IJCRR - 3(9), September, 2011
Pages: 89-95
Print Article
Download XML Download PDF
EFFICACY OF DEEP TRANSVERSE FRICTION MASSAGE ON SUPRASPINATUS TENDINITIS - A
RANDOMIZED PILOT TRIAL STUDY
Author: H.Karvannan, R.D.Chakravarty, V.Prem
Category: Healthcare
Abstract:Background Deep transverse friction massage (DTFM) is a technique popularized by Dr. James Cyriax for pain and inflammation relief in musculoskeletal conditions. The study aimed to assess the efficacy of DTMF on treating patients with supraspinatus tendinitis (SST) of the shoulder joint. Methodology A total 20 participants' (n=20) were met the inclusion criteria and were randomly allocated into the study and the control group in this pilot trial. A Pretest and Posttest measurement of Visual Analog Scale and Active Pain free shoulder Range of Motion was documented before and after the trial , Study group underwent DTMF , Therapeutic ultrasound, shoulder stabilization and strengthening exercises, the Control group underwent therapeutic ultrasound , shoulder stabilization and strengthening exercise. Dependent 't' test was used to show the effectiveness of interventions between groups.The data were analysed using SPSS 16.0 version (SPSS Inc., Chicago, Illinois, USA) Results Both the groups showed the significant reduction in the intensity of pain and increase in Active pain free Range of Motion of the shoulder Joint. The obtained ?t' value with independent ?t' test shows the study group is effective than control group. Conclusion Our results showed improvements on pain severity, and ROM of the patients SST with DTMF, therapeutic ultrasound and exercise. This study concludes DTMF are the valuable components in
the comprehensive rehabilitation of participants with SST of the shoulder joint.
Keywords: Deep Transverse Friction Massage, Therapeutic ultrasound, Supraspinatus tendinitis, Visual Analog scale, Range of Motion
Full Text:
INTRODUCTION
Conditions causing shoulder pain are common and contribute substantially to the musculoskeletal morbidity of the community1 . Moving the shoulder allows placement of the hand, hence compromised shoulder mobility impacts substantially on the performance of tasks essential to daily living (e.g. dressing, personal hygiene, eating and work). In addition, shoulder pain is often associated with impaired ability to sleep, so affecting mood and concentration. People with shoulder pain have been shown to score substantially less than normal values on the SF-36 (a standardised measure of general health) for physical function, social function, physical role function, emotional role function and pain2, 3 . Supraspinatus tendon of shoulder joint is particularly vulnerable to degenerative change, particularly in the elderly 4 . Codman 5 suggested the presence of a ?critical zone‘ of relative avascularity close to the point of insertion of the supraspinatus tendon. This may be affected by the position of the shoulder 6 and increase with age 7 . Moseley and Rothman and Parke reported the 'critical zone' at the supraspinatus tendon where the vasculature of this structure could be affected during movement. Chronic irritation of this poorly vascularized region may lead to an inflammatory response which in turn may cause tendinitis8, 9 . There are ample treatment used in the management of tendon disorders like Nonsteroidal anti-inflammatory drugs, Corticosteroid injections and various Physical therapy interventions ( cryotherapy , therapeutic ultrasound ,LASER, Manual therapy techniques like deep transverse friction massage, soft tissue mobilization, and Extra corporeal shock wave therapy ).10 Deep transverse friction massage (DTFM) is a technique popularized by Dr. James Cyriax for pain and inflammation relief in musculoskeletal conditions11,12. DTFM may be part of a physiotherapy program offered in the treatment of various musculoskeletal conditions. DTFM is a technique that attempts to reduce abnormal fibrous adhesions and makes scar tissue more mobile in sub-acute and chronic inflammatory conditions by realigning the normal soft tissue fibers 13, 14. It has been indicated that DTFM also enhances normal healing conditions by breaking cross bridges and preventing abnormal scarring. Its mechanical action causes hyperaemia, which results in increased blood flow to the area13 . There were only two randomized controlled trials on DTFM one on the treatment of extensor carpi radialis tendinopathy (lateral epicondylopathy) and the other on the iliotibial band friction syndrome15 . Studies could not be retrieved on DTFM on supraspinatus tendinitis, Hence the current Randomized pilot trial aimed to study the effectiveness of Deep Transverse Friction Massage on Supraspinatus tendinitis.
