stimulation in Management of Osteo-arthritis Knee Pain. Physiotherapy 2002;88:493-499.
19. Deyle G D, Henderson N E, Matekel R L, et al. Effectiveness on manual physical therapy and exercise in osteoarthritis of the knee - A randomized controlled trial.Annals of Internal Medicine 2000;132:173-181
20. Maillefert J F, Hudry C, Baron G, et al. Laterally elevated wedge insole in the treatment of medial knee osteoarthritis: a prospective randomised controlled trial. Osteoarthritis and Cartilage 2001;9:738- 745.
21. P Ravaud, B Giraudeau, I Logeart, J Larguier, D Rolland, R Treves, L Euller-Ziegler, B Bannwarth, and M Dougados. Management of osteoarthritis (OA) with an unsupervised home based exercise programme and/or patient administered assessment tools. A cluster randomised controlled trial with a 2x2 factorial design. Ann Rheum Dis. 2004 June; 63(6): 703- 708.
22. Lin S Y, Davey R C and Cochrane T. Community rehabilitation for older adults with osteoarthritis of the lower limb: a controlled clinical trial. Clinical Rehabilitation 2004;18:92-101.
23. Brosseau L, Judd MG, Marchand S, et al. Thermotherapy for treatment of osteoarthritis. The Cochrane Database of Systematic Reviews 2005; 2.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





