IJCRR - 3(9), September, 2011
Pages: 127-133
Print Article
Download XML Download PDF
EVALUATION OF THE CONTAMINATION AND EFFECTIVE DISINFECTION OF TOOTHBRUSHES USED
BY CHILDREN
Author: Auxilia Hemamalini Tilak , Stanica Prasath , Lakshmi.T
Category: Healthcare
Abstract:Introduction : Previous studies have indicated that a S. mutans is the most common bacteria implicated in the causation of dental caries. It has also been documented that S. mutans can easily colonise tooth brushes. S. mutans count as high as 106 has been recovered few minutes after brushing and a count as high as 104 is being retained after 24 hours after storage. The retention and survival of S. mutans poses a threat of reinfection. Numerous studies has been done to evaluate the effectiveness of 12% chlorhexidine, 1% sodium hypochlorite and normal saline as toothbrush disinfectants and research personnel have shown that chlorhexidine and sodium hypochlorite are very effective in disinfection. None have established the effective time for complete disinfection. None have addressed the question if the disinfected toothbrushes can be used again. We have in this study tried to standardize a time frame for effective disinfection and the effective concentration using a highly affordable and easily available disinfectant and most importantly with the Indian mother in mind. The purpose of this present investigation is to study the 1) In vivo contamination by mutans streptococci (MS) of toothbrushes after use on 72 children (6- 12years old) visiting a single physician.
2) To evaluate .9% normal saline as a toothbrush disinfectant.
3) To standardize the time for effective disinfection .
4) To prove that .9% normal saline when used as a toothbrush disinfectant for the right time is much superior than .12% chlorhexidine and 1% sodium hypochlorite in many ways.
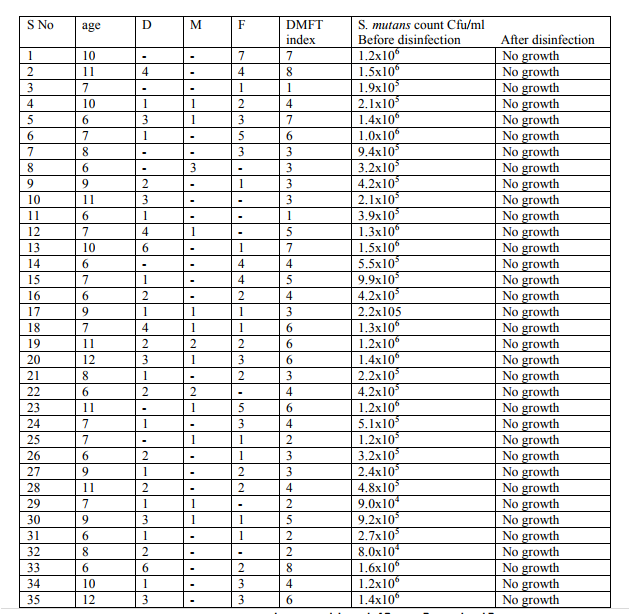
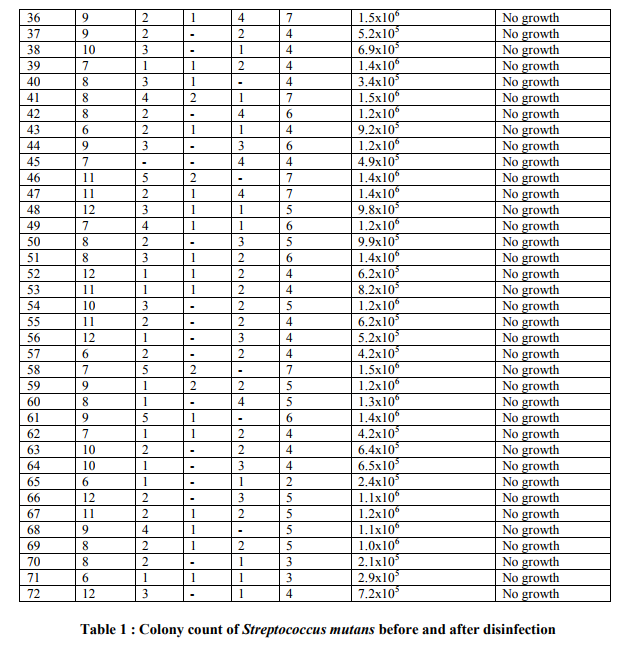
Materials & Methods: The in use toothbrushes(less than 3 months of use) of 72 children whose DMFT indexes are already in record were submitted for S. mutans count and they were provide with new toothbrushes. The new toothbrushes were to be put to use for a month and then submitted to the physician's office at the stipulated date within an hour after the routine morning brushing. They were immediately analyzed for S.mutans count after 15 minutes, 30 minutes, 1hour and 8 hours of being treated with .9%NS. There was no reduction in the CFU after 15min, 30 min and 1 hour but there was an absolute reduction in the cfu after 8 hour disinfection in .9% NS. All these brushes were returned to the children after a routine tap water rinse and were put to regular use in the night. The parents have not reported any problem with putting them to reuse after disinfection with .9%NS. Conclusion: These results have addressed the concept of cheap, effective and user friendly routine house
based toothbrush disinfection between use.
