IJCRR - 3(5), May, 2011
Pages: 17-22
Print Article
Download XML Download PDF
A CLINICOPATHOLOGICAL STUDY OF ADENOMYOSIS AT HYSTERECTOMY
Author: Ramesh B.H, Shashikala P, Manjula, Doddikoppad, Chandrasekhar H.R
Category: Healthcare
Abstract:Background: Adenomyosis is a relatively frequent finding in the series of hysterectomies preformed for menorrhagia and dysmenorrhoea. In spite of the fact that it causes distressing and often serious functional
disturbances requiring major operation for correction, many physicians, even gynaecologists have only a
passing acquaintance with this entity.
Aim: The present study sought to evaluate the clinopathological aspects of adenomyosis. Materials and Methods: The present study is a descriptive analysis of 896 hysterectomies received to the department of pathology J.J.M Medical College, Davangere, for a period of 2 years. Adenomyosis
reported in 896 (49.04%) of 1827 uteri were included in the study irrespective of the preoperative
diagnosis. When adenomyosis was found it was recorded and graded as to depth of penetration and degree
of involvement.
Results: The prevalence of adenomyosis in 1827 hysterectomy specimen was 49.04% (896). Age of patients ranged from 20 \?75 years. The parity ranged from one to ten. Menorrhagia was the commonest
symptom. Leiomyoma was the common associated pathological lesion. In correlating adenomyosis with
clinical symptoms, menorrhagia and dysmenorrhoea increases in frequency as the depth of penetration
and degree of involvement of adenomyosis increases.
Conclusion: Adenomyosis is not a rare histopathological finding. Available evidence seems to generate
uncertainty regarding a casual relationship between adenomyosis and the symptoms attributed to it.
Majority of the patients with adenomyosis presented with various clinical features, which were clinically
attributed to associated diseases.
Keywords: Adenomyosis, Parity, Grading
Full Text:
INTRODUCTION
Adenomyosis was first described by Rokitansky in 18601 . In spite of long cognizance and many publications regarding adenomyosis there is still widespread disagreement as to its incidence, theories of origin, and associated pathology. Hyperestrinism has been frequently cited as the initiating factor in adenomyosis. This has never been substantiated, but the frequent association of endometrial hyperplasia and myomas with adenomyosis certainly tends to link adenomyosis in some way with uncompensated estrogen stimulation in many cases2 .
In reviewing the literature, adenomyosis is indeed an ?elusive? lesion. There are several reasons for this. First, the exact aetiology of adenomyosis is not known. Second, its precise incidence in surgical specimens is not known and variance between 8% - 40% is reported, depending on which study or text one reviews. Certain reviews reports a correct pre-operative diagnosis is less than 10% of the instances of proved adenomyosis3 . In spite of the fact that it causes distressing and often serious functional disturbances requiring major operation for correction, many physicians, even gynaecologists have only a passing acquaintance with this entity2 . In 60 to 80% of women with this condition also have other associated pelvic diseases such as leiomyomas, endometriosis and endometrial polyps. According to some authors, this frequent association tends to indicate hyperestrogenism as a common denominator4 . The present study sought to evaluate the clinopathological aspects of adenomyosis.
SUBJECTS AND METHODS
During the study period of 2years 1827hysterectomy specimens were received in the department of pathology J.J.M Medical College, Davangere. These specimens were fixed in 10% formalin for 24-48 hrs. Gross morphology of uterus with associated pathology was noted. Tissue bits from representative areas (3-6 blocks) were taken for histopathology examination. Multiple sections of 5 microns thickness stained with haematoxylin and eosin were studied. Adenomyosis reported in 896 uteri irrespective of the preoperative diagnosis were included in the study. The diagnostic criteria used in the identification was the presence endometrial glands and stroma at least one low power field below the basal layer of endometrium surrounded by myometrium. When adenomyosis was found it was recorded and graded as to depth of penetration and degree of involvement3 . Based on depth of penetration Grade I: one low power field below the basal endometrium, Grade II: penetration to mid myometrium and Grade III - penetration beyond mid myometrium. With respect to degree of Involvement were categorized as Slight: few (1-3) endometrial glands / low power field, Moderate: several (4- 9) endometrial glands / low power field and Marked: many (10 or more) endometrial glands/ low power field. These pathologic results were then reviewed and an attempt was made to correlate the pathologic findings with data, preoperative diagnosis and other clinical parameters.
