IJCRR - 3(11), November, 2011
Pages: 153-156
Print Article
Download XML Download PDF
PECTUS DEFORMITIES AMONG CHILDREN OF COASTAL ANDHRA PRADESH
Author: Padmasree Dantu, Srinivas Pusuluri
Category: Healthcare
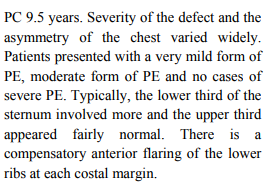
Abstract:Pectus excavatum (PE) and Pectus carinatum (PC) are two common chest deformities. The
present study was conducted with an aim to document the prevalence of chest wall deformities
including PE and PC in Indian population. 22750 children and adolescents aged 7-14 years
consisting of 12628 (55.5%) males and 10122 (44.5%) females were studied who attended
Pediatric and Chest Clinics over a period of 8 years. Subjects with chest wall deformities (PE
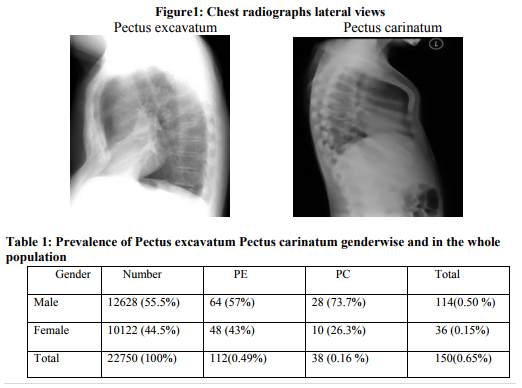
and PC) were traced out. The prevalence of chest deformities in our population is 150 (0.6%).
The mean age of subjects was 11.2 years. Of these subjects 112 (0.49%) [64 (57%) males and
48 (43%) females)] had PE and 38 (0.16%) [28 (73.7%) males and 10 (26.3%) females)] had
PC. The prevalence of PE seems to be high compared to PC in coastal Andhra of India. Chest
deformities should not be considered only as a cosmetic derangement, one should also consider
its functional, social and psychological ramifications.
Keywords: Chest wall deformity, Pectus carinatum, Pectus excavatum.
Full Text:
INTRODUCTION
Pectus deformities are common; about 1 in 400 people have a pectus disorder. Pectus carinatum, occurring in only about 20% of people with pectus deformities. About four out of five patients are males. [1] Pectus carinatum (pigeon chest), is a deformity of the chest characterized by a protrusion of the sternum and ribs. . People with Pectus carinatum usually develop normal heart and lungs, but the deformity may prevent these from functioning optimally. In moderate to severe cases of Pectus carinatum, the chest wall is rigidly held in an outward position. Thus, respirations are inefficient and the individual needs to use the diaphragm and accessory muscles for respiration, rather than normal chest muscles, during strenuous exercise. This negatively affects gas exchange and causes a decrease in stamina. Pectus excavatum is the most common congenital deformity of the anterior wall of the chest, in which several ribs and the sternum grow abnormally. This produces a caved-in or sunken appearance of the chest. It can either be present at birth or not develop until puberty. Pectus excavatum is sometimes considered to be cosmetic; however, depending on the severity, it can impair cardiac and respiratory function and cause pain in the chest and back. People with the abnormality may experience negative psychosocial effects. Pectus excavatum is sometimes referred to as cobbler's chest, sunken chest, funnel chest, chest hole or simply a dent in the chest.[2] Clinical PECTUS DEFORMITIES AMONG CHILDREN OF COASTAL ANDHRA PRADESH Padmasree Dantu1 , Srinivas Pusuluri2 1Maharajah‘s Institute of Medical Sciences, Nellimarla Vizianagaram, Andhra Pradesh 2 Pediatric and Chest Clinics, R.K Mediworld, Visakhapatnam, Andhra Pradesh E-mail of Corresponding Author: docpadmaamc@yahoo.co.in 154 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 symptoms include mild to moderate exercise limitation, respiratory infections and asthmatic conditions. The hallmark of the condition is a sunken appearance of the sternum. The heart can be displaced and /or rotated. Mitral valve prolapse may also be present. Base lung capacity is decreased. Researchers are currently unsure as to the actual cause of Pectus excavatum but hypothesize genetic defect. Approximately 37% of individuals with Pectus excavatum have a first degree family member with the condition. . Pectus excavatum is also a relatively common symptom of Marfan syndrome. Many children with spinal muscular atrophy develop Pectus excavatum due to the diaphragmatic breathing that is common with the disease. Pectus excavatum also occurs in about 1% of persons diagnosed with Celiac disease for unknown reasons. Because the heart is located behind the sternum and individuals with Pectus excavatum have been shown to have visible deformities of the heart (seen both on radiological imaging and after autopsies), it has been hypothesized that there is impairment of function of the cardiovascular system in individuals with Pectus excavatum. While some studies have