IJCRR - 3(8), August, 2011
Pages: 144-148
Print Article
Download XML Download PDF
THE ROLE OF HOME BASED VESTIBULAR REHABILITATION IN THE TREATMENT OF CHRONIC PERIPHERAL VESTIBULAR DISORDER -A RANDOMISED CONTROLLED TRAIL
Author: Vaishali K, Kishore Chandra Prasad, Jeganathan, Sampth Chandra Prasad
Category: Healthcare
Abstract:Vertigo is defined as the illusory sensation of motion, either of the body or of the surrounding
environment, occurring while an individual is stationary. It is often associated with a feeling of spinning,
nausea, emesis and diaphoresis. The aim of the study is to evaluate the long term home based effect of
vestibular rehabilitation on activity of daily living in peripheral vestibular disorder. Method twenty
patients with chronic peripheral vestibular disorder were randomly assingned into two groups. Control
group(only medication) and experimental group (vestibular habituation). The patients were assessed
using VADL intially at the commencement of the study, at end of three months, six months and end of
twelve months for both the groups. Vestibular disorder Activity of Daily Living Scale (VADL) is is a 28
item, 10 point self administered scale of self perceived indepented in ADL. The scale has 3 subscales:
functional, ambulation, and instrumental Result: The mean age of 43.40 \? 16.84 were included in the
study. The total VADL and all the sub scores of VADL, functional, ambulatory and instrumental
showed a very highly significant change in the intervention group following treatment. Conclusion: The
activity of daily living improved following home based vestibular rehabilitation as compared to the
control group with only medication.
Keywords: Vestibular Rehabilitaton, Chronic vertigo, Dizziness, Vestibular disorder Activity of daily living, peripheral vestibular disease.
Full Text:
INTRODUCTION
Vertigo is defined as the illusory sensation of motion, either of the body or of the surrounding environment, occurring while an individual is stationary. It is often associated with a feeling of spinning, nausea, emesis and diaphoresis.1 Vertigo can result from lesions in the inner ear; the deep paravertebral stretch receptors of the neck, the visual/vestibular interaction centres in the brainstem and cerebellum, and in the subjective sensation pathways of the thalamus or cortex.2 Lesions of the vestibular system may result in peripheral vertigo which includes vestibular neuritis, benign paroxysmal positional vertigo, Meniere‘s disease, labyrinthitis.1The treatment is symptomatic with antivertiginous medication. The main intervention for chronic peripheral vertigo is vestibular rehabilitation.3 It involves various movement-based regimes. Components of vestibular rehabilitation involve learning to bring on the symptoms to ?desensitise‘ the vestibular system, learning to coordinate eye and head movements, improving balance and walking skills, learning about the
condition
and how to cope or become more active.4 There is very limited data to claim the home based, long term effect of vestibular rehabilitation in chronic peripheral vestibular disorders. The aim of the study is to evaluate the long term home based effect of vestibular rehabilitation on activity of daily living in peripheral vestibular disorder.
METHOD
The study was approved by the institutional ethical committee.This was a prospective study conducted in patients with uncompensated vestibular dysfunction as diagnosed by an Otolaryngologist, in a vertigo out patient clinic.The patients were screened for inclusion and exclusion criteria. Inclusion criteria – Patients with chronic peripheral vestibular vertigo of at least one year duration not cured by medications were included in the study with diagnosis of Benign Positional Paroxysmal Vertigo, Labyrinthitis, Vestibular Neuronitis, Meniere‘s disease, local trauma. Exclusion criteria – Patients with vertigo due to middle ear causes like effusions, perilymphatic fistula, Otosclerosis and Mastoiditis were excluded from the study. Written informed consent was taken and were randomly assingned into two groups- control group(only medication) and experimental group (vestibular habituation). Pre treatment Vestibular disorder Activity of Daily Living scale(VADL) were taken.The control group patients took vestibular supressent medication.The intervention group were treated with vestibular habituation exercise. The intervention group attended during the first week, a series of vestibular habituation program for 30-45 minute sessions. Subsequesntly the patients were instructed to continue the same vestibular habituation for an year, once a day, at home independentaly. A audio cassette and written home exercise program was given.The patients were assessed intially at the commencement of the study, at end of three months, six months and end of twelve months for both the groups. The vestibular habituation exercises were Encourage vestibular adaptation by inducing retinal slip which includes X1 viewing paradigm (horizontal and vertical, Eye Head Exercise horizontal and vertical, Remembered target exercise) and X2 Viewing Paradigm. Exercise to encourage resetting of VOR gain at various head speeds were given given to improve the vestibulo-ocular system, Improve ability to utilize somatosensory & vestibular input for postural control were given. The control group were on vestibular labryrinthin sedative medication as prescribed by the otolaryngologist. At the end of one year, Vestibular disorder Activity of Daily Living Scale (VADL) was assessed.Vestibular disorder Activity of Daily Living scale (VADL) – This is a 28 item, 10 point self administered scale of self perceived indepented in ADL. It adressess 3 domains of occupation: basic self maintainance task, mobility skills and higher level or more socially complex tasks within and outside home. The VADL scale assesses the impact of vestibular impairment on everyday activities. The 28 items are grouped into three dimensions: functional (self-care andintimate activities), ambulation (walking and stair climbing), and instrumental (home management and leisure activities) The final scale has 3 subscales: functional, ambulation, and instrumental. It has good face validity, high internal consistency ( .90), and high test-retest reliability (rc 0.87). Scale ratings ranged from 1 (independent) to 10 (ceasing to participate in the activity).5 Data analysis were done using SPSS 13 version software. Vestibular disorder Activity of Daily Living scale (VADL) scales were analyzed using nonparametric test. Multiple comparisons with in the groups and between groups were analyzed using Wilcoxon Signed Rank Test and Mann-Whitney test respectively.
