IJCRR - 8(16), August, 2016
Pages: 14-20
Date of Publication: 22-Aug-2016
Print Article
Download XML Download PDF
A STUDY OF SHORT-TERM OUTCOME OF ACUTE CORONARY SYNDROME PATIENTS WITH SPECIAL REFERENCE TO SERUM URIC ACID AT PRESENTATION
Author: Kapildev Mondal, Soumabrota Dutta
Category: Healthcare
Abstract:Background: Acute coronary syndrome is very common course of death worldwide. It is the most common life Threatening cardiological disease. Assessment of prognosis of acute coronary syndrome patient with respect of Uric acid level as a risk factor to prevent mortality and morbidity have great impact on public health.
Aim of the study: Very few Literatures are available regarding this. Our objective is to find out the Effect of Serum Uric acid level on short term outcome of acute coronary syndrome patient.
Materials and Methods: We did retrospective study in general medicine department of SSKM HOSPITAL; Kolkata, with acute coronary syndrome patients on 2009-2010.
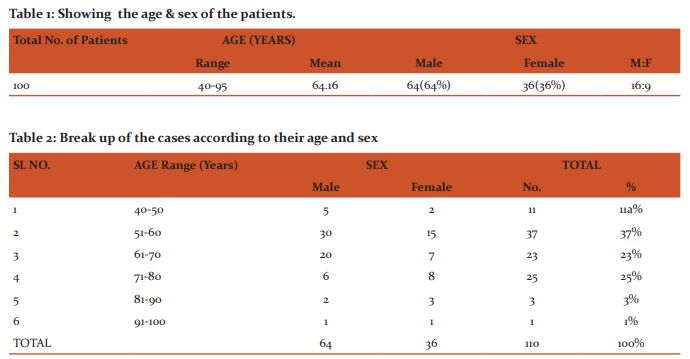
Our study included 100 patients of acute coronary syndrome of various severity. We also proposed to do a detailed laboratory investigation including serum uric acid level in every patient. We did Detailed Clinical Examination and Relevant laboratory investigation. We collected Data according to Hospital regulation after approval by Hospital authorities. Then we analyzed data with help of statistical method BY using software.
Results: In our study serum uric acid levels correlate with severity of cardiac failure. There was statistically significant correlation found between serum uric had higher levels of uric acid as compared to patients of class l and ll.
Discussion: Out of 100 patients, six expired during 7 day follow up. Patients who had myocardial infarction in past have higher serum uric acid levels and are in higher Killip class. Combination of Killip class and serum uric acid level after acute myocardial infarction is a good predictor of mortality after ami.
Conclusion: Hyperurecemia is found to be associated with less chance of good outcome of acute coronary syndrome patients.
Keywords: Hyperurecemia, Investigation, Arthritis
Full Text:
INTRODUCTION
Acute coronary syndrome (ACS) is usually one of three diseases involving the coronary arteries-ST elevation myocardial infarction (30%), Non ST elevation myocardial infarction (25%) and Unstable angina (38%). ACS should be distinguished from stable angina, which develops during exertion and resolves at rest. In contrast with stable angina, unstable angina occurs suddenly, often at rest or with minimal exertion, or at lesser degrees of exertion than the individual’s previous angina (“crescendo angina”). New onset angina is also considered unstable angina, since it suggests a new problem in a coronary artery. Diabetes (with or without insulin resistance)is the single most important risk factor for ischaemic heart disease (IHD). others risk factors are tobacco smoking, hypercholesterolemia, low HDL, high triglycerides, high blood pressure, family history of ischaemic heart disease (IHD),obesity (defined by a body mass index of more than 30 kg/m²), age (men acquire an independent risk factor at age 45, Women acquire an independent risk factor at age 55)stress, prolong intake of alcohol. There are ongoing research in the field of emerging risk factors and factors determining ultimate outcome. Epidemiological studies shows direct relationship between the levels of the natural antioxidant uric acid and the risk of coronary ischaemic events Assuming the importance of oxidative stress in patients with brain ischaemia and the antioxidant property of uric acid, in our study this relationship is evaluated in 100 patients of acute coronary syndrome. Aims of the study: Evaluation of A.C.S. patients clinically, evaluation of serum uric acid for all these patients at presentation and assessment of coexisting risk factors making regular check up of all these till discharge or death. Objectives: To find out effect of serum uric acid level on Short term outcome of Acute Coronary syndrome patient. Materials and Methods: We conducted the study in the Department of Medicine and cardiology department I.P.G.M.E.and R and SSKM Hospital during 2009-2010. Selection Criteria: we ,selected ACS patients presenting within 72hrs of onset, excluded Patients of below 40 yrs ,Patients suffering from other co-morbid conditions which itself may be the determining factor of outcome of patients, any patient with a condition known to elevate uric acid level and Any acute coronary syndrome secondary to ventricular aneurism and vasculitis .