demonstrated decreased cardiovascular function in Pectus excavatum, there has been no consensus reached of the presence or degree of impairment in cardiovascular function in people with Pectus excavatum based on tests such as echocardiography. Similarly, there is no consensus on the degree of functional improvement after corrective surgery. Children with pectus deformities often tire sooner than their peers, due to shortness of breath and fatigue. Commonly there is a concurrent mild to moderate asthma. Some children with Pectus carinatum also have scoliosis. Some have mitral valve prolapse. Connective tissue disorders involving structural abnormalities of the major blood vessels and heart valves are also seen. Although rarely seen, some children have other connective tissue disorders, including arthritis, visual and healing impairment. Apart from the possible physiologic consequences, pectus deformities can have a significant psychological impact. Some people, especially those with milder cases, live happily with Pectus carinatum. For others, the shape of the chest can damage their self-image and confidence, possibly disrupting social connections and causing them to feel uncomfortable throughout adolescence and adulthood. Physiologically, increased pressure in utero, rickets and increased traction on the sterssnum due to abnormalities of the diaphragm have been postulated as specific mechanisms. Keeping in view if the aforementioned ailments, our study was undertaken to document the prevalence of chest wall deformities (PE and PC) among children of coastal Andhra Pradesh. In the present study the prevalence of PE and PC was identified in a population of about 22750 children.


CONCLUSION
In our study, we were able to show that PE is prevalent in coastal Andhra population. Pectus deformities usually become more severe during adolescent growth years and may worsen throughout adult life. The secondary effects, such as scoliosis and cardiovascular and pulmonary conditions, may worsen with advancing age. Body building exercises (often attempted to cover the defect with pectoral muscles) will not alter the ribs and cartilage of the chest wall, and are generally considered not harmful. Fortunately, most insurance companies no longer consider chest wall deformities like Pectus carinatum to be purely cosmetic conditions. While the psychological impact of any deformity is real and must be addressed, the physiological concerns must take precedence. The possibility of lifelong cardiopulmonary difficulties is serious enough to warrant a visit to a thoracic surgeon.
ACKNOWLEDGMENTS
The authors are grateful to the Management and the Dean, Maharajah‘s Institute Of Medical Sciences, Nellimarla, for their constant encouragement to do research work. The authors express their gratitude 156 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 to the EDP department, MIMS, for their timely help and thank the staff of Pediatric and Chest Clinics for their co-operation during the study over a prolonged period.
References:
1. "Pectus Carinatum, Cincinnati Children's Hospital Medical Center". Cincinnatichildrens.org. 2007-09-26. 3. chief lexicographer: Douglas M. Anderson (2003).
2. "Pectus Excavatum". Spence, Roy A. J.; Patrick J. Morrison (2005). Genetics for Surgeons. Remedica Publishing. ISBN 1-901346-69-2.
3. Westphal FL, Lima LC, Lima Neto JC, et al. Prevalence of pectus carinatum and pectus excavatum in students in the city of Manaus, Brazil. J Bras Pneumol. 2009;35(3):221?6.
4. Haje DP, Haje SA, Simioni MA. Prevalence of pectus carinatum and pectus excavatum in students in the city of Manaus, Brazil. Brasília Med. 2002;39(1/4):10?5. (In Portuguese).
5. Goncalves A, Ferrari I. Characteristics of the occurrence of pectus excavatum in a study of thoracic malformation in preschool children in Sao Paulo. Rev Bras Ortop. 1987;22(1):19?22.
6. Goretsky MJ, Kelly Jr. RE, Croitoru D, Nuss D. Chest wall anomalies: Pectus excavatum and pectus carinatum. Adolesc Med Clin. 2004; 15(3):455?71.
7. Fonkalsrud EW, Dunn JC, Atkinson JB. Repair of pectus excavatum deformities: 30 years of experience with 375 patients. Ann Surg. 2000; 231(3):443?8.
8. de Matos AC, Bernardo JE, Fernandes LE, Antunes MJ. Surgery of chest wall deformities. Eur J Cardiothorac Surg. 1997;12(3):345?50.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