RESULTS
Twenty patients (7 males and 13 females) with a mean age of 43.40 ± 16.84 were included in the study. Through block randomisation they were divided into control and intervention group. The total VADL and the sub scores functional (p <0.001), ambulation (p <0.001), instrumental (p <0.001) showed a very highly significant in the vestibular rehabilitation group as compared to the control group. Of the ten there were two lost for follow up in intervention group as they shifted their residence and three lost for follow up in the control group as they had opted for alternate treatment therapy. Only eight in the intervention group and sevent in the control group were analysed. A dairy was given to the intervention group 85% of them was complaint with their exercise.
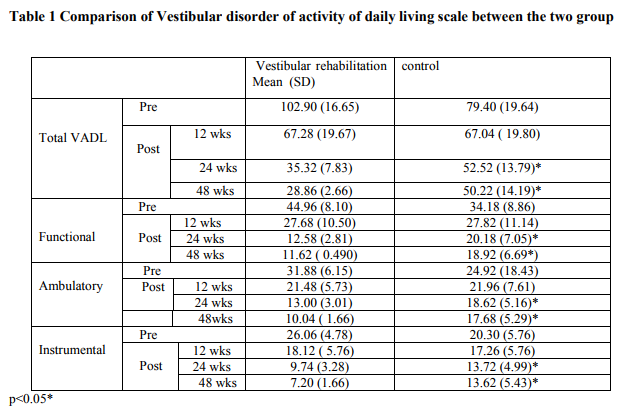
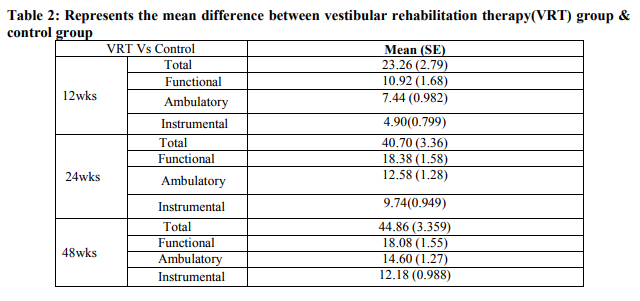
DISCUSSION In the present study all the patients showed improvement with respect to vestibular activity of daily living scale following one year of home based vestibular rehabilitation in the vestibular rehabilitation group as compared to the control group as the mean difference in the total vestibular activity of daily living scale between group at the end of one year was 44.86. In our study the patients reported confidence in their activity of daily living by the third month and continued to improve by the sixth month and they maintained their improved level of confidence up to one year as they adhered to their exercise regime. Our study is in agreement with Mira et al review who also reported improvement in the quality of life following vestibular rehabilitation.6 Where as Topuz et al in his eight week study reported that better improvement in supervised exercise session as compared to home exercise session.7 Vestibular rehabilitation is an exercise based program, designed to maximise central nervous system compensation for vestibular pathology.3The exercises are supposed to accelerate and improve central compensation via the mechanism of habituation training, with enhanced adaptation of vestibule-ocular reflex and vestibule-spinal reflex.8,9 There was improvement in the independence in the activities of daily living score in the vestibular rehabilitation group as compared to the control group. The most likely cause of improvement in the functional skills was because of decrease in the intensity of vertigo as vestibular rehabilitation accelerate compensation and medication act to suppress the labyrinthine. Since subject felt better, moving their head did not elicit vertigo, so they were better able to engage in self care, mobility, home management and vocational activities. Subjects had previously avoided these activities, needed assistance to perform them, or had performed them more slowly or carefully than usual. Increased participation in daily life tasks and related increased activity levels may have generated more head movements, facilitating the effects of habituation exercise. Unlike previous reports which used repeated visits of out patient therapy, the results of this study suggest that, a home program of vestibular habituation is sufficient to reduce their symptoms. Rapid return to independence in routine daily life task, including occupational role, is an important psychological benefit.
CONCLUSION
The activity of daily living improved following home based vestibular rehabilitation as compared to the control group with only medication.
References:
1. Raman Abrol, Vikas I Nehru, Y Venkataramana Prevalence and etiology of vertigo in adult rural population. Indian journal of otolaryngology and head and neck surgery 2001; 53: 32-36.
2. Robert W Baloh. Vertigo. Lancet 1998;352:1841–46.
3. Oya Topuz et al. Efficacy of vestibular rehabilitation on chronic unilateral vestibular dysfunction. Clinical rehabilitation 2004; 18: 76-83.
4. Hillier SL, Hollohan V. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction (Review) the Cochrane library 2008, issue 4:1-38.
5. Cohen HS, Kimball KT. Development of the vestibular disorders activities of daily living scale. Arch Otolaryngol Head Neck Surg. 2000; 126: 881-887.
6. Mira E. Improving the quality of life in patients with vestibular disorders: the role of medical treatments and physical rehabilitation. Int J Clin Pract, 2008; 62(1): 109-114.
7. Topuz O, Topuz B, Necdet NA. Efficacy of vestibular rehabilitation on chronic unilateral vestibular dysfunction. Clin Rehab 2004; 18: 76–83.
8. M.Igarashi Vestibular Compensation, an overview. Acta Otolaryngol (stockh) 1984; suppl. 406: 78-82.
9. Helen S Cohen, Kay T Kimball increased independence and decreased vertigo after vestibular rehabilitation Otolaryngol Head Neck Surg 2003; 128: 60-70.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