RESULTS
Of the 1827 hysterectomy specimen received during the 2year period, adenomyosis was reported in 896 uteri (49.04%).
Patient profile
Age of patients ranged from 20 – 75 years with a mean age of 39.8years. Peak incidence was seen in fourth decade with 48.43% cases. Of these 892 patients were parous (99.55%) and only four were nulliparous (0.45%). The parity ranged from one to ten. Menorrhagia was the commonest symptom [Figure 1].
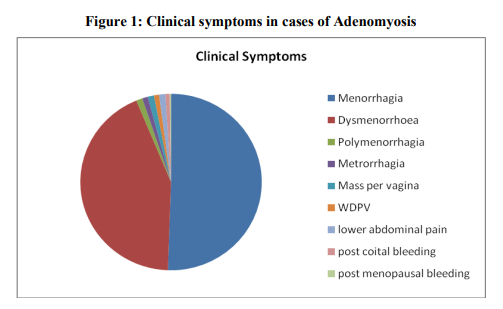
Histomorphology Of the 896 uterus studied, 475(53%) cases were normal in size, 391(43.64%) were bulky and only 30(3.36%) uteri were atrophic. On cut section, myometrium showed characteristic coarse trabeculated appearance which was diffuse in 677(75.55%) uteri and focal in 189(21.09%) uteri. However it was difficult to appreciate these features in 30 atrophic uteri. Small cyst like spaces with dark brown areas was observed in 150 adenomyotic uteri. 122(13.61%) uteri were associated with leiomyomas. Microscopically grade I adenomyosis was encountered in 528 uteri (58.93%), Grade II in 340 uteri (37.95%) and 28 uteri (3.12%) showed Grade III adenomyosis. Analysis of the degree of involvement of adenomyosis, slight or mild degree was commonest encountered in 580(64.73%) uteri followed by moderate involvement in 281 (31.36%) uteri and severe degree in 35(3.91%) uteri. Endometrial changes in Adenomyotic uterus: Proliferative phase was seen in 471 cases (52.56%) followed by secretary endometrium in 296 cases (33.04%) and cystic glandular hyperplasia in 72 cases (8.04%). Atrophic endometrium was found in 57 cases (6.36%). In 326 (36.38%) cases various associated pathological lesions were observed along with adenomyosis [Table 1].
DISCUSSION
The true incidence of adenomyosis is unknown. The frequency of adenomyosis reported in the literature ranges widely from 5 to 70%. The incidence of adenomyosis in the present study was 49.04% and preoperative clinical diagnosis of adenomyosis was done in only 31 cases (3.46%) similar to other studies1-3,5 .
Age/parity
In the present study the peak age incidence of adenomyosis was in fourth and fifth decades (73.88%) which is in accordance with other studies1-3,8. Adenomyosis typically affects multiparous patients1,4. In our study, most of the patients were multiparous (99.55%) as comparable to other studies2-4, 8,9. The overwhelming population of parous patients in various studies lends support to the concept that child bearing may play a role in the aetiology of adenomyosis2 .
Symptoms
The symptom association with adenomyosis is excessive uterine bleeding accompanied by worsening dysmenorrhoea. However adenomyosis may be entirely asymptomatic3,4. In the present study, incidence of menorrhagia in patients with adenomyosis was 50.55% similar to other studies3,7. Dysmenorrhoea from present study correlates with other studies1-3,6,7. As with other studies in the present study reported symptoms in cases of adenomyosis were heterogenous, nonspecific and probably related to the associated diseases4
Histomorphology
Diffuse enlarged uterus that is soft and tender on palpation is associated with adenomyosis3 . In the present series, adenomyotic uterine size was normal in 53% of cases, slightly enlarged or bulky in 43.64% of cases and was atrophic in 3.36% similar to other studies2 . This study shows that adenomyosis is not always associated with clinically demonstrable uterine enlargement, unless associated with leiomyomas similar to other studies2 . Grade I adenomyosis was commonest, found in 58.93% of uteri, followed by Grade II in 37.95% and Grade III in 3.12% in accordance with other studies3 . Present study showed mild adenomyosis in 64.73%, moderate degree in 31.36% and severe degree in 3.91% of uteri in contrast to other studies3 .