METHODOLOGY
A Randomized Pilot Trial study was conducted at Manipal Hospital Bangalore, Ethical approval has been taken from the Institutional review board and Informed consent was taken from the participants. Participants presenting with clinical signs and symptoms indicating supraspinatus tendinitis are recruited in this study. The inclusion criteria was age group between 18 and 75 years, and has a symptom of more than four weeks, main complaints in the glenohumeral joint region or the proximal arm, presence of one of the following signs indicating supraspinatus tendinitis: Neer impingement test, Hawkins-Kennedy impingement test, painful arc with active abduction or flexion, pain with one of the following resistance tests: external rotation, internal rotation, abduction, or flexion. Exclusion criteria was participants with diagnosed instability or previous history of dislocation, primary scapulothoracic dysfunction due to paresis, adhesive capsulitis (frozen shoulder), substantial shoulder weakness or loss of active shoulder function, shoulder surgery in the last 12 months on the involved side, reproduction of symptoms with active or passive cervical movements, neurological involvement with sensory and muscular deficit, Randomization and allocation concealment was performed to either study group or control group using block randomization, following informed consent and baseline assessment of participants.
Procedure
All participants had undergone a clinical examination process starting with a thorough history taking, followed by a physical examination of the cervical spine, the shoulder girdle, and the shoulder joints. All joints are manually assessed with passive, active, and combined angular movements, and with translatory tests according to the description of Maitland 16. Isometric resistance tests are used to judge shoulder strength and pain. Integrity of the rotator cuff is assessed with the external rotation lag sign 17, the lift off test 18, and the horn blowers' sign 19 involvement of the neural system with upper limb tension tests described by Butler 20. Contributing factors such as a slouched posture, forward head position, thoracic kyphosis, or protracted shoulders are noted and if necessary also assessed in detail. Both groups received therapeutic ultrasound, stabilization exercise and supraspinatus strengthening exercise (full can exercise, horizontal abduction). Therapeutic ultrasound a common physical treatment for tendon disorders. Ultrasound waves are transmitted from a transducer to a patient via a coupling Medium (such as a gel). Ultrasound has a thermal effect on tissues, causing local heating, although this may be attenuated by the use of a pulsed (intermittent) process. Despite the popularity of therapeutic ultrasound there is little clinical evidence demonstrating its efficacy 21-23 .Therapeutic ultrasound was administered in 1 MHZ for 10 minutes with an intensity of 0.8 W/cm2 with a total of 12 sessions, 4 times in a week for 3 weeks. Study group underwent DTMF in addition to the control group treatment procedure and was administered to the participants in sitting with the arms placed behind his or her back .In this position the tendon is bent through a right angle and exposed in the sagittal plane ( brings the tendon out from the acromion ). The Physical therapist finger?s directed to the lesion and transverse to the direction of the muscle fibers in circular movements with the tendon receveing the DTMF appropriately tensioned and the friction applied over the site of lesion, and the depth of friction was administered tolerable to the patient11, 12, and the treatment duration is about 15 minutes and given a total of 12 sessions with 4 sessions a week for about 3 weeks‘ time. Pain intensity was recorded in a 10 cm Visual Analog Scale (VAS) with 0 indicating no pain and 10 indicating more severe pain, and the active pain free shoulder Range of Motion (ROM) was assessed in a standard goniometer. A pretest measurement of pain Active pain free shoulder ROM was measured and documented before the commencement of the treatment and the participants was assessed at the end of twelve sessions of treatment and posttest measurement was documented for analysis.
Outcome measure
Selection criteria for the outcome measures used in this study were their reliability and validity in relation to the study population, the main focus is on pain and ROM. The primary outcome measure used in this study is Visual Analog Scale (VAS) and the secondary outcome measure is Active pain free Range of Motion (ROM).
Data Analysis
In this Randomized pilot trial the statistical method used to show the effectiveness of the study and the control group was dependent?t‘ test. And the combined standard deviations values of both groups was obtained and the independent?t‘ test is performed to show the effectiveness.