Keywords: Dental caries , Streptococcus mutans , Tooth brush, Disinfection, Colony count, Children, DMFT index.
Full Text:
INTRODUCTION
Dental caries is widely recognised as an infectious disease induced by diet. The main players in the aetiology of the disease are; a) cariogenic bacteria( especially S mutans), b) fermentable carbohydrates, c) a susceptible tooth and host and d) time. However, in young children bacterial flora and host defence systems are in the process of being developed, tooth surfaces are newly erupted and may show hypoplastic defects, and their parents must negotiate the dietary transition through breast/bottle feeding, first solids and childhood tastes. Thus it is thought that there may be unique risk factors for caries in infants and children .It is disconcerting to see rampant caries in young children.The pattern of decay is typically that many teeth are affected, with caries developing rapidly, often soon after the teeth have erupted. Surfaces usually at low risk of developing caries are the buccal surfaces of maxillary incisors with the obvious consequence of affecting the child‘s facial appearance. Dietary habits such as increased consumption of carbohydrates and junk food increases the incidence of caries in the deciduous molars with subsequent loss of the most important natural space maintainers of a young child resulting in malocclusion in permanent dentition. Hence, keeping in mind age old adage ?prevention is better than cure? every precautious step should be taken to minimize the occurance of caries. The continuous accumulation of oral bacterial plaque is the most important forerunner of dental caries1. Hence the mechanical disruption by brushing with a tooth brush is the most favoured method for disruption of the plaque in children2 However certain bacteria such as S.mutans may colonise toothbrushes and recontaminate the oral cavity when used again. Several bactericidal agents have been tried as prospective candidates for routine toothbrush disinfection such as chlorhexidine3,brushtox4, UV light activated tooth brush sanitizer5 and several dentrifices6, 7,8. But none has been approved so far as a home based routine between use toothbrush disinfectant . The reasons may be that they may be expensive, time consuming, needing equipment and procedures not suitable for routine use not to mention the after taste due to product residues.
MATERIALS AND METHODS
Sample 1:
100 children between the age group 6-12 years visiting a single physician cum dentist and whose DMFT indexes were on record, were enrolled in the study. They were healthy children with no other local or systemic disorders and who were on a routine twice a day oral hygiene maintenance. The parents of the 72 children brought their child‘s toothbrush which was in use for less than 3 months and within 1 hour of use after a routine dental cleansing in the morning. They were immediately processed. Brand new toothbrushes were given to the parents in exchange and the second date of sampling(after a month) was preset.
Sample 2: The second set of 72 toothbrushes used by the same children were again submitted after 1 month, after routine morning cleansing and within 1 hour of usage and were immediately put in .9% saline and processed.
Bacterial Culture
Sample 1:
Methods employed for bacterial culture followed standard techniques9 . Media included tryptose soya broth and Mutans sanguis agar. For bacterial extraction the toothbrushes were individually placed in pre-labelled sterile 50 ml test tubes containing 10ml of tryptose soya broth (TSB) to completely immerse the bristles and vortexed vigorously for 1 minute squeezed against the sides of the test tube to drain. Then 1µl of this was plated on to Mutans sanguis agar in triplicate and incubated for 37°C for 24 hours. The number if colonies were measured as colony forming units per ml.
