IJCRR - 3(3), March, 2011
Pages: 12-21
Print Article
Download XML Download PDF
IMMEDIATE EFFECTS OF PROPHYLACTIC KNEE TAPING AND BRACING ON PROPRIOCEPTION AND
DYNAMIC BALANCE IN ASYMPTOMATIC AMATEUR ATHLETES- A RANDOMIZED CROSS-OVER TRIAL
Author: Sandhya Sharma, Zulfeequer C.P, S. Raja sekar
Category: Healthcare
Abstract:Purpose of the study: To compare the immediate effects of prophylactic taping and bracing on proprioception and dynamic balance on asymptomatic knee in amateur athletes.
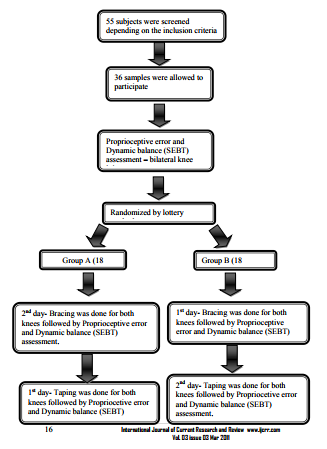
Methods: 36 subjects of both sexes (mean age group was 22.3 + 1.8) were included in the study. Inclusion criteria were minimum proprioceptive degree error: 30 using universal
goniometer, full and free range of motion of lower extremity. They were randomized into two
groups, group A and group B using block randomization, with 18 subjects in each group. Their
proprioception (universal goniometer) and dynamic balance (SEBT) were assessed in both the
knees, and the values were noted by the observer. The subjects underwent, either taping or
bracing in both the knees and their proprioception and dynamic balance were assessed again.
Followed by 24hrs of rest, cross-over of subjects to other technique were performed.
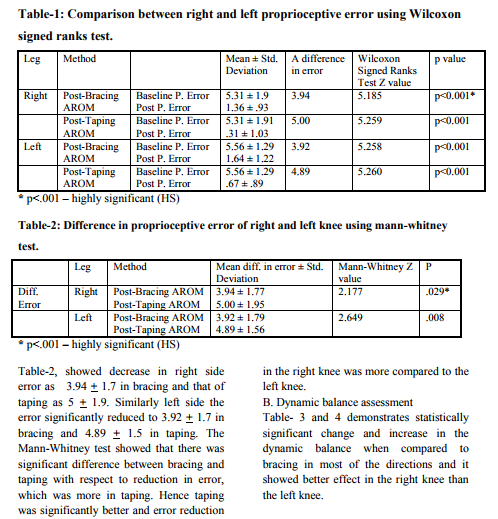
Results: The result showed that there is significant improvement in both proprioception and dynamic balance with taping and bracing. Application of tape and brace on right knee showed a
significant reduction in proprioceptive error. The amount of decrease in error was 3.940 + 1.70
and 50 + 1.90 with bracing and taping respectively. The same when analyzed for left side the
error significantly reduced to 3.920 + 1.70 with bracing and 4.890 + 1.50 with taping. Tape and
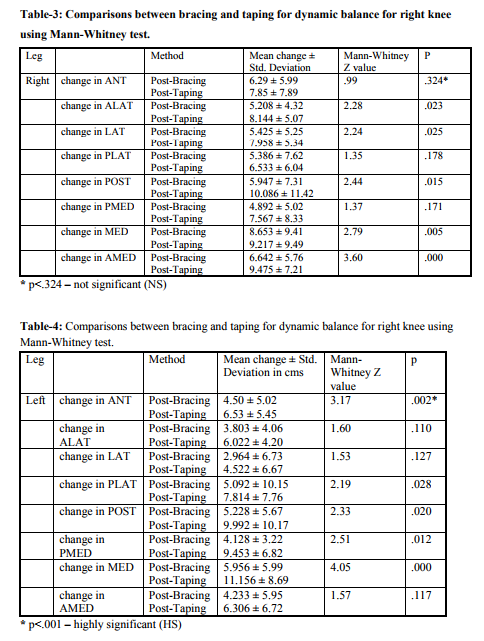
brace have shown equal effect on proprioception. With taping and bracing there is statistically
significant increase in dynamic balance (p< 0.001) in all the direction of SEBT for bilateral
knee.
Conclusion: Bracing and taping were effective in improving the proprioception and dynamic
balance of the amateur athletes.
Keywords: Taping, Bracing, Dynamic Balance, Proprioception, SEBT.