METHODS
We included 100 patients of ACS of various severity (Any patient who were diagnosed as ST segment elevated acute myocardial infarction (STEMI) or non-ST segment elevated acute myocardial infarction (NSTEMI) on the basis of clinical history, examination, ECG changes, biochemical markers, and admitted in Cardiology and Medicine ward of S.S.K.M Hospital, Kolkata)(severity is assessed with killip scale both on admission and on discharge). We put the result of the study in tables and performed statistical analysis with the help of SYSTAT statistlcal software.
COUNCELLING: We explained the nature of study to each patient and patient's fellow and took informed consent.
PROCEDURES: A through history and clinical evaluation has done a in each patient and also imaging studies and biochemical test conducted meticulously special reference to Killip class.
STUDY TECHNIQUE: The presentstudy is a restrospective, observational epidemiological study We took history and did proper clinical examination. Patients were treated as decided by attending physician. Patients were followed up till hospital stay i.e. 7 days. Serum uric acid level was measured on day 0, 3 and 7 day of MI.
RESULTS
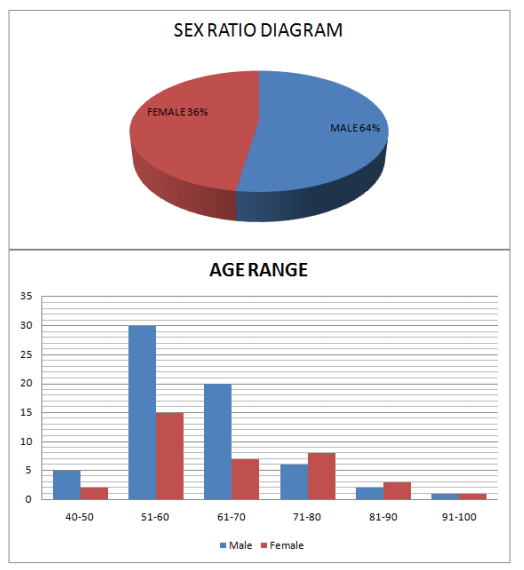
100 patients of ischaemic stroke presenting within 72 hours, of either sex were studied in Medicine and cardiology indoor, I.P. G.M.E and R Kolkata. We excluded patients of age below 40 and patients suffering from other co-morbid conditions which itself may be the determining factor of outcome, e.g., cerebral stroke, hepatic encephalopathy, renal failure. Elaborate clinical examination and laboratory investigations were done in every patients to evaluate relevant confounding factors and outcome Predictors. Outcome in ischaemic ACS patients greatly varies, from complete recovery to death. So, researchers at different time tried to evaluate the outcome of ACS. There are observed data where we found beneficial effects of serum uric acid (5,6)and in some deleterious effects (7) is documented in outcome of ACS. Therefore we examined the effect of serum uric acid on outcome of ACS stroke patients. Acute coronary syndrome(ACS) was measured on admission and discharge by killip scale done with the help of SYSTAT software. General Least square Method with two dependent variables and single dependent variable were used to analysis relevant confounder and potential predictors such as Age, Sex, ACS Severity on admission, Diabetes, Hypertension, Atrial Fibrillation, Sodium and Potassium, Smoking, Previous History of AMI, FBS- Urea and Creatinine. In statistical analysis, we found significant effects of Age, sex, Stroke Severity on admission, Diabetes, Hypertension, Atrial Fibrillation, lschaemic Heart Disease, Smoking, Previous History of Stroke, FBS, Urea and creatinine in outcome of stroke in our study, as found in other studies (13,32,35) also. Hyperuricaemia is found to be associated with less chance of good outcome. This finding is corroborating with other studies (6 ,1,9).
