IJCRR - 3(10), October, 2011
Pages: 99-105
Print Article
Download XML Download PDF
PROFILE OF FINE NEEDLE ASPIRATION CYTOLOGY OF HEAD AND NECK LESIONS IN A TERTIARY
HOSPITAL
Author: Lakshmibai B Mallappa, Ramya B S, B Latha, D C Prabhu
Category: Healthcare
Abstract:Background and objective :- Fine Needle aspiration cytology (FNAC) is a simple, minimally invasive screening test and is an essential component of pre-treatment investigation, on which clinical
management is based. Although surgical excision of palpable lesions in head and neck lesions is relatively
simple, vicinity to other anatomical structures in this region sometimes causes problems. Hence FNAC is
a useful diagnostic technique in the management of head and neck lesion. This study is done to evaluate
the role of FNAC in palpable head and neck masses and also to study their distribution.
Materials and methods :- Study includes 437 patients presenting with palpable head and neck lesions subjected to FNAC at the Department of Pathology, Victoria hospital BMCRIand RI, Bangalore
fromJanuary2011to March2011. The age ranged between1-95 yrs with Male to Female ratio of 1:1.57.
Out of these 199 cases (45.5%) were from cervical lymph nodes, 141(32.5%) from thyroid, 28
cases(6.4%) from salivary glands. Granulomatous Lymphadenitis was the commonest diagnosis followed
by nodular goitre of thyroid, Hashimotos thyroiditis, reactive hyperplasia, metastatic lymph nodes.Out of
these 43 cases (9.83%) malignant and 394 cases (90.16%) benign. FNAC was inconclusive in7.8% of
cases.
Conclusion:- The current study evalutes the role of FNAC as a diagnostic tool in the investigation of
head and neck lesions. Tuberculous Lymphadenitis still remains the most common lesion in the head and
neck region.
Keywords: Fine-Needle Aspiration Cytology, Lymph-Nodes, Thyroid, Salivary Glands.
Full Text:
INTRODUCTION
FNACis a rapid, convenient and accurate method of tissue diagnosis that can be done on an out-patient basis. FNAC offers a simple method of diagnosis of neoplastic and non – neoplastic lesions of the head and neck. The procedure is safe and free from complications and is well tolerated by the patients. There is no evidence that the tumor spreads through the skin tract created by the fine hypodermic needle used in this technique.1 The high degree of diagnostic accuracy, low costs and minimally disruptive nature of the procedure makes FNAC a highly desirable alternative to open biopsy.2 FNAC does not give the same architectural detail as histology but it can provide cells from the entire lesion as many passes through the lesion can be made while aspirating. All head and neck lesions must undergo FNAC and culture if necessary.3The tissues which are most frequently sampled are lymph-nodes, thyroid and major salivary glands.4
MATERIALS AND METHODS
A prospective study of 3 months duration, between January2011 to March 2011 was conducted in the Department of Pathology, Victoria Hospital, Bangalore. A total of 698 cases of FNAC were done out of which 437 cases were of head and neck region. Prior to FNAC, the patients were examined in detail, which included the recording of their pertinent clinical history and significant clinical findings. Relevant investigations were carried out as per requirements. FNAC was done using 22G needle fitted to a 10ml disposable syringe. Multiple needle passes, continuous aspiratory pressure and release of pressure before withdrawal from lesions was followed during aspiration. Smears were air-dried and stained by Giemsa Stain. The rest of the slides were fixed in methanol and stained by Hand E procedure. The Zeihl Neelsen‘ stain for AFB was done in those cases with Lymph-node swellings where the clinical suspicions or diagnosis was tuberculosis and/ or in those cases where purulent or cheesy material was aspirated. A cell-block preparation was also done where the aspirated material was adequate. Ultra-sound Guided FNACs were very few .