RESULTS
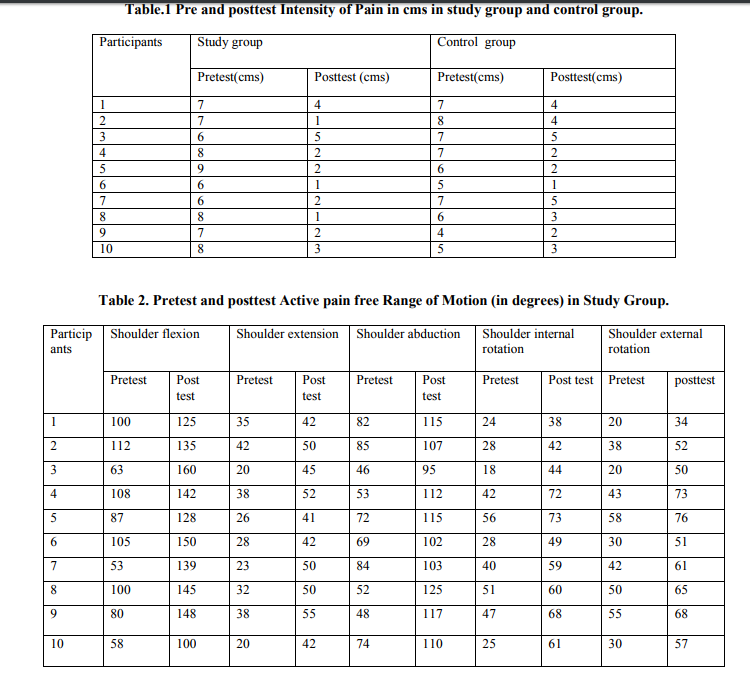
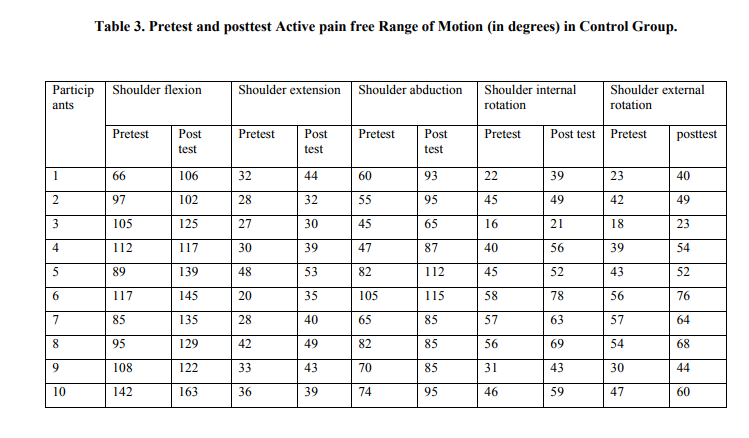
A total of 42 participants were visited our physical therapy department with shoulder pain out of which 20 participants were met the inclusion criteria( n=20) irrespective of gender and age they randomly allocated in to the study and control group .The pretest and posttest VAS in cms is shown in (Table 1). The dependent?t‘ value of study group is 8.9 and control group is 8.3 the obtained?t‘ value for both groups is compared with the two tailed table value with 9 degrees of freedom 2.26 while comparing it shows both the group decreases pain effectively, using the independent?t‘ test?t‘ value is 2.640 this ?t‘value is greater than one tail table value 2.10 with 18 degrees of freedom at p=0.05 respectively. This shows the treatment given in study group decreases pain effectively than the control group. The pretest and posttest Active pain free shoulder range of motion in degrees is shown in (Table 2) for study group and (Table 3) for control group. The shoulder ROM (flexion, extension, abduction, internal rotation, external rotation , were analyzed with dependent ?t‘value .The dependent ?t‘value in flexion, extension, abduction, internal rotation, external rotation in study group was 6.40,8.44,,7.3,8.0,9.5 and the control group was 2.36,6.3,5.7,6.4,8.0 respectively. The obtained ?t‘value for both the groups is compared with the two tailed table value with nine degrees of freedom 2.26 while comparing it shows the both the groups shows a significant increase in range of motion. Using the independent ?t‘ test the ?t‘ value is 2.37,4.08,2.87,3.02,3.27 in flexion ,extension ,abduction ,internal rotation and external rotation respectively ,the obtained ?t‘ values is greater than the one tail table value 2.10 with 18 degrees of freedom at p=0.05 respectively. Hence the treatments given in the study group increases shoulder Range of Motion effectively than the treatment given in the control group.
DISCUSSION
The results of this study indicated that both DTMF combined with therapeutic ultrasound and exercise showed significant improvements in pain severity, ROM measurements. Both groups showed improvements in pain severity, ROM measurements. Improvements in both groups may be due to additional application of therapeutic ultrasound and exercise program. Deborah Swan Downing and Arthur Weinstien24 in his double blind trial shown both Ultrasound and exercise can be considered to contain certain properties that might lead to an eventual reduction of pain and increase in range of motion. Exercise, however, possibly has such a profound beneficial effect that it masked any minor benefit from Ultrasound. But Ultrasound and exercise usually are prescribed together for the treatment of adhesive capsulitis, tendinitis, or bursitis of the shoulder and, thus, the above concern is more theoretical than practical. Nagrale et al 25 in his study demonstrated that Cyriax physiotherapy is superior to treatment approach compared to phonophoresis and exercise in management of lateral epicondyalgia, this study with the obtained independent ?t‘ test value demonstrates the DTMF combined with therapeutic ultrasound and exercise shown effectiveness than the therapeutic ultrasound and exercise, however the small population size ,small follow up duration a Randomized Pilot trial limits the study. Further studies with large samples, longer follow up durations were required to demonstrate its efficacy, frequency and duration.
