IJCRR - 3(11), November, 2011
Pages: 170-178
Print Article
Download XML Download PDF
CLINICAL EFFICACY OF A UNANI HERBAL FORMULATION OF HEMIDESMUS INDICUS AND
OINTMENT OF ASTRAGALUS HAMOSUS IN ENDOCERVICITIS-A RANDOMIZED SINGLE BLIND
STANDARD CONTROLLED TRIAL.
Author: Shahida Habib, Wajeeha Begum, Ismath Shameem, Gh Sofi, Azad Hussain Lone, Alia Bilal
Category: Healthcare
Abstract:Objectives: To compare the efficacy and safety of Hemidesmus indicus and ointment of Astragalus hamosus with Tablet Doxycycline and vaginal pessary of Clindamycin and
Clotrimazole in endocervicitis. Material and Methods: A randomized standard controlled single blind study was carried out in the Department of Gynecology at the National Institute of
Unani Medicine. Clinically diagnosed patients (n=45) were randomized to the test (n=30) and
control (n=15) Groups by computer generated random table No. The inclusion criteria were
married patients aged 18 to 40 years with symptoms of vaginal discharge, lower abdominal
pain, low backache, dysuria, dyspareunia, pruritus vulvae and post coital bleeding. The
exclusion criteria were unmarried, pregnant or lactating women, patients with pelvic pathology
or malignancy, using oral or intrauterine contraceptive devices, sexually transmitted diseases
and concomitant diseases. In the test Group, Majoon Ushba was given 10 gm BD orally and
intra-vaginally Marham Nakhuna was applied once daily at night for 15 days after menses for 3
consecutive cycles. In control group, Tablet Doxycycline 100 mg BD was given orally and
vaginal pessary of Clindamycin and Clotrimazole OD at night after menses for 7 days for 3
consecutive cycles. The results were analyzed by Kruskal-Wallis with Dunn's multiple
comparison, Wilcoxan match pair, Mann Whitney test, Student?t' test, Fisher's exact test and
Chi-square test. Results: There was a significant improvement in the subjective and objective parameters in both test and control group. The test drugs were found to show more response
than the control in the management of endocervicitis with p value< 0.05 Conclusion: The test
drugs were found to be useful and effective in the management of endocervicitis. Further, the
effectiveness should be evaluated in large sample size with recent techniques.
Keywords: Endocervicitis; sexually transmitted disease; Hemidesmus indicus; Astragalus hamosus; Unani Herbal formulation.
Full Text:
INTRODUCTION
Gynecological disorders can have a substantial impact on many aspects of quality of life, including reproductive ability, sexual functioning, mental health and the ability to work and perform routine physical activities.1-3 Endocervicitis is defined as inflammation of the columnar epithelium of the endocervix or inflammatory process in cervical epithelium and stroma or infection of the endocervix including stroma and glands.4-7 Clinically presence of yellow or green purulent exudates, more than 10 white blood cells per high power field (hpf) on cervical gram staining, ectopy of cervix with erythema, edema and friability.8, 9 Chronic inflammation of the endocervix is very common and is seen in about 35-85% of women. It is usually a histological diagnosis. It is found in nearly all multiparous and nulliparous, cervices.7, 10 Acute endocervicitis occurs after trauma due to parturition or abortion, inappropriate use of tampons or infection by pathogenic agents like streptococcus, staphylococcus, E. coli, Neisseria gonorrhoea, Chlamydia trachomatis. 10-12 Approximately, one-third of all women with vaginal discharge have endocervicitis. The Centre for Disease Control (CDC) and prevention estimates that over 19 million STIs occur annually, almost half of them among aged 15-24 years. The etiology of infective endocervicitis is variable and consists commonly of STIs.5, 9,13 In Unani system of medicine, the concept of humoral theory was first proposed by Hippocrates in 460 BC. He stated that if akhlat arba (morbid humours) are in a state of equilibrium, both qualitatively and quantitatively health is restored. Any derangement in these humours either qualitatively or quantitatively leads to disease.14 According to the Humoral theory, it is dam (blood), safra (bile) or occasionally sauda (black bile) or balgham (black bile) which are involved and dominant in warme ghishae unqur rehm (endocervicitis). Hence the abnormal accumulation of morbid humours causes sues Mizaj (deranged temperament) of uterus leading to endocervicitis. The therapeutic options for endocervicitis in conventional medicine include antiseptics, antibiotics, ablation by cryosurgery, electro diathermy, Co2 laser, cold coagulation and surgical interventions like trachelorrhapy,
cone biopsy, trachelectomy and hysterectomy.15 The surgical procedures cannot be availed by the poor sections of population. Looking at the side effects of conventional therapy and complications of surgical procedures, it is need of the hour to switch to an alternative system of medicine that is safe, cost effective, nonsurgical and can be easily availed by everyone with long lasting effects. Though the treatment of this disease dates back to ancient period, but validation and documentation are extremely deficient. Keeping the above facts in view, the present study was undertaken to evaluate the efficacy and safety of the Unani drugs in the management of Warme ghishae unqur rehm and to compare the results of Unani herbal drugs with standard drugs in controlled manner.