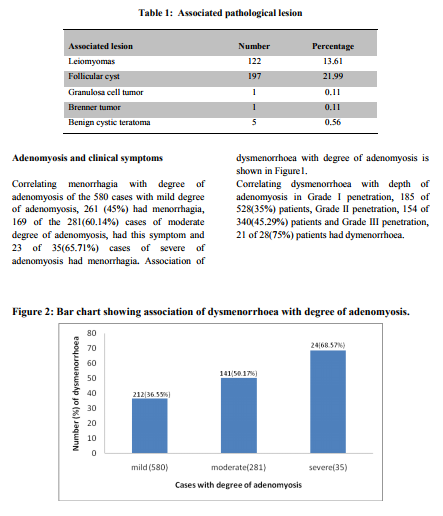
Association of Adenomyotic uteri with Clinical symptoms
Incidence of menorrhagia is directly proportional to the degree of involvement3 . With respect to degree of involvement the results in the present study was in accordance with other studies3 that, as the degree of involvement increases more frequent is the occurrence of menorrhagia. Present study shows dysmenorrhoea correlated with depth of penetration and degree of involvement Similar to other studies3, 4,11. which showed dysmenorrhoea increases in frequency as the depth of penetration and degree of involved increases, which substantiates Halls hypothesis3 .
Association of adenomyosis with other uterine pathology
In the present study, most of the uteri with adenomyosis showed proliferative phase (52.56%) followed by Secretory phase (33.04%), endometrial hyperplasia (8.04%) and atrophic in 6.36% of uteri which are in accordance with other studies2-4 . Present study shows additional pelvic pathology in 36.38% of adenomyotic uteri which is less in comparison to other studies2 . The incidence of leiomyoma in our study (13.61%) is similar to other studies7, 10,12 .
CONCLUSION
Adenomyosis is not a rare histopathological finding. Available evidence seems to generate uncertainty regarding a casual relationship between adenomyosis and the symptoms attributed to it. Majority of the patients in this study with adenomyosis presented with various clinical features, which were clinically attributed to associated diseases.
References:
1. Azziz R. Adenomyosis: Current perspectives. Obstet Gynaecol Clinics of North America 1989; 16: 221-35.
2. Molitor J. Adenomyosis: A clinical and pathologic appraisal. Am J Obstet Gynaecol 1971; 110: 275-84.
3. Bird CC, Mcelin TW, Manola EP. The elusive adenomyosis of the uterus- revisited. Am J Obstet Gynaecol 1972; 112: 583-89.
4. Vercellini P, Ragni G, Trespidi L, Oldani S, Panazza ,S.et al: Adenomyosis: A Déjà vu ? Obstet and Gynaecol Survey 1993; 48: 789-94.
5. Vercellini P, Parazzini, Oldani S, Panazza S, et al. Adenomyosis at hysterectomy; a study on frequency distribution and patient characteristics. Human reproduction: 1995; 10:1160-2.
6. Kilkku P, Erkolla R, Gronroos M. Non specificity of symptoms related to adenomyosis: A prospective comparative survey. Acta Obstet. Gynaecol. Scand 1984; 63: 229-31.
7. McCausland A.M. Hysteroscopic myometrial biopsy: Its use in diagnosing adenomyosis and its clinical application. Am. J. Obstet. and Gynaecol 1992; 166:1619-28.
8. Wéry O, Thille A, Gaspard U, van den Brûle F. Adenomyosis: update on a frequent but difficult diagnosis. Gynaecol obstet Biol Reprod 2005; 34:633-48.
9. Bergholt T, Eriksen L, Berendt N, Jacobsen M, Hertz JB. Prevalence and risk factors of adenomyosis at hysterectomy. Hum. Reprod 2001;16: 2418-21
10. Yeniel O, Cirpan T, Ulukus M, Ozbal A, Gundem G, Ozsener S et al. Adenomyosis: prevalence, risk factors, symptoms and clinical findings. Clin Exp Obstet Gynecol. 2007; 34: 163-7.
11. Sammour A, Pirwany I, Usubutun A, Arseneau J, Tulandi T. Correlations between extent and spread of adenomyosis and clinical symptoms. Gynecol Obstet Invest. 2002; 54 :213-6.
12. Taran AF, Weaver AL, Coddington C, Stewart EA. Characteristics indicating adenomyosis coexisting with leiomyomas: a case–control study. Hum. Reprod 2010; 25: 1177-82.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