RESULTS
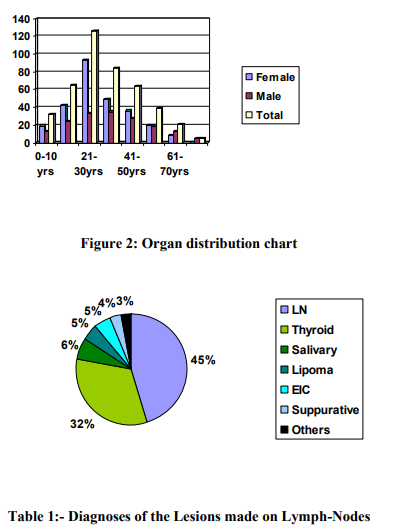
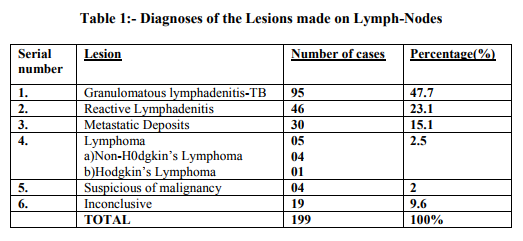
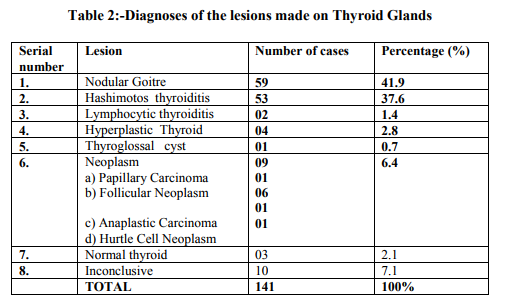
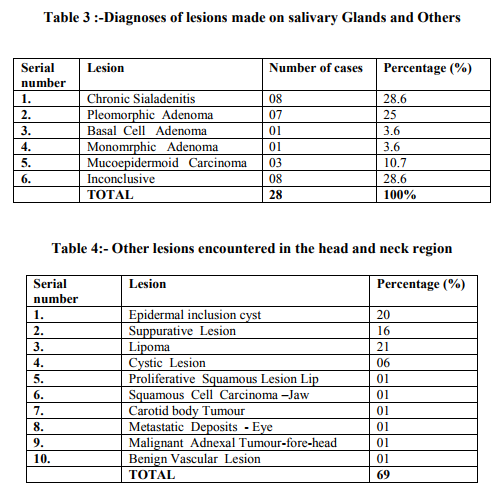
In this prospective study of 437 cases, adequacy of material was achieved is 92.2%.The age ranged between 1-95 yrs. The lesions were most commonly seen in the age group of 21- 30yrs.The number of male patients were 170(39%) and female patients were 267(61%). The male to female ratio was 1:1.57(Figure 1). Lymph-nodes constituted the most common organ with 199 cases(45.5%),followed by Thyroid 141cases(32.5%),Salivary Glands-28 cases(6.4%) and others 69 cases(15.9%).Among these cases 43 cases(9.83%) were malignant and 394 cases(90.16%) were benign(Figure 2). In the lymph node granulomatous lymphadenitis was the most common lesion accounting for 95(47.7%) cases followed by reactive lymphadenitis in 46 cases and metastatic lymph node deposits in 30 cases (Table 1). A total of 141 cases of thyroid FNAC were done among which nodular goitre was the most common diagnosis(41.9%) followed by Hashimotos thyroiditis (Table 2). In the salivary gland chronic sialadenitis was the commonest with 8 cases followed by pleomorphic adenoma in 7 cases. The other common lesions encountered during FNAC of head and neck region includes mainly epidermal inclusion cysts 20 cases, lipoma 21 cases, suppurative lesions 16 cases, benign cystic lesions 6 cases and single cases of proliferative squamous lesion lip, Squamous Cell Carcinoma of Jaw, Carotid body tumour, Metastatic deposits in the Eye, Malignant adnexal tumour over forehead and Benign vascular lesion (Table 4).
DISCUSSION
Diagnostic cytology when performed by well trained experienced individual offers high degree of reliability and feasibility, therefore FNAC has gained universal acceptance as in most instances it is inexpensive, safe, quick and accurate.2 Head and Neck masses often pose a challenging diagnostic problem to the clinician.4 The goal of FNAC in the head and neck area as in other anatomical sites is to provide clinically useful information which exceeds that obtained by palpation or imaging alone. The false negatives and false positives were pointers towards problems and pitfalls in cytological interpretation.6 This prospective study was evaluated and the results were compared with other reports.