MATERIAL AND METHODS
Design: A prospective, single center, randomized standard controlled, single blind, pre and post evaluation study was conducted in the Outpatient department of Amraze Niswan (Gynecology) at the National Institute of Unani Medicine, during the year 2010-2011. This study was started after the approval from institutional ethical committee. The intervention was given for 3 consecutive cycles.
Participants: A total number of 98 patients were screened for endocervicitis during the study period. Fifty five patients were subjected to preliminary investigations and out of them ten patients were excluded (4 PCOS, 2 Pregnant, 1 DM, 2 Ovarian cysts, 1 Fibroid). The written consent was obtained from the patients, who fulfilled the inclusion criteria. They were evaluated through the complete history and physical examination. The inclusion criteria were married women aged 18 to 40 years with symptoms like white discharge, low backache, low abdominal discomfort, dyspareunia, postcoital bleeding, vulval itching, and dysmenorrhoea. The exclusion criteria were unmarried, pregnant or lactating women, patients with pelvic pathology and carcinoma, using oral or intrauterine contraceptive devices, with any concomitant diseases like hypertension, diabetes mellitus, and sexually transmitted diseases.
The pelvic examination was performed to evaluate the endocervicitis-related signs like vaginal discharge, bleed on touch, and to note the state of cervix, its position, direction, consistency, irregularity, or any other abnormalities. The subjective parameters like WDPV, LBA, LAP, pruritus vulvae and dysuria and the objective parameters like hypertrophy and congestion of cervix were assessed by grading system 15,16. Similarly, dyspareunia, post coital bleeding and foul smell, nabothian follicles and bleeds on touch were assessed by the presence or absence.15, 16 .
Investigations: The baseline clinical laboratory investigations such as haemoglobin percentage, total leucocytes count, differential leucocytes count, erythrocyte sedimentation rate, VDRL and Random blood sugar were done to exclude general diseases. Ultrasonography, and Papinicoulaou smear were done to exclude the pelvic pathology and malignancy. Cervical swab and culture for culture and sensitivity was done to see the organism involved. To assess the safety of drugs, blood urea, serum creatinine, SGOT, SGPT, and Alkaline phosphatase were done before and after trial. At every follow up of 15 days during three months of study period, progression or regression of symptoms and signs were recorded in the case record form.