Full Text:
INTRODUCTION
Knee is the most vulnerable site for injuries sustained by the athletes, who engage in sports that demands frequent change in the direction of the body movement and rapid acceleration and deceleration. Moreover knee injuries can significantly affect performance and result in the lost practice and game time and they can lead to the development of chronic knee instability and pain.1 Because of the high prevalence of these injuries, many organized sports association have implemented prophylactic measures in an attempt to decrease the incidence and prevalence of injuries,
however controversy continues to exist in regard to the best method of treatment and prevention of these injuries.2,3 Proprioception and balance are two of the essential components that play an important role in avoiding the injury rates.4 Proprioception has been indicated to coordinate the following movement variables: positioning, force, and velocity. Because of its importance for coordinating sophisticated movements, proprioception is even more crucial for the skill-demanding movements (e.g., tennis playing) than daily movements.5,6 The effect of proprioception on the sports and its difference between patients and healthy adults has been widely tested. However, current knowledge provides insufficient insight into the effect of experience within an amateur athletic population.4 Measures of proprioception characteristically have high variability between different measurement techniques and also between subjects within the same measurement technique, one making objective comparisons of baseline joint position sense (JPS) scores difficult between subjects.7 Dynamic balance is required for normal daily activities, such as walking, running and stair climbing. Sports activities also require proper balance control. The visual, somatosensory, and vestibular systems all contribute to the maintenance of balance and may be adversely affected by musculoskeletal injury, head trauma, disease, or aging. These influences on the visual, somatosensory, and vestibular systems might decrease a person's ability to perform dynamic activities and, thus, impede normal daily functioning. Quantification of balance, or postural control, is often necessary to assess the level of injury or ability to function in order to initiate an appropriate plan of care.8 Squatting exercises are commonly included in lower-extremity rehabilitation programs in an effort to improve strength, balance, and neuromuscular control. Recently, a more complex squatting task to train and assess lower-extremity balance and neuromuscular control has been reported. The Star Excursion Balance Tests (SEBTs) are a series of unilateral mini squats performed while attempting with the opposite leg to reach as far as possible in a given direction.9 Proprioceptive training, star excursion balance exercise, taping and bracing are commonly employed in sports to prevent injury and re-injury. Athletic taping and bracing can prevent injury or facilitate injured athletes return to competition. In general the tape will limit the abnormal or excessive movement of the sprained joint while also providing support to the muscle that the sprain has compromised. Many clinicians attribute the value of taping to the enhanced proprioceptive feedback that the tape provides the athletes during performance.10 The literature shows taping and bracing has positive effect on proprioception but comparing among these which is better is not been studied. The aim and objective of the study was to compare the immediate effects of prophylactic taping and bracing on proprioception and balance on asymptomatic knee in amateur athletes.
METHOD
Study was approved by ethics committee of K.M.C Mangalore. Study was conducted at Kasturba Medical College, Mangalore. The inclusion criteria were Minimum proprioceptive degree error: 3 0 using universal goniometer (pilot study) and subjects with full and free range of motion of lower extremity. Subjects were excluded if they had any neurological deficits of lower extremity, history of lower extremity injury within 6 months and deformity of lower extremity / spine.
Demographic data of the participants were collected. Subjects were randomized into two groups, group A and group B using block randomization with 18 subjects in each group. Their proprioception (universal goniometer) and dynamic balance (SEBT) was assessed in both the knees, and the values were noted by the observer, the tester was blinded. The subjects underwent, either taping or bracing in both the knees depending on the block randomization and their proprioception and dynamic balance were –assessed again, Followed by 24hrs of rest, cross-over of subjects to other technique were performed. During the 24hrs rest period the subject were advised strictly not to undergo any form of training.
Proprioceptive Error Measurement Procedure
The subjects were asked to sit on a table, with their legs allowed to hang freely over the side of the table at a distance of 5cms to 10cms proximal to the popliteal fossa. The knee joint was palpated to place the goniometer, as the lateral joint line acts as the fulcrum (fig 1). The subject?s knee was then extended to 450 , passively and held for 10 seconds in order to memorize the position. Same procedure was repeated with the subject blindfolded and the leg was again held for 10 seconds to facilitate memorizing the position by the subject. In the fourth step the subject still being blindfolded was asked to achieve or place his knee range of motion in the same range i.e. 450 , actively. The degree of error was hence noted by the observers, and the proprioceptive error was calculated.
Star Excursion Balance Test Procedure (SEBT) The SEBT was performed with the participants standing in the middle of a grid formed by eight lines extending out at 450 from each other (fig 2). The participant were asked to reach as far as possible along each of the eight lines, make a light touch on the line, and return the reaching leg back to the center, while maintaining a single-leg stance with the other leg in the center of the grid. Participants were instructed to make a light touch on the ground with the most distal part of the reaching leg and return to a double leg stance without allowing contact to affect overall balance. The terminology of the excursion direction is based on the direction of reach in relation to the leg stance. When reaching in the lateral and postero-lateral directions participants reached from behind the stance leg to complete the task.