Sample 2:
The toothbrushes were placed individually in prelabelled sterile 50ml test tubes containing 10 ml of .9%NS vortexed vigorously for 1 minute and kept aside at room temperature.1µl of the resulting disinfectant was subjected to bacterial counts on Mutans sanguis agar after 15 minutes, 30 minutes, 1 hour and 8 hours.
RESULT
According to several authors 11-14, the presence of decayed teeth increases significantly the S. mutans counts in saliva. The above tabular column shows the correlation of a high DMFT score with increase in the bacterial count before disinfection. But after 8 hours of disinfection in normal saline, the bacterial count is completely eliminated irrespective of the DMFT score. Thus, the above study clearly indicates that saline is one of the most effective yet easily available disinfectant for the Indian Mother, who plays a pivotal role in maintaining the overall health of her children
DISCUSSION
Every parent keeps their finger crossed until the first sign of tooth eruption. Teeth are important not only for mastication, but also for aesthetics and phonetics. Deciduous teeth are especially important, as they are the best natural space maintainers15. Any premature loss of primary teeth , especially deciduous molars will result in mesial migration of permanent 1st molars, thereby resulting in impacted premolars, and also various malocclusion problems16,17 necessitating orthodontic treatment later on in life. Caries in primary anteriors affects the psychology of children. Children hesitate to smile and talk properly because of the carious primary incisors, thereby becoming the victim of unnecessary bullying and pranks. Hence every care should be taken to prevent the progression of dental caries. Dental caries is one of the most common causes of premature loss of deciduous teeth 17. The beginning and progression of dental caries are influenced by several risk factors, including bacterial, dietary, environmental and socioeconomic factors. The most significant indicators of caries risk are past caries experience, concentration of S. mutans and Lactobacilli, and the presence of protective factors like the buffering capacity of saliva. Any unbalance between protective and risk factors results in growth of specific microorganisms (S. mutans and Lactobacilli), which are part of the human dental biofilm18 and are considered the main acidogenic andaciduric organisms associated with dental caries.18-20 Dietery habits of children facilitate the progression of dental caries. Frequent intake of chocolates, junk foods, improper brushing technique , consumption of milk before bedtime, and the morphology of deciduous teeth are the various other common factors of dental caries 21. One of the most common and simple methods of preventing caries is mechanical method of removal, i.e., using a tooth brush. Every child dreads to brush everyday in the morning and so just pass the brush around the teeth in a fraction of second, and put it away even without rinsing the brush properly, inadvertently, contaminating the tooth brush with S mutans, and facilitating its growth.22. When in use the next day, the teeth are further contaminated by the brush, hence the need to disinfect the brush to prevent reinfection23. This study ensure that a simple, home product, economical, easy to use yet effective disinfectant is made available to parents, to ensure that proper oral hygiene is maintained for children. The timings for disinfection were chosen keeping in mind the purpose of the study. 15minutes, 30 minutes and 1hour were chosen as they would be ideal timings in case the mother contemplates disinfecting the child‘s toothbrush early in the morning before the child performs his morning toothbrushing act. 1 hour was chosen, as this period of time would be ideal for an overnight disinfection after a routine bedtime brushing. While after 15 min, 30 min and 1 hour of immersing in normal saline there was no considerable drop in Streptococcus mutans count, there was absolute disinfection after 8 hours of immersion in normal saline.
CONCLUSION
This study has addressed the concept of disinfection between use. The toothbrushes were put to routine use after disinfection in normal saline for 8 hours. They were washed in tap water to remove the salinity. There was no bad taste or odour that could adversely affect the use by children. Most importantly a bottle of normal saline costing about 30 rupees is going to hold good for a month. Hence in this study we have proven that simple, economical methods of disinfection can be advocated in our day to day lives to contribute to better dental hygiene for children.
References:
1. Holst D. Causes and prevention of dental caries: A perspective on cases and incidences. Oral Health Prev Dent 2005;3: 9-14
2. Franzman MR, Levy SM, Warren JJ, Broffitt B. Tooth-brushing and dentifrice use among children ages 6 to 60 months.Pediatr Dent. 2004 JanFeb;26(1):87-92.
