IJCRR - 8(16), August, 2016
Pages: 05-08
Date of Publication: 22-Aug-2016
Print Article
Download XML Download PDF
ANATOMIC CONFIGURATIONS OF EXTERNAL BRANCH OF SUPERIOR LARYNGEAL NERVE AND SUPERIOR THYROID ARTERY: A STUDY IN CADAVERS
Author: Swapnali Shamkuwar, PS Bhuiyan
Category: Healthcare
Abstract:Objectives: Thyroidectomy is one of the commonly performed procedures in head and neck surgery. Injury to the external branch of superior laryngeal nerve occurs frequently in thyroid surgery which can result in voice changes in the patient. The aim of the present study is to study the anatomical relationship between external branch of superior laryngeal nerve and superior thyroid artery.
Methods: Sixty specimens of the thyroid gland of both sexes were studied. The distance between superior pole of thyroid gland and crossing point of superior thyroid artery and external branch of superior laryngeal nerve was measured and recorded.
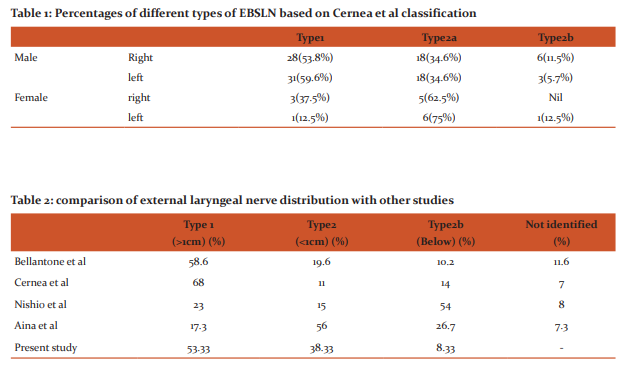
Results: The external laryngeal nerve was categorized into three types. In 63 (52.5%) cases the nerve crossed the superior thyroid artery more than 1cm (type1) and in 47 (39.16%) cases it crossed the artery less than 1cm (type 2a) above the upper pole of the thyroid gland. In 10 (8.33%) cases the nerve crossed the artery under cover (type 2b) of upper pole of the thyroid gland.
Conclusions: A sound knowledge of the anatomy of the external laryngeal nerve and its relation to superior thyroid artery and superior pole of thyroid gland is helpful to minimize lesions of the nerve and perform safe surgery on thyroid gland.
Keywords: Superior laryngeal nerve, Superior thyroid artery, Thyroid gland
Full Text:
INTRODUCTION
The superior laryngeal nerve (SLN)arises from vagus nerve after it leaves the skull base. It typically originates from the vagus at the no dose ganglion 1 and divides into an internal and external branch at the level of superior cornu of hyoid bone2 . The external branch of superior laryngeal nerve (EBSLN) first descends dorsolaterally to the carotid arteries and extends medially towards the larynxand usually crosses the superior thyroid artery(STA) near the thyroid gland. After giving off some twigs to the inferior pharyngeal constrictor, the EBSLN terminates mainly within the cricothyroid muscle3 . The course of the EBSLN in the neck places it at risk during thyroid or parathyroid surgery, carotid end arterectomy and anterior approaches to the cervical spine4 .Preservation of the EBSLN is important for optimal function of the larynx5 . It gives nerve supply to same side cricothyroid muscle6 to tense the vocal cord4 . Ipsilateral paralysis of cricothyroid muscle occurs due to damage of EBSLN5 which can lead to changes in voicequality and projection1 . EBSLN is highly vulnerable during ligation of superior thyroid artery of thyroid gland 6 . Because of the close relationship between STA and EBSLN it may be inadvertently stretched, ligated or transacted 4 .The topographical relationship to the STA and the upper pole of the thyroid gland represents the key point for identifying the EBSLN during surgery of the neck. When these two landmarks are considered, identification and protection of the nerve are easy3 .Cernea7 carried out a study to identify the EBSLN and analyze its anatomical relations with the superior pedicle of the thyroid gland.