Intervention: The patients were randomly allocated to the test (n=30) and control Groups (n=15) by computer generated table No. In the test Group, 10 gm BD Majoon Ushba was given orally and intra-vaginally ointment of Nakhuna was applied once daily at night for 15 days after menses (3 consecutive cycles). The control Group received orally, Tab Doxycycline 100gm BD and locally, vaginal pessary of Clindamycin and Clotrimazole per vaginum for 7 days after menses (3 consecutive cycles).17
Outcome: The outcome measures were to assess effectiveness of trial drugs on subjective and objective parameters. The patients each in the test and the control Group were assessed on day one before starting the treatment and after administration of the test drugs or the standard control for 3 consecutive cycles. The endocervicitis was considered cured when there is complete resolution of signs and symptoms, improved when there was incomplete resolution of signs and symptoms where as not cured, when there was no apparent response or worsening of signs and symptoms after treatment.18
Statistical Analysis: The results were analyzed statistically using Graph Pad Instat version 3.00 for window (Graph Pad Software, San Diego, Calif, USA) at the completion of the study taking in account the relief of symptoms and healing of the erosion. Results on continuous measurements were presented on Mean (Median) and results on categorical measurements were presented in Number (%). Significance was assessed at 5 % with 95% confidence interval. Subjective parameters were analysed by implying Kruskal-Wallis with Dunn‘s multiple comparisons test (both intra and inter group comparison) while as objective parameters were assessed by Kruskal-
Wallis with Dunn‘s multiple comparisons and Fisher‘s exact (2-tailed) test (both inter and intra group comparison). The safety evaluation was done by Mann Whitney U (two-tailed, independant), Wilcoxan match pair test and Student‘t‘ test (2-tailed, paired and unpaired) for inter and intra group comparison. The overall efficacy of test drugs and control drugs were assessed by Chi-square test.
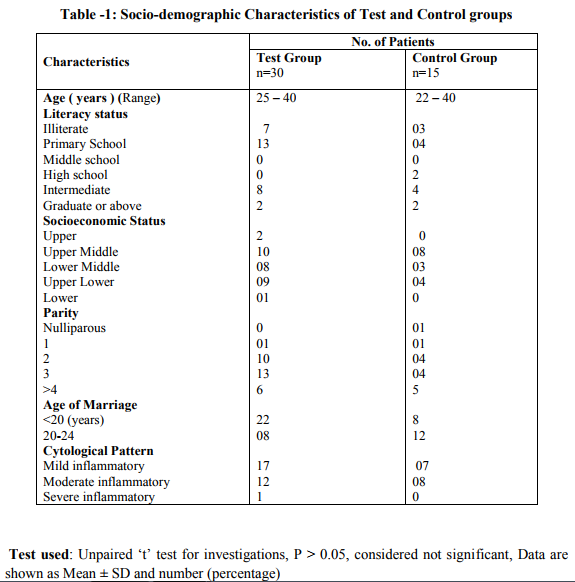
RESULTS The Socio-demographic (literacy status, socioeconomic status, parity, age at marriage) characteristics and investigations of the test and control groups are shown in Table 1. It was found that the parameters were statistically not significant. (P > 0.05) Thus, the groups were homogenous in terms of biochemical parameter and age before intervention. (Table 1)
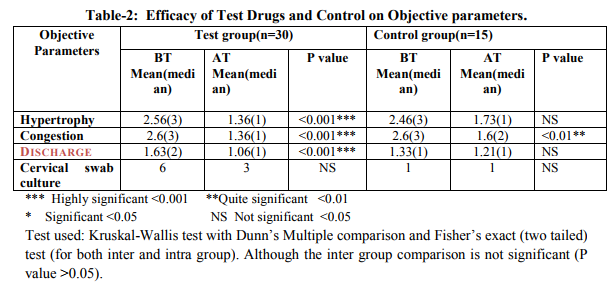
Efficacy of the Test Drugs and Control on Objective parameters
The data was statistically analysed using Kruskal-Wallis test with Dunn‘s Multiple comparison test and Fisher‘s Exact test. The median rating score after treatment in the test group when compared with median rating score before treatment in control and median rating score after treatment in control was found to be significantly reduced (P < 0.05). (Table 2)
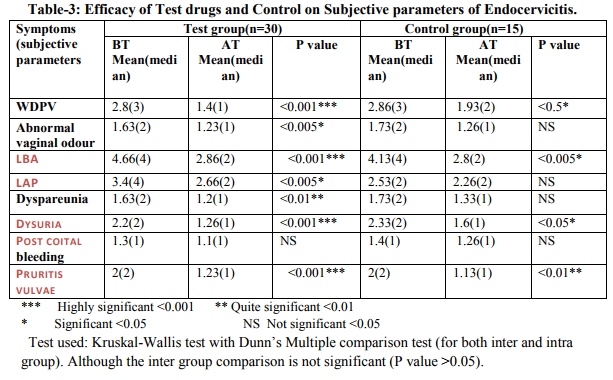
Effect of Test Drugs and Control on Subjective Parameters The most common symptom in the present study was white discharge. The median rating score for white discharge and other symptoms are in the test group after treatment [0(0, 0)] was significantly reduced (P < 0.001) when compared to median rating score with range before treatment of the test and control group. The median rating score of other symptoms are summarized. (Table 3)
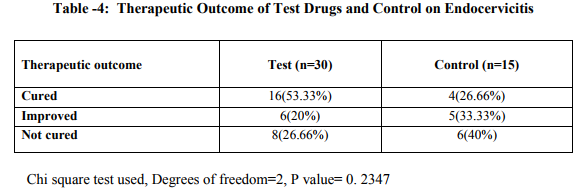
Therapeutic Outcome
In the test Group, out of 30 patients of endocervicitis, 16 (53.33%) patients were cured completely and in the control Group 4(26.66%) patients were cured. The data was analysed by Chi-square test and the comparison revealed that the difference in the cure was significant (P =0.2347). (Table 4)
DISCUSSION
