IJCRR - 3(4), April, 2011
Pages: 29-33
Print Article
Download XML Download PDF
A RARE ANATOMICAL VARIANT OF THE EXTERNAL CAROTID ARTERY
Author: Takkallapalli Anitha, Neelee Jayasree, Krishnamurthy Asha, Dattatray Dombe
Category: Healthcare
Abstract:During routine dissections in the lab, the position of external carotid artery [ECA] and internal carotid
artery [ICA] were found to be mutually displaced. ECA was formed and coursed antero-laterally while ICA formed and coursed postero-medially, in one cadaver on the right side out of 50 cadavers dissected. Though rare, such variations must be given utmost importance before planning for any neck surgeries to avoid post operative complications.
Keywords: External carotid artery, variation, position
Full Text:
INTRODUCTION
Common carotid artery [CCA], internal carotid artery [ICA] and external carotid artery [ECA] provide the major source of blood to the head and neck. Normally right common carotid artery is a branch of brachiocephalic trunk formed at the level of sterno- clavicular joint. The artery courses vertically upwards in the carotid sheath to the level of the upper border of the thyroid cartilage of the larynx which also corresponds to C3, C4 inter vertebral disc. The CCA terminates into external and internal carotid arteries. At their origin in carotid triangle ECA and ICA are normally situated anteromedially and posterolaterally respectively. External carotid artery extends from the level of upper border of the lamina of thyroid cartilage, ascends slightly forwards and inclines posteriorly and laterally, to pass midway between tip of mastoid process and angle of mandible. In the substance of parotid gland, behind the neck of mandible, it divides into its terminal branches, the superficial temporal and maxillary arteries. In the carotid triangle, the ECA gives five branches namely superior thyroid artery, lingual artery, facial artery, occipital artery and ascending pharyngeal artery. ICA ascends vertically upwards without giving any branch to enter into the lower opening of carotid canal at the base of the skull. The variations of CCA bifurcation and position of its terminal branches, ECA and ICA have been described by few anatomists though it is of utmost importance to know this rare position of ECA, to avoid unnecessary complications during carotid end-arterectomy.
METHODOLOGY
The present study was conducted in the department of anatomy at Chalmeda Anandrao Institute of Medical Sciences. The study period was one year from 1st January 2010 to 31st December 2010. Fifty cadavers who were dissected in the department during routine dissection process were included in the study. The dissection was carried out as per Cunningham‘s manual. Observations are mainly carried out for the placement of ECA and ICA ande the findings were noted down.
RESULTS
Anterolateral position of ECA on right side was found in one cadaver out of 50 cadavers dissected [2%]. The route of same variant artery found in an approximately 50 year male cadaver is given below:-
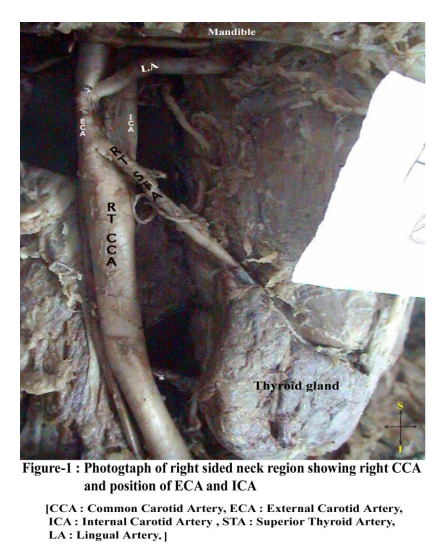
[a] Normal bifurcation of right CCA at the level of upper border of lamina of thyroid cartilage where it terminated into external carotid and internal carotid arteries.
[b] The formation and initial course of right ECA and right ICA differed from the normal pattern i.e. ECA was situated anterolateraly and ICA was situated posteromedially [Figure-1].
[c] The anterior branches of ECA, the superior thyroid artery, lingual artery and facial artery crossed ICA to reach their destination and this is the cause for their increased length and course [Figure-1]. [d] The ICA on the right side was postero medial and normal in its course.
DISCUSSION
We observed this rare positional variation only on right side, where ECA was anterolateral and ICA was posteromedial. As per the available literature, Handa et al [1] mentioned that the first description of the lateral position of the ECA was reported by an anatomist Hyrtl in 1841.He described that medial or lateral ECA migration during embryogenesis may be responsible for this anatomical variation, Handa et al explained that, this variation may be age related, secondary to elongation and tortuosity of atherosclerotic carotid arteries. Prendes et al [2] observed an anatomic variant for the position of ECA at the carotid bifurcation in 5.3% of patients investigated by Doppler ultrasound and contrast angiography. In his study, ECA was posterolateral to the ICA. Ueda S et al [3], reported an unusual case of peripheral hypoglossal nerve palsy caused by lateral position of the ECA and with an abnormally high position of bifurcation of CCA. The patient improved after cutting and ligation of ECA at its origin, which is due to compensatory dilatation of anastomotic arteries. Bergman et al [4] explained that:-[a] The ECA may be absent unilaterally or bilaterally. [b] When unilaterally absent, the branches, usually derived from it, arose from the CCA or from the contralateral vessel through anastomosis. [c] The artery may be located superficially and run lateral to the stylohyoid muscle or between the posterior belly of digstric muscle and the stylohyoid. J.P. Trigaux et al [5] performed intravenous digital subtraction angiography to determine the positional variations of the common carotid bifurcation and course of ECA and ICA in 100 consecutive patients with clinically suspected arteriosclerotic diseases. They observed [a] the position [97/200; 46.5%] of the ECA was anteromedial to the ICA. [b] Position of the ECA anterolateral to ICA was noted in 20/200 [13%]. [c] But the anatomical variant was more common on the right [21/100 than on the left [5/100].