S.Soni etal1 Studied 59 cases and found 47.45% were of neck nodes, 23.72% were of thyroid, 22.03% were of salivary glands and 6.77% were of other lesions. Farzana Shahid et al2 have studied 518 FNAC from head and neck lesions, out of which 473 were benign and 45 cases were malignant. Maximum number of cases were from Lymphnodes (356), followed by Thyroid (124) and Salivary gland (38). The above 2 studies are almost similar to our analysis. In our study 43(9.83%) cases were malignant and 394 cases (90.16%) were benign. The frequency of the various lesions in the different organs were as follows Lymph-Nodes - 199cases(45.5%), Thyroid-141cases(32.5%), Salivary Gland-28 cases(6.4%) and others 69 cases(15.9%). Fernandes H et al4 found that the most common site aspirated was Thyroid Gland (71.3%) followed by Lymph-Nodes(22.48%),Salivary gland (3.87%) and soft tissue lesions(2.32%). Naila Tariq et al6 analysed 122 FNACs of Head and Neck lesions, among which 65 cases were from thyroid,53 cases from lymph-nodes and 4 cases from salivary gland. In our study of lymph-nodes, the spectrum of lesions include granulomatous Lymphadenitis constituting (48%), followed by reactive lymphadenitis which is 23.2%. Metastatic Deposits about 15.1%.Primary malignancies such as Hodgkin‘sLymphoma and NonHodgkin‘s Lymphoma constituted about 2.5%.About 2% of cases were suspicious of malignancy. About 19cases(9.6%) were inconclusive for interpretations. The study conducted by Farzana Shahid etal2 ,showed almost similar results with Granulomatous Inflammations being most common lesion constituting which 238cases(66.9%) followed by reactive hyperplasia 54 cases(15.2%) and that of primary malignancy were2.8%. Another study conducted by Tariq Ahmed et al3 on 50 patients found Tuberculous Lymphadenitis to be the commonest(36%), followed by reactive Lymphadenitis(18%).Other malignant lesions constituted(14%). About 8% of cases were inconclusive. In our study of Paediatric lymph-node FNAC, the ratio of Tubercular Lymphadenitis to that of Reactive Lymphadenitis is almost1:2. This ratio indicates that lymphoid hyperplasias are more common in this age group.This analysis has also been done by Amy Rapkiewicz et al5 where in they had 36 cases of reactive lymphoid hyperplasia to 3 cases of Tubercular Lymphadenitis. Fernandes H et al4 found reactive Lymphadenopathy was the commonest cause of lymphadenopathy followed by Tuberculosis and Granulomatous, Metastatic Lymphadenopathy. The study conducted by Muhammad Javaid et al7 showed that malignant Lymphadenopathy constitutes a significant portion of findings in aspirates of enlarged lymph nodes(57.15%).The benign lymphadenopathy only constitutes 42.85% of which tuberculous lymphadenitis was the commonest finding(26.19%) followed by reactive hyperplasia(16.66%). The diagnostic accuracy of material in our study was 92.2%.This valve is similar to that of Andleeb Abrari et al8 , where it is 93.3%. With regards to thyroid lesions our study showed that Nodular Goitre(41.9%) was the commonest followed by Inflammatory lesions such as Hashimotos‘s Thyroiditis- 37.6%,Hyperplastic Thyroid-2.8%, Lymphocytic Thyroiditis 1.4%.The neoplastic lesions constituted about 6.4%.3 cases of normal thyroid and in 10 cases(7%) the aspirates were inconclusive. The above figures are similar to that of Farzana Shahid et al2 where in their commonest lesion was Benign Nodular Goitre(52.4%);Inflammatory lesions(7.4%) and Neoplastic were 3.2%.Another study conducted by Fernandes H et al4 found that Thyroid Gland(71.31%) was the commonest site aspirated in the head and neck region.Even in their study the commonest lesion encountered in the Thyroid Gland was Nodular Goitre, followed by Hashimotos Thyroiditis and Papillary Carcinoma was the commonest malignant lesion.1 case of Thyroglossal Cyst was diagnosed. Even in our study there was 1 case of Thyroglossal Cyst. The study conducted by Naila Tariq et al6 Showed 37 cases of Multinodular Goitre(56.9%);followed by inflammatory and neoplastic lesions. A study conducted in a tertiary health care centre by G.G. Swamy et al10 also revealed that the most common organ aspirated was the Thyroid Gland(60%) with 52% Nodular Goitre followed by 16% of follicular neoplasm;12% as papillary carcinoma and 4% cases as suspicious of malignancy Finally with regards to salivary glands in our study there were 28 cases(6.4%).The commonest lesion being inflammatory-Chronic Sialadenitis- 8cases(28.6%), 9cases(32.2%) benign neoplasms and 3 cases of (10.7%) mucoepidermoid carcinoma and 8 cases were inconclusive(28.6%). A study by G.G Swamy et al9 showed out of 20 cases-8cases(40%) were benign neoplasms,3 cases(15%) were malignant neoplasms, 1 case(5%) was non-neoplastic and 8cases(40%) were inflammatory lesions. Another study by El Hag et al10 also showed that inflammatory lesions such as sialadenitis was most commonest with 12cases(57%) followed by benign lesions 8 cases(38%) and mucoepidermoid carcinoma 1 case(5%). The remaining other lesions were Epidermal Inclusion Cyst 20 cases(4.6%), suppurative lesions 16 cases(3.7%), Lipoma 21 cases(4.8%) ,Cystic Lesion 6 cases(1.4%),proliferative squamous lesion lip -1 case, squamous cellcarcinoma –jaw -1 case, carotid body tumour -1 case, metastatic deposits eye-1case ,malignant adnexal tumour –fore head -1 case and benign vascular lesion 1 case. The high rate of inconclusive samples can be explained by some factors that have been described previously in the literature. These are as follows
- Inexperience in the collection of cells
- difficulty in interpreting the smears
. - poor or inadequate smears for interpretation
. - artifacts, such as necrosis and high content of blood in some samples.11
On comparing the results of the present series with other workers, it can be said that the results of this study are favourable with those published in literature and are fairly accurate.