This study demonstrates that the test drugs were effective in the management of endocervicitis. The laboratory investigations were within normal range before and after treatment showing that these drugs were safe. Till date, none of the studies in the Unani system of medicine had evaluated or documented the efficacy and safety of the test drugs in the management of endocervicitis. Thus, it is difficult to correlate the finding with other clinical studies but it validates the claim made by the Unani Scholars. According to the Unani Scholars, Warme ghishae unqur rehm is caused by Ufunat (infection) and it needs dafe tafun (antimicrobial) and mohallil (anti-inflammatory) drugs to relieve infections and associated symptoms like vulval itching, dysuria, postcoital bleeding. Moreover, these drugs are used for healing the wound and ulcers since they are having Musaffie Khoon (blood purifier), Musakkin (analgesic), Qabiz (astringent) and Mundamile qurooh (wound healing) properties. Hence, it is assumed that the properties of the test drugs have caused relief in the sign and symptoms of endocervicitis.
Effect of Test Drugs and Control on Subjective Parameters The most common symptom in the present study was white discharge. The mean and median for WDPV in test group before and after treatment was statistically significant 174 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 with P value <0.001 when compared to mean and median before and after treatment in control group. This improvement may be due to qabiz, mujaffif, mohallil, dafe taffun, musaffie khoon properties of ushba and nakhuna respectively. This result coincides with the findings as documented by Ibn Baitar, 19 Kabeerrudin, 20 Ghani, 21 Roy 22 Gayathri.23 The mean and median for foul smell in test group before and after treatment was statistically significant with P value <0.001 when compared to mean and median before and after treatment in the control group. This improvement may be due to dafe taffun, mujaffif and musaffie khoon properties of ushba and nakhuna. This result coincides with the findings as documented by Ghani 21 and Gayathri.23 The mean and median for pruritus vulvae in test group before and after treatment was significantly reduced with P value <0.00 when compared to mean and median before and after treatment in control group. This improvement may be due to the musaffie khoon, qabiz properties of ushba and nakhuna. This result coincides with the findings as documented by Ibn Baitar 19 andRoy.22
According to VAS score used for assessment of LBA, the mean and median in test group before and after treatment was statistically significant with P value <0.001 when compared to mean and median before and after treatment in control group. The improvement may be due to the mohallil and musakkin properties of the ushba and nakhuna. This result coincides with the findings as documented by Ibn Baitar, 19 Kabeerrudin, 20Ghani 21 and Roy.22
According to VAS score used for assessment of LAP, the mean and median in test group before and after treatment was 3.4(4) and 2.66(2) respectively. It was statistically significant wit P value <0.05 (Kruskal-Wallis with Dunn‘s multiple comparison test) compared to mean and median before and after treatment 2.53(2) and 2.26(2) in control group. The improvement was due to the mohallil and musakkin properties of ushba and nakhuna. This result coincides with the findings documented by Ibn Baitar, 19 Kabeerrudin, 20 Ghani, 21 Roy22 and Gayathri.23
The mean and median for dysuria in test group before and after treatment was statistically significant with P value <0.001 when compared to mean and median before and after treatment in control group. This improvement may be due to mudire boul effect of ushba and nakhuna. This result coincides with the findings documented by Ghani 21 and Roy.22
The Mean and median for dyspareunia in test group before and after treatment was statistically significant with P value <0.001 when compared to mean and median before and after treatment in control group. This improvement may be due to the musakkin properties of the ushba and nakhuna. This result coincides with the findings documented by Ibn Baitar 19 and Kabeerrudin. 20