THE CERNEA EBSLN CLASSIFICATIONSCHEME IS AS FOLLOWS:
The type 1 nerve crosses the superior thyroid vessels more than 1 cm above the upper edge of the thyroid superior pole The type 2A nerve crosses the vessels <1 cm above the upper edge of the superior pole The type 2B nerve crosses the superior thyroid pedicle below the upper border of the superior thyroid pole. In 1998, Kierner et al added a fourth category in which EBSLN runs dorsal to the superior thyroid artery. Type4 ESBLN observed in 13% of their dissection studies3 and was considered more difficult to visuallyidentify1 . Kokocharov et al. described the EBSLN as being very close to the superior thyroid artery and vein, usually in a medial position to these vessels. These authors have suggested that dissection of the blood vessels should be done at least for 1.5 to 2 cm away from the entry point of these vessels into the thyroid capsule to avoid injury to the EBSLN8 . Thus the aim of the present study was to measure the distance between the crossing point of EBSLN and STA and the superior pole of the thyroid gland8 and categorize the nerve into three types according to Cerena et al 7 .
MATERIALS AND METHODS
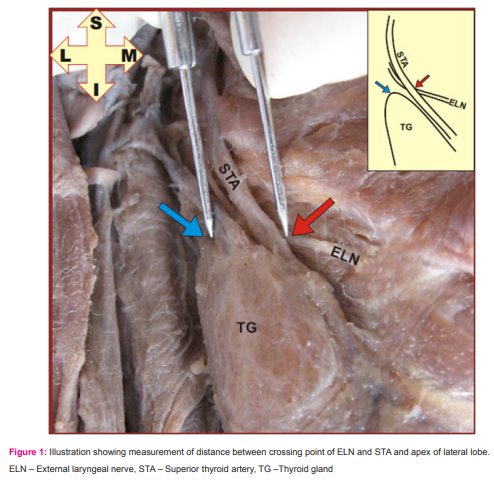
Sixty specimens (8 females and 52 males) of the thyroid gland obtained from sixty cadavers, embalmed using 10% formalin were used for the study. In each cadaver, the thyroid gland was looked for any gross deformity, tumour or trauma. Dissection of the thyroid gland was done systematically. Crossing point between superior thyroid artery and external laryngeal nerve was noted and recorded. The distance between crossing point of artery and nerve and most prominent point on the apex of the lobe was measured on both sides as shown in figure 1. All these measurements were statically analysed using the SPSS – program. Student’s t test was used to evaluate the mean differences of the measured parameters on right and left sides. The influence of gender of cadavers on the position of nerves was not analysed due to the great difference in the available number of male and female specimens.
RESULTS
The distance between crossing of superior thyroid artery and external laryngeal nerve and superior pole of thyroid gland was measured and this data was classified according to Cerena et al 7 . The mean distance was 0.96cm ± 0.50cm on the right and 1.10cm ± 0.4cm on the left. Using independent ttest no statistical significance was found on the right and left sides (p – value = 0.287). In 32 cases (53.33%) the EBSLN crosses the STA 1 or more cm above a horizontal plane on both sides (Table 1). Type 2b ESBLN was found in 22 cases (26.66%) on right side and 24 cases (36.66%) on left side. Crossing of artery and nerve was below the superior pole of the thyroid gland in 6 cases (10%) on right side and in 4cases (6.66%) on the left side. Within the 60 thyroid glands that was dissected, the predominance of type 1 nerve was obvious on both sides. The most common type of EBSLN was type 2a nerve on both sides in females and type 1 nerve was dominant on both sides in males.