CONCLUSION
Both groups showed a significant improvement in pain and Range of Motion, however study group showed detectable changes than the control group. Our results showed improvements on pain severity, and ROM of the patients with SST with the therapy program of DTMF, therapeutic ultrasound and exercise. Finally this study concludes DTMF are the valuable components in the comprehensive rehabilitation of participants with supraspinatus tendinitis of the shoulder joint.
References:
1. Bjelle A. Epidemiology of shoulder problems. Balliere’s Clinical Rheumatology 1989; 3:437–451.
2. Beaton D, Richards L. Measuring Function of the Shoulder. The Journal of Bone and Joint Surgery 1996; 78-A: 882–90.
3. Gartsman GM, Brinker MR, Khan M, Karahan M. Self-assessment of general health status in patients with five common shoulder conditions. Journal of Shoulder and Elbow Surgery 1998; 7(3):228–237
4. Rees J, Wamuo I, Jan W, Gibson T. Ultrasound evaluation of shoulder pain and restriction in the elderly. British Society for Rheumatology Annual Meeting, April 2004; 43(Suppl 2):ii73
5. Codman EA. The shoulder: rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. Boston, MA: Thomas Todd, 1934.
6. Rathbun JB, Macnab I. The micro vascular pattern of the rotator cuff. J Bone Joint Surg Br 1970; 52:540–53.
7. Ling SC, Chen CF, Wan RX. A study on the vascular supply of the supraspinatus tendon. Surg Radiol Anat 1990; 12:161–5.
8. Moseley, H.F. The vascular supply of the rotator cuff. Surgical Clinics of North America 1963; 43, 1521-1522
9. Rothman, R.H. and Parke, W.W. The vascular anatomy of the rotator cuff. Clinical Orthopaedics 1965; 41, 176-186.
10. J. D. Rees, A. M. Wilson and R. L. Wolman. Current concepts in the management of tendon disorders. Rheumatology 2006; 45:508–521.
11. Cyriax J. Diagnosis of soft tissue lesions. In: Cyriax J editor(s). Textbook of Orthopaedic Medicine. 9th Edition. Vol. 1, Baltimore: Williams and Wilkins, 1975.
12. Cyriax J. Treatment by manipulation, massage and injection. In: Cyriax J editor(s). Textbook of Orthopaedic Medicine. 9th Edition.Vol. 2, Baltimore: Williams and Wilkins, 1975.
13. Schwellnus MP, Mckintosh L, Mee J. Deep Transverse Frictions in the Treatment of Iliotibial Band Friction Syndrome in Athletes: A Clinical Trial. Physiotherapy 1992; 78(6):564–568.
14. Walker JM. Deep transverse frictions in ligament healing. JOSPT 1984; 6(2):89–94.
15. Brosseau L, Casimiro L, Milne S et al. Deep transverse friction massage for treating tendinitis. Cochrane Database Syst Rev 2002; 4: CD003528.
16. Maitland GD: Manipulation der Wirbelsäule. 2nd edition. Berlin: Springer Verlag; 1994.
17. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. Journal of Shoulder and Elbow Surgery 1996, 5:307-313.
18. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle. Clinical features in 16 cases. Journal of Bone and Joint Surgery 1991, 73B:389-394.
19. Walch G, Boulahia A, Calderone S, Robinson AHN: The 'dropping' and 'Hornblower‘s' signs in evaluation of rotatorcuff tears. Journal of Bone and Joint Surgery Br 1998, 80:624-628.
20. Butler DS: Mobilisation des Nervensystems. Berlin: Springer Verlag; 1995
21. Speed CA. Therapeutic ultrasound in soft tissue lesions. Rheumatology 2001; 40:1331–6.
22. Van der Windt DA, van der Heijden GJ, van der Berg SG, Ter Riet G, de Winter AF, Boulter LM. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain 1999; 81:257–71.
23. Robertson VJ, Baker KG. A review of therapeutic ultrasound effectiveness studies. Phys Ther 201; 81:1339–50.
24. Deborah Swan Downing and Arthur Weinstein. Ultrasound Therapy of Sub acromial Bursitis. A Double Blind Trial. Phys Ther Volume 66 / Number 2, February 1986 194-199.
25. Nagrale AV, Herd CR, Ramteke G. Cyriax Physiotherapy versus Phonophoresis with supervised exercise in subjects with lateral epicondyalgia. A Randomized controlled Trial. J Man Manip Ther 2009; 17(3):171-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