The mean and median for post coital bleeding in test group before and after treatment was statistically not significant with P value >0 as compared to mean and median before and after treatment in control group. This improvement may be due to the qabiz, dafe qurooh and mujaffif properties of the ushba. This result coincides with the findings documented by Ibn Baitar19 and Kabeerrudin. 20
Effect of Test Drugs and Control on Objective Parameters The mean and median for congestion of cervix in test group before and after treatment was statistically significant with P value <0.001 as compared to mean and median before and after treatment in control group. This improvement may be due to the mohallil, dafe taffun properties of the ushba and nakhuna. This result coincides with the findings documented by Ibn Baitar, 19 Kabeerrudin, 20 Ghani 21and Gayathri.23
The mean and median for hypertrophy in test group before and after treatment was statistically significant with P value <0.001 as compared to the mean and median before and after treatment in control group. This improvement may be due to the mohallil properties of the ushba and nakhuna. This result coincides with the findings documented by Ibn Baitar, 19 Kabeerrudin, 20 Ghani 22and Gayathri.23 It was observed that 3 out of 6 patients after treatment showed cervical swab negative in test group with P value =1.00 (Fisher‘s Exact test, two-tailed) with 95% CI=0.3093=5.44.
All the patients show inflammatory changes in the Pap smear (24-mild, 20- moderate, 1-severe inflammatory smear). Furthermore, It has been Pharmacologically proven that Ushba 21-24 Iklil-ul malik 19-22 , Neem 25 are having antimicrobial and anti-inflammatory property that have inhibited the growth of organism and decreased the inflammation respectively. This finding was well correlated with the study conducted by Parsons WL and Wilson et al who found that inflammatory changes on cytology are associated with cervical infection. 26 The patients were followed up for three months after completion of the trial of the disease to observe the recurrence. However, no recurrence of this disease was found in the patients who got relieved completely of symptoms and signs of endocervicitis except of three patients (1 in test and 2 in control). Moreover, though the response was seen in 53.33% patients, it is appreciable since, antibiotics and antiseptics have limited response in conventional medicine. Further studies with large sample size, double blinding and modified recent techniques are recommended.
CONCLUSION
The endocervicitis is considered as a potential risk factor for sexually transmitted diseases. It is a major public health problem. In addition, the symptoms related to endocervicitis have substantial impact on many aspects of quality of life, including reproductive ability, sexual functioning, mental health and the ability to work and perform routine physical activities. Therefore, it must be treated with due care. This study proves that Unani herbal drugs were found to be safe and effective in the management of endocervicitis when compared to the standard. The study also validated the claim of the Unani physicians in the treatment of endocervicitis.
ACKNOWLEDGEMENT
We are thankful to the Director, National Institute of Unani Medicine, India for providing all the facilities.
References:
1. Kjerulff KH, Erickson BA, Langenberg PW. Chronic gynecological conditions reported by US women: findings from the National Health Interview Survey, 1984-1992. American journal of Public Health 1996; 86(2): 195-199.
2. Carlson KJ, Miller BA, Fowler FJ. The Maine women‘s health study: I. outcomes of hysterectomy. Obstet Gynecol 1994; 83: 556-565.
3. Carlson KJ, Miller BA, Fowler FJ. The Maine women‘s health study: II. Outcomes of nonsurgical management 176 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 of leiomyomas, abnormal bleeding, and chronic pelvic pain. Obstet Gynecol 1994; 83: 566-572.
4. Moore TR, Reiter RC, Rebar RW, Baker VV. Gynecology and ObstetricsA Longitudinal Approach. New York: Churchill Livingstone Inc 1993: 689,832.