According to Bussaka et al [6], lateral position of ECA is seen in 17 cases [4.3%] of which 13 cases were on the right side and 4 cases on the left. They expressed that it is necessary know this rare position of ECA, to avoid unnecessary complications during carotid endarterectomy. They emphasized that it is very important to ensure that the artery being ligated is ECA rather than ICA, as ligation of the latter cause‘s high risk of hemiparesis. MC Rusu et al [7] observed during dissections, a rare anatomical unilateral variant in the right carotid triangle of a adult male. They observed that the CCA on right side bifurcated slightly above the normal level, but the ECA was posterolateral to the ICA and its anterior branches initially crossed anterior to the ICA before continuing with a normal anatomical course. M.A Bailey et al [8] observed that. [a] In 2 cadavers [ aged 82 and 83] Right ECA was lateral. [b] The superior thyroid, lingual and facial arteries coursed medially, and partially obscured the ICA thus potentially limiting surgical access to the vessel. [c] They stated that when this anomaly is encountered during carotid endarterectomy initial recognition is crucial in order to preserve the hypoglossal and internal laryngeal nerves during ICA exposure. They expressed that this problem can be facilitated by circumferential ECA dissection and medial mobilization to reveal the lateral surface of the ICA. [d] They stressed that, the vagus nerve, located deep to the ECA, must also be identified and preserved while performing any neck surgery. Jasmin Delic et al [9] investigated the mutual relation of the initial parts of the ICA and ECA, as well as the height of crossing these blood vessels. They evaluated 50 patients by using magnetic resonance imaging of the neck and observed that [a] ECA is placed medially and coursed anterior to the ICA in 90% of cases. [b]In 7% of cases the right ECA was placed lateral to the ICA. [c] The ICA and ECA crossed approximately 3.04 cm above the bifurcation (at right 3.05 cm and at left 3.12 cm) and the height of the crossing varies from 1.3cm to 4.2cm (at right 1.3cim to 4.2cm, and the left 1.5cm to 4.1cm). [d] The height of crossing is symmetric in 18% of cases. They explained that the inversed disposition of the ICA and ECA must be held in mind while performing arterial ligatures in the carotid triangle, to avoid damage to the ICA and haemorrhagic accidents.
CONCLUSION
Our observation of anterolateral position was in one cadaver out of 50 present on right side [2%]. Though rare, positional variation of ECA and its branches must be observed by every surgeon while performing any surgery in neck. Prior angiographic and USG observation will be helpful for a proper planning of surgery and for better prognosis.
References:
1. Handa J, Matsuda M, Handa H. Lateral position of the external carotid artery, report of a case, Radiology 1972 ; 102 ; 361 - 2
2. Prendes JL, Mckinney
WM, Buonanno FS, Jones AM, Anatomic variations of the carotid bifurcation affecting Doppler scan interpretation J. Clin. Ultrasound 1980; 8: 147 - 50
3. Ueda S, Kohyama Y, Takase K; peripheral hypoglossal nerve palsy caused by lateral position of external carotid artery by an abnormally high position of bifurcation of the external and internal carotid arteries, a case report stroke 1984; 15 : 736 - 9.
4. Bergman RA, Thomson SA, Afifi AK, Saadeh FA, compendium of human anatomicvariations, Urban and Schwarzenberg, Baltimore-Munich 65, 1988.
5. J.P. Trigaux, MD, F.Delchambre, MD and B.Van Beers MD, Anatomical variations of the Carotid bifurcation: implications for digital subtraction angiography and ultrasonography, The British Journal of Radiology, 1990, 63, 181-185.
6. Bussaka H, Sato N, Oguni T, Korogi M, Yamashita Y, Takahashi.M, Lateral position of external carotid artery G. Rhinso Hoshasen 1990; 35 : 1061 - 3.
7. M. C. Rusu, A. Vasilescu and V. Nimigean published Elsevier Ltd. Volume 35, issue 11, Novemeber 2006, pages 1066 - 1067.
8. M.A. Bailey, D.J.A. Scott, R.G. Tunstall, M.J. Gough Lateral External Carotid Artery: Implications for vascular surgeon. European Journal of Vascular and Endovascular Surgery 2007, Vol. 34, Issue 4, Page 492.
9. Jasmin Delic, Alma Bajtaveric, Eldar Isakavic : positional variations of the external and internal carotid artery 2010 Acta medica Saliniana.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