DISCUSSION
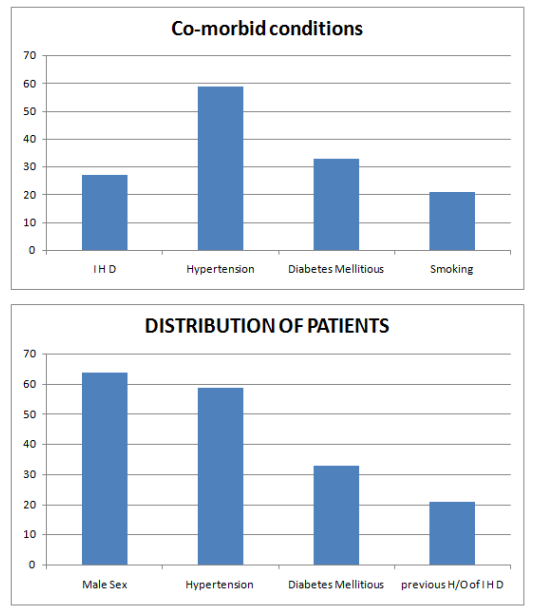
We, used the study as referral study, we © JAPI • VOL. 56 • OCTOBER 2008 www.japi.org 761 tried to find correlation between serum uric acid and Killip class and their prognostic value in our patients. Present study was conducted in 100 patients of acute Coronary syndrome, who presented to hospital with in 24 hrs of onset of symptoms. Out of 100 patients, 65 had ST-elevation myocardial infarction (STEMI), while 35 patients were of non-ST elevation myocardial infarction (NSTEMI).
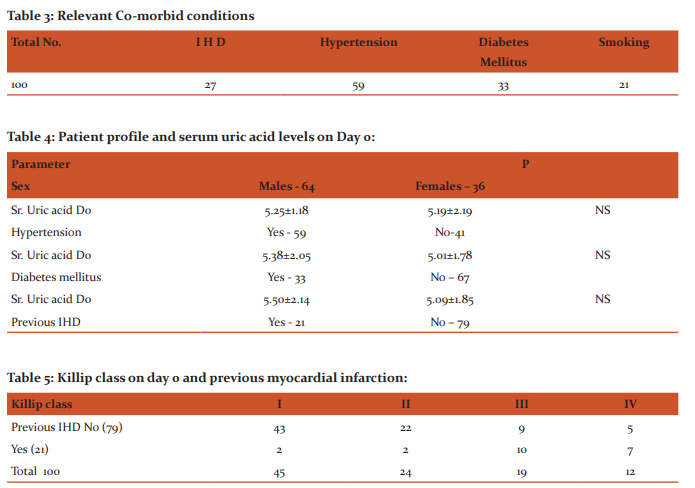
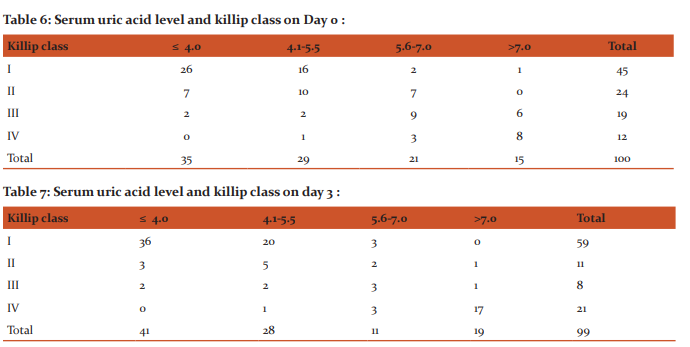
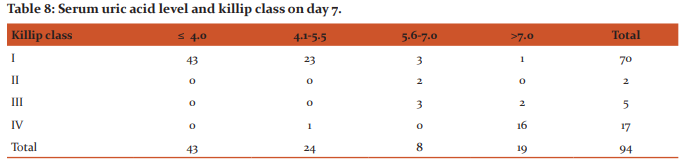
Sixty one patients were thrombolysed while four were not thrombolysed due to delayed presentation. Uric acid was treated as a continuous variable and as a categorical variable, and variables were divided into quartiles according to serum uric acid concentrations same as in referral study by Kojima et al. There was no significant correlation (p=0.396) between serum uric acid level and patients who were known or found to be hypertensive on admission (Table 2). This is different than other studies which showed that hypertensive patients had more hyperuricaemia. Thirty three percent patients were known diabetic in our study. Non-diabetic and diabetic patients had comparable serum uric acid levels on Day0 (Table 2). This finding is consistent with study by Tuomilheto et al in which there was no significant association between serum uric acid level and diabetic status. In our study patients with hyperuricaemia is significantly associated with type 2 diabetes mellitus. Twenty one percent patients had history of ischemic heart disease. There was significant difference between serum uric acid concentration at the time of admission and h/o ischemic heart disease (Table 2). Also, Patients who were known case of IHD were in higher Killip class (Table 3). There was a correlation between serum uric acid level and Killip class on day of admission (Table 4). patients of Killip class lll and lV In our study serum uric acid levels correlate with severity of cardiac failure (Tables 4, 5 and 6). There was statistically significant correlation found between