5. Brunham RC, et al. Mucopurulent Cervicitis: the ignored counterpart of urethritis in the male. N Engl J Med 1984; 311: 1.
6. Dutta DC. Text book of Gynaecology including contraception. 3rd ed. Calcutta: New Central Book Agency (P) Ltd; 2001: 156-157.
7. Khan RL. Five Teachers Gynaecology.3rd ed. New Delhi: CBS Publishers and Distributors; 2003: 8-9, 89-91.
8. Mukherjee GG, Chakravarty S, Pal B, Mukherjee B. Current Obstetrics and Gynaecology. 1st ed. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2007: 266-67, 272.
9. Patrick DM. Secret Cervicitis? Can Med Assoc J 1998; 158(1): 65-67.
10. Kumar P, Malhotra N. Jefffcoate‘s Principles of Gynaecolgy. 7th ed. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2008: 31-32, 347- 349.
11. Brabin L, Gogate A, Gogate S, Karande A, Khanna R, Dollimore N, et al. Reproductive tract infections, gynaecological morbidity and HIV seroprevalence among women in Mumbai, India. Bulletin of the World Health Organisation 1998; 76(3): 277- 287.
12. McIver CJ, Rismanto N, Smith C, Naing ZW, Rayner B, Lusk MJ, et al. Multiplex PCR testing detection of higher- than –Expected rates of cervical Mycoplasma, Ureaplasma, and Trichomonas and viral agent infections in Sexually Active Australian women. Journal of Clinical Microbial Biology.2009; 47(5): 1358-1363.
13. Esan OG, Osasan SA, Ojo OS. Nonneoplastic diseases of the cervix in Nigerians: A histopathological study. African Health Sciences 2006; 6(2): 76-80.
14. Ahmed SI. Introduction to Al-Umur Al–Tabiyah. 1st ed. New Delhi: Saini Printers; 1980: 16, 42, 76,139,141.
15. Padubidri VG, Daftary SN. Howkins and Bourne Shaw‘s Textbook of Gynaecology. 14th ed. New Delhi: Elsevier; 2008: 7, 293-294.
16. Paavonen J, Critchlow CW, DeRouen T, Stevens CE, Kiviat N, Brunham RC, et-al. Etiology of cervical inflammation. Am J Obstet Gynecol 1986; 154(3): 556-64.
17. Tripathi KD. Essentials of Medical Pharmacology. 4th ed. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2001: 721-722.
18. Dimian C, Nayagam M, Bradbeer C. The association between sexually transmitted diseases and inflammatory cervical cytology. Genitourin Med 1992; 68:305-306.
19. Ibn Baitar. Al Jamul Mufradat al Advia al Aghzia. Vol I. CCRUM; YNM: 116- 117.
20. Kabiruddin M. Makhzanul Mufradat. New Delhi: Ajaz Publishing House; 2007: 74, 401,410.
21. Ghani MN. Khazainul Advia. New Delhi: Idarae Kitabul Shifa; YNM: 87, 255, 266, 945, 946, 1330, 1331, 1332
. 22. Roy, SK, Ali, M, Sharma, MP and Ramachandram, R. New pentacyclic triterpenes from the roots of Hemidesmus indicus. Pharmazie. 2001; 56(3): 244-246.
23. Gayathri M, Kannabiran K. Hypoglycemic activity of Hemidesmus indicus R. Br. on streptozotocininduced diabetic rats. Int J Diab Dev Ctries 2008; 28(1): 6-10.
24. Mahalingam G, Kannabiran K. Hemidesmus indicus root extract ameliorates diabetes-mediated metabolic changes in rats. International Journal of Green Pharmacy 2009; 314- 318
25. Anonymous. The Wealth of India. Vol I. A dictionary of Indian raw material and industrial products. New Delhi: CSIR; 2003: 390-412.
26. Parsons WL, Godwin M, Robbins C, Butler R. Prevalence of cervical pathogens in women with and without inflammatory changes on smear testing. BMJ.1993; 306: 1173-1174
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