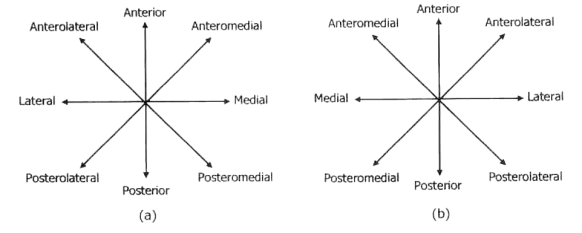
Participants were allowed to practice reaching in each of the eight directions six times to minimize the learning effect. Following a five minute rest period, participants performed three trails in each of the eight directions. They began with the anterior direction and progressed clock wise around the grid. After completion of the three trails of the eight directions and another five minute rest period, the test continued with the stance leg. The investigator recorded each reach distance with the mark on the tape as the distance from the center of the grid to point of maximum excursion by the reach leg. At the conclusion of all trails, the investigator measured the distance of each excursion with a standard tape measure. If the investigator felt the participants used: The reaching leg for a substantial amount of support at any time Removed his/her foot from the center of the grid or Was unable to maintain balance on the support leg throughout the trails The trail would be discarded and repeated.11 Taping Technique Knee Support: Diamond Wrap: Split both ends of the tape, forming four tails. Stretch the tails and apply firmly around the patella superiorly and inferiorly, interlocking the ends (fig 3). Close off with a strip of tape.12
RESULTS
In our study the numbers of samples included were 36, 28 were females and 8 males. The mean age group was 22.3 + 1.8. Taping and bracing has improved the proprioceptive and dynamic balance and comparison between them showed taping to be statistically better than bracing. 1. Comparison between bracing & taping and right knee & left knee A. Proprioceptive error Wilcoxon signed rank test showed statistical significant reduction in error in post bracing and taping in right as well as left knee. (Table 1)
DISCUSSION
Our study aimed at finding the immediate effects of prophylactic knee taping and bracing on proprioception and dynamic balance in asymptomatic amateur athletes. The result showed that there was significant improvement in both proprioception and dynamic balance with taping and bracing. Application of tape and brace on right knee showed a significant reduction in proprioceptive error. The amount of decrease in error was 30 and 50 with bracing and taping respectively. The same when analyzed for left side the error significantly reduced to 30 with bracing and 4 0 with taping. Tape and brace have shown equal effect on proprioception. The minimum error considered for proprioception is 10 using the electronic goniometer.4 In this study we used the universal goniometer, the minimum error established was 30 , which was found from our pilot study. In the present study, taping and bracing showed significant improvement in proprioception. Earlier studies have done on the effects of knee bracing on the joint position sense of subjects with anterior cruciate ligament reconstruction. Results indicated a significant difference for the knee joint angle repositioning test with bracing. In addition, the present study had the same positive findings as McNair et al who reported a significant improvement in the proprioceptive performance of normal subjects who used a knee sleeve.13 As active repositioning relies on afferent feedback from both muscle and joint mechanoreceptors, and that this greater influx of neurological information to the brain and spinal cord tends to increase repositioning ability. The additional information from the muscle mechanoreceptors involved in the active movement and going to the brain requires more processing and increases the precision involved with joint repositioning. It would seem plausible that both Golgi tendon organs (GTO) and muscle spindle activity may be improved as a result of the compression to muscle following application of tape or brace, as muscle spindle is a major receptor of movement. Mechanoreceptors respond specifically to extremes in range of motion and localized compressions. Also, the traction of the tape on the hair and skin provides sensory cues about orientation and position, thus improving joint position sense. 14 The other outcome measure in this study was dynamic balance (SEBT). With taping and bracing there is statistically significant increase in dynamic balance, in all the direction of SEBT for bilateral knee. The increase in dynamic balance following taping and bracing would help athletes to enhance performance and reduce injury. The mechanism by which it is attained is by joint stability. Joint stability requires the interaction of three different subsystems – the passive (the bone, ligaments, fascia and any other non-contractile tissue such as discs and menisci), the active (the muscles acting on the joints) and the neural (central nervous system and nerves controlling, the muscles) subsystems. The most vulnerable area of a joint is known as the neutral zone, where little resistance is offered by the passive structures. Dysfunction of the passive, active or neural systems will affect the neutral zone and hence the stability of the joint. The size of the neutral zone can be increased by injury. Muscle strengthening and application of external support to the joint, decreases the neutral zone.15 When we compared taping and bracing, bracing restricted the anterior lateral, lateral, posterior, medial and anterior medial directions of right knee and anterior, posterior lateral, posterior, posterior medial and medial directions in the left knee . This can be because of braces that restrict the motion, which reduces the opposite-limb reach distances in the braced stance leg. Whether ROM is limited by the brace, causing other segments in the kinetic chain to compensate and achieve necessary motion, is unknown. It is important to examine dynamic balance to gain insight into how braces affect motion in specific directions. Restricted motion in a single direction may affect one?s performance or risk of injury and, therefore, whether a brace should be used for prophylactic purposes in a healthy athlete must be carefully considered. 