CONCLUSION
FNAC is a simple and rapid procedure which can be carried out as an out-patient procedure with minimal problems. Owing to its accurate diagnostic potential it is proved useful in separating inflammatory, benign and malignant lesions with good certainty. Morever, the procedure is simple and cost-effective. Hence, FNAC is recommended as the first-line investigation in diagnosing head and neck lesions. In a developing country like India even today Tuberculosis Lymphadenitis remains the most common lesion,
References:
1. S,Soni, S.KPippal,YashveerB,P Srivastava: Efficacy of Fine Needle Aspiration Cytology inDiagnosis of Neck Masses. www.waent.org/archeives/2010/Vol3-2; pg1-5
2. Farzana Shahid, Talat Mirza,Shahid Mustafa,,Saima Sabahat andShaheen Sharafat;An Experimental Status of Fine Needle Aspiration Cytology of Head and Neck Lesions in aTertiary Care Scenario.- International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 10 October 2011 103 Journal of Basic and Applied Sciences vol.6,No2,159-162,2010.
3. Tariq Ahmad, Mohammad Naeem, Siddique Ahmad, Ambreen Samad, Amir Nasir-Fine Needle Aspiration Cytology(FNAC) and swellings in the surgical out-patient.-J .Ayub Med ical College Abbottabad 2008;20(3):30-32.
4. Fernandes H, D‘Souza C.R.S., Thejaswini B .N-Role of Fine Needle Aspiration Cytology in palpable Head and Neck Masses. Journal of Clinical and Diagnostic Research.2009; Oct(3):1719-1725.
5. Amy Rapkiewicz et al-Spectrum of Head and Neck Lesions Diagnosed by Fine – Needle Aspiration. Cytoiogy inthe Pediatric Population. Cancer CytoPathology 2007;111:242- 51@2007American Cancer Society.
6. Naila Tariq,Saleem Sadiq,Shahnaz Kehar,Muhammad Shafiq. Fine Needle Aspiration Cytology of Head and Neck Lesions-An Experience at the Jinnah Postgraduate Medical Centre,Karachi. Pakistan Journal of Otolaryngology 2007;23:63-65
7. Muhammad Javaid, Niamatullah, Khurshid Anwar, Muhammad Said-Diagnostic valve of Fine Needle Aspiration Cytology (FNAC) in Cervical LymphadenopathyJPMI 2006 Vol.20No.2:117-120
8. Andleed Abrari,S .Shamshad Ahmad, Vandana Bakshi.-Cytology in the otorhinolaryngologist‘s domain-A study of 150 cases,emphasizing diagnostic utility and pitfalls-Indian Journal of Otolaryngology and Head and Neck Surgery Vol.54No.2,April-June2002
9. G.G. Swamy,A.Singh,J.M Ahuja, N.Satyanarayana.-Accuracy of fine needle aspiration cytology in the diagnosis of palpable head and neck masses in a tertiary health care center.-Journal of College of Medical Sciences-Nepal,,2010.Vol-6,No- 4,19-25.
10. Imad Abdien El Hag et al-Fine Needle Aspiration Cytology of Head and Neck Masses-Seven years Experience in a Secondary Care Hospital-Acta Cytologica 2003;47:387-392.
11. Ana Paula Candido dos Santos et al-Fine Needle aspiration biopsy in the oral cavity and head and neck regionBrazOralRes.2011Marc-April;25(2):186- 91.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