serum uric had higher levels of uric acid as compared to patients of class l and ll. This finding is consistent with referral study.9 .There is statistically significant association (p=<0.05) between serum creatinine on day of admission and Killip class, in our study. Out of 100 patients, six expired during 7 day follow up. All the patients who died had serum uric acid level more than 7.0 mg/dL. Of these six patients, one was in Killip class, one in Killip class III and four were in Killip class IV at the time of admission. Thus, 83% of patient who died were in higher class i.e. class III and IV at time of admission. Two patients (one each) of Killip class I and III shifted to Killip class IV on day 3. One patient expired on day 3 was in Killip class IV on day 0. Rest five patients were in Killip class IV on day 3, who died later. Out of these six patients five had serum uric acid level in quartile 4 on day 0. Only one patient who was in Killip class I and had uric acid in 1st quartile; however his uric acid Uric acid raised to quartile 4 with shift of Killip class to class lV on day 3. On day 3 all five patients were in Killip class lV and had uric acid level in 4th quartile. Thus, all six pts who expired were in Killip class lV and had uric acid level in 4th quartile. Therefore it shows that serum uric acid concentration is significantly correlated with Killip class.
CONCLUSION
Rum uric acid levels are higher in patients of acute myocardial infarction as compared to normal healthy persons. Serum uric levels are correlated with Killip class; patients in higher Killip class have higher serum uric acid levels. Serum uric acid levels and Killip class are influenced significantly by previous myocardial infarction. Patients who had myocardial infarction in past have higher serum uric acid levels and are in higher Killip class. Combination of Killip class and serum uric acid level after acute myocardial infarction is a good predictor of mortality after AMI.
ACKNOWLEDGEMENT
To medical superintendent cum vice principal of S.S.K.M HOSPITAL and I.P.G.M.E and R, editor of different journal and text book from where I have taken references.
Source of funding: I expand from my personal account.