16 Our results revealed that taping and bracing have significant effect on proprioception and dynamic balance. Tape and brace have certain advantages and disadvantages over each other. So the use of either of them would also depend on these factors. Taping can limit the range of knee, thus offering protection from over stretch or impingement of non-contractile structures. However, the taping technique used by athletes and physiotherapists is often governed by personal preference, the experience of the person applying the tape, and a general "feel" as to the correct technique.17 Braces have advantages over tape in being self applied without needing the expertise of qualified personnel, convenient to apply and remove," reusable, readjust able, and washable. Also, skin problems are less common, especially among those athletes who have an allergic reaction to elastoplasts or zinc oxide. These readymade braces are of various materials, thus providing varying amounts of support and stability. The non rigid braces are often made of canvas or a neoprene-type material, which can easily be slipped on and off, some with additional lacing. A number of studies have established the role of braces in restricting the amount of movement.15 Though, as mentioned above bracing have its advantages over taping. Hence the choice of use among taping and bracing would depend on sports specific needs. We measured the proprioceptive error with the universal goniometer, it was the limitation of our study. Before performing the star excursion balance test, the sports shoe used were also not being assessed. The long term effectiveness of tape and brace were not studied, and there is a need to study the comparison between tapes and brace effectiveness in injured athletes and its sports specific use. Our study population was amateur athletes, studies are warranted to be done in elite groups and post fatigue. Also, studies are required to analyze the various taping techniques.
CONCLUSION
Bracing and taping were effective in improving the proprioception and dynamic balance of the amateur athletes.
References:
1. K, Docherty CL, Dapena J, Schrader J. Prophylactic ankle braces and knee varus-valgus and internal-external rotation torque. J Athl Train 2006;41:239–44.
2. Olmsted LC, Vela LI, Denegar CR, Hertel J. Prophylactic ankle taping and bracing: a numbers-needed-to-treat and cost-benefit analysis. J Athl Train 2004;39:95–100.
3. Mickel TJ, Bottoni CR, Tsuji G, Chang K, Baum L, Tokushige KNS. Prophylactic bracing versus taping for the prevention of ankle sprains in high school athletes: a prospective, randomized trial. JFAS 2006;45:360–5
. 4. Lin CH, Lien YH, Wang SF, Tsauo JY. Hip and knee proprioception of the elite, amateur, and novice tennis players. Am J Phys Med Rehabil 2006;85:216-21.
5. Roberts D, Friden T, Zatterstorm R, Lindstrand A, Moritz U. Proprioception in people with anterior cruciate ligament deficient knee: comparison of symptomatic and asymptomatic patients. J Orthop Sports Phys Ther 1999;29:587-94.
6. Hoffman M, Payne VG. The effects of proprioceptive ankle disk training on healthy subjects. J Orthop Sports Phys Ther 1995;21:90-93. 7. Mizelle C, Brindle TJ, Stanhope S. Proprioceptive error can be reduced with training. Phys Ther Rehabil Sci. 2004;41:260–5.
8. Kinzey SJ, Armstrong CW. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther 1998;27:356-60.
9. Neufeld SD. Reproducing movement in the lower extremity using kinesthetic cues of distance and location. Phys Ther 1981;61:1147-51.
10. Perrin DH. Athletic taping and bracing. Human Kinetics; 2nd ed: 2005. p .4-8.
11. Macdonald R. editor. Taping techniques principles and practice. 2nd ed.Philadelphia (USA): Butterworth Heinemann; 2004. p. 126.
12. Shumbay – cook A, Woollacott MH. Motor control, theory and practical application. Maryland (USA) Williams and wilkins 1995. p. 3-21
13. Earl JE, Hertel J. Lower – extremity muscle activation during the star excursion balance tests. Sport Rehabil 2001;10:93-104
14. Kaminski TW, Gerlach TM. The effect of tape and neoprene ankle supports on ankle joint position sense. Phys Ther Sport 2001; 2:132 – 40.
15. Hardy L, Huxel K, Brucker J, Nesser T. Prophylactic Ankle Braces and Star Excursion BalanceMeasures in Healthy Volunteers. J Athl Train. 2008;43:347– 51.
16. McLean DA. Use of adhesive strapping In Sport. Br J Sports Med 1989 23:147-49.
17. Callaghan MJ. Role of ankle taping and bracing in the athlete. Br J Sports Med 1997;31:102-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