3. Sato S, Pedrazzi V, Guimaraes LEH, Panzeri H, Ferreira del Albuquerque R, Ito IY. Antimicrobial spray for toothbrush disinfection: An invivo evaluation. Quitessence Int 2005: 36 :812-816
4. Neal PR, Rippin The efficacy of a toothbrush disinfectant spray. An in vitro study. J Dent 2003: 31: 153-157
5. RobertBoylan, Yihong li, Lidia Simeonova, Gene Sherwin, Judith Kreisman, Ronald G. Craig, Jonathan A. Ship, Jane A. McCutcheon. Reduction in bacterial contamination of toothbrushes nusing ultraviolet light activated toothbrush sanitizer. Am J Dent 2008: 313-317
6. Nelson-Filho P, Isper AR, Assed S, FariaG, Ito IY. Effect of triclosan dentrifice on toothbrush contamination. Pediatr Dent 2004:26:11-16
7. Quireynen M, de Soete M, Pauwels M, Goosens K, Teughels W, van Eldere J, van Steenberg D. Bacterial survival rate on tooth and interdental brushes in relation to the use of toothpaste. J Clin Periodontol 2001:28: 1106-1114
8. Warren DP, Goldschmidt MC, Thompson MB, Adler-Storthz K. The effect of toothpastes on the residual microbial contamination of toothbrushes. J Am Dent Assox 2001: 132:1241-1245
9. Isenberg HD, Baron EJ, D‘Amato RF, Johnson RC, Murray PR, Rodgers FG, vonGraevenitzm A. Recommendaitions for the isolation of bacteria from clinical specimens. Manual of clinical microbiology 5th edition Washington DC: American society for microbiology, 1991: 216-221
10. Sánchez-Pérez L, Acosta-Gío AE, MéndezRamírez I. A cluster analysis model for caries risk assessment. Arch Oral Biol. 2004; 49:719-25.
11. Zoitopoulos L, Brailsford SR, Gelhier S, Ludford RW, Marchant SH, Beighton D. Dental caries and caries-associated microorganisms in the saliva and plaque of 3- and 4-year old afro-caribbean and caucasian children in south London. Arch Oral Biol. 1996; 41:1011-8.
12. Petti S, Pezzi R, Cattaruzza MS, Osborn JF, D‘Arca AS. Restoration-related salivary Streptococcus mutans level: a dental caries risk factor? J Dent. 1997;25:257-62.
13. Seibert W, Farmer-Dixon C, Bolden T, Stewart JH. Streptococcus mutans levels and caries prevalence in low-income schoolchildren. J Tenn Dent Assoc. 2002; 82:19-22.
14. Laing E, Ashley P, Naini FB, Gill DS. space mainteinance. Int J Paediatr Dent. 2009 May; 19(3):155-62.
15. Craddock HL. Consequences of tooth loss: 2. Dentist considerations--restorative problems and implication .Dent Update. 2010 Jan-Feb; 37(1):28-32.
16. Hoffding J, Kisling E. Premature loss of primary teeth: part I, its overall effect on occlusion and space in the permanent dentition. ASDC J Dent Child. 1978 JulAug; 45(4):279-83.
17. Loesche WJ. Clinical and microbiological aspects of chemotherapeutic agents used according to the specific plaque hypothesis. J Dent Res. 1979; 58:2404-12.
18. Zickert I, Emilson CG, Krasse B. Streptococcus mutans, Lactobacilli and dental health in 13-14 year old Swedish children. Community Dent Oral Epidemiol. 1982; 10:77-81.
19. Kingman A, Little W, Gomez I, Heifetz SB, Driscoll WS, Sheats R, et al. Salivary levels of Streptococcus mutans and Lactobacilli and dental caries experiences in a U.S. adolescents population. Community Dent Oral Epidemiol. 1988;16:98-103
20. Moynihan PJ. Dietary advice in dental practice. Br Dent J. 2002; 193:563-8.
21. Filho PN, Macari S, Faria G, Assed S, Ito IY: Microbial contamination of toothbrushes and their decontamination. Pediatric Dentistry. 2000 22(5) 381-384.
22. Fratto G, Nazzicone M, Ortolani E. Disinfection of toothbrushes. Experimental research] Prev Assist Dent. 1990 Jan-Feb; 16(1):7-10.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