Abbreaviation ACS Acute coronary syndrome AMI Acute myocardial infraction A. Pn Aspiration pneumonia ADM Admission AF Atrial fibrillation CR Creatinine COPD Chronic obstructive pulmonary disease CHD Coronary heart disease D Discharge FBS Fasting blood sugar HTN Hypertension HT Hypothyroid IHD Ischaemic heart disease K Potassium ML Multiple lesion Na Sodium P/H/O Stroke Past history of stroke RHD Rheumatic heart disease RTI Respiratory tract infection SEP Septicaemia SL Single lesion SSS Scandinavian Stroke Scale Trop t troponin t Trop I Troponin I UA Uric acid U An Unstable angina U Urea
References:
1. Alderman M, Aiyer KJ. Uric acid: role in cardiovascular disease and effects of losartan. Curr Med Res Opin 2004;20:369-79.
2. Kroll K, Bukowski TR, Schwartz LM, Knoepfler D, Bassingthwaighte JB. Capillary endothelial transport of uric acid in guinea pig heart. Am J Physiol 1992, 262:H420-31.
3. Castelli P, Condemi AM, Brambillasca C, et al. Improvement of cardiac function by allopurinol in patients undergoing cardiac surgery. J Cardiovasc Pharmacol 1995;25:119–25.
4. Kogure K, Ishizaki M, Nemoto M, et al. Evaluation of serum uric acid changes in different forms of hepatic vascular inflow occlusion in human liver surgeries. Life Sci 1999;64:305–13.
5. Anker SD, Doehner W, Rauchhaus M, et al. Uric acid and survival in chronic heart failure: validation and application in metabolic, functional, and haemodynamic staging. Circulation 2003;22:1991–97.
6. Ochiai ME, Barretto AC, Oliveira MT, et al. Uric acid renal excretion and renal in sufficiency in decompensated severe heart failure. Eur J Heart Fail 2005;7:468–74.
7. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005;21:1685–95.
8. Fest a A, Haffner SM. Inflammat ion and cardiovascular disease in patients with diabetes: lessons from the Diabetes Control and Complications Trial . Circulation 2005; 11 :2414–15.
9. Kojima S, Sakamoto T, Ishihara M, et al. Prognostic usefulness of serum uric acid after acute myocardial infarction (Japanese Acute coronary Syndrome Study) . AmJ Cardiol 2005 ; 96 :489-95.
10. Bickel C, Rupprecht HJ, Blankenberg S, et al. Serum uric acid as an independent predictor of mortality in patients with angiographically proven coronary artery disease. Am J Cardiol 2002;89:12-7.
11. Johnson RJ, Rodriguez-Iturbe B, Kang DH, et al. A unifying pathway foressential hypertension. Am J Hypertens 2005;18:431-40.
12. Tuomilheto J, Zimmet P, Evawolf. Plasma Uric acid level and its association with Diabetes Mellitus and some Biologic Parameters in a Biracial Population of FIJI Am J Epidemiol 1988;127:32136.
13. Safi AJ, Mahmood R, Khan MA, Haq A. Association of serum Uric Acid with type II diabetes mellitus. J Postgrad Med Inst 2004;18:59-63.
14. Cicoira M, Zanolla L, Rossi A, et al. Elevated Serum Uric acid levels are associated with diastolic dysfunction in patients with dilated cardiomyopathy . Am Heart J 2002;143:1107-11.
15. Olexa P, Olexova M, Gonsorcik J, et al. Uric acid a marker for systemic inflammatory response in patients with congestive heart failure? Wien KIin Wochenschr 2002;28:211–15.
16. Harison’s Internal medicine 17th edition(Chapter 220,221,238,239).
17. Braunwald’s Heart Disease 8th edition(Chapter 50,51). 18. Davidson’s principle and practice of medicine 21th edition (chapter 18).
19. Hare JM, Johnson RJ. Uric acid predicts clinical outcomes in heart failure: insights regarding the role of xanthine oxidase and uric acid in disease pathophysiology. Circulation 2003;107: 1951-3.
20. Mercuro G, Vitale C, Cerquetani E, et al. Effect of hyperuricemia upon endothelial function in patients at increased cardiovascular risk. Am J Cardiol 2004;94:932-5.
21. War d HJ . Uric acid as an independent risk factor in the treatment of hypertension. Lancet 1998;352:670-1.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