DISCUSSION
The principals of head and neck surgery are based on identification and preservation of important structures. The EBSLN is considered at risk in each patient until it is identified. The surgical importance of the EBSLN is due to the close anatomical relationship between the nerve and superior thyroid artery at the superior pole of the thyroid gland5
In the present study, type 1 external laryngeal nerve distribution was found to be 53.33% which closely resembles the findings of Cerena et al, Bellantone et al 9 (Table 2) but was higher than the study of Nishito etal10 and Aina et al 11In the present study, type 2a external laryngeal nerve distribution was found to be 38.33% which was double compared to the findings of Bellatone et al. The most common type of distribution of external laryngeal nerve was found to be type 1 in the present study which is similar to the findings of Cerena et al and Bellatone et al but findings by Nishito et al had shown type 2b the most common(60%). Type 2b was the least common type in the present study and study by Bellantone et al whereas type 2a was the least common type in study of Cerena et al and Nishito et al. Type 2a and 2b are particularly prone to injury during dissection and ligation of the superior thyroid vessels due to their low lying course. They reasoned that if the nerve crosses within 1 cm the ‘critical centimetre’ of the superior pole it should be considered ‘at risk’ during thyroid surgery 4 . In the present study in majority of cases nerve was crossing the artery more than one centimetre above the thyroid gland but in some cases it was crossing the artery close to the thyroid gland.
Awareness of these anatomical variations demands careful dissection around the superior thyroid pole. According to literatureit is safe to ligate superior thyroid artery as close to the superior pole of thyroid gland as possible and our study results also suggest the same. However this procedure must be done with utmost care and precaution because in few cases the nerve crosses the artery very close to the thyroid gland.
CONCLUSION
Thorough knowledge of the anatomical relationship between EBSLN, superior thyroid artery and upper pole of the thyroid gland and categorization of the EBSLN enable the otolarygologists, endocrine surgeons and laryngologists to have safe surgery and reduce the morbidity to minimum.
References:
1. Barczynski, M, Randolph G W, Cernea CR, Dralle H, DionigiG, Alesina PF, Mihai R External Branch of the Superior Laryngeal Nerve MonitoringDuring Thyroid and Parathyroid Surgery: International Neural Monitoring Study Group Standards Guideline Statement. Laryngoscope2013; 123: s1-s14.
2. Taytawat P. Viravud Y DDS, Plakornkul V DVM, Roongruangchai J DDS, Manoonpol C Identification of the External Laryngeal Nerve: Its Anatomical Relations to Inferior Constrictor Muscle, Superior Thyroid Artery, and Superior Pole of the Thyroid Gland in Thais. J Med Assoc Thai 2010; 93 (8): 961-8.
3. Kierner AC, Aigner M, Burian M. The External Branch of the Superior Laryngeal Nerve Its Topographical Anatomy as Related to Surgery of the Neck Arch Otolaryngol Head Neck Surg. 1998;124(3):301-303.
4. Morton R P, Whitfield P, Al-Ali S Anatomical and surgical considerations of the external branch of the superior laryngeal nerve: a systematic review Clinical Otolaryngology 2006;31:368–374.
5. Friedman M, LoSavio P, Ibrahim H. Superior laryngeal nerve identification and preservation in thyroidectomy. Arch Otolaryngol Head Neck Surg 2002; 128: 296-303.
6. Thiagarajan B, Ramamoorthy G. Preventing Nerve Damage During Thyroid Surgeries. Webmed Central otorhinolaryngology 2012;3(4):wmcoo3260.
7. Cerena CR, Ferraz AR, Furlani J, Monterio S. Identification of the external branch of superior laryngeal nerve during thyroidectomy. The American Journal of Surgery 1992Dec;164:634-9.
8. EstrelaF, LeãoHZ, JotzGP Anatomic relation between the external branch of the superior laryngeal nerve and the thyroid gland. Brazilian journal of otolaryngol 2011 March- April; 77(2):249- 58.
9. Bellantone R, Boscherini M, Lombardi CP, Bossola M, Rubino F, De Crea C, et al. Is the identification of the external branch of the superior laryngeal nerve mandatory in thyroid operation Results of a prospective randomized study. Surgery 2001; 130: 1055-9.
10. Cernea CR, Nishio S, Hojaij FC. Identification of the external branch of the superior laryngeal nerve (EBSLN) in large goiters. Am J Otolaryngol 1995; 16: 307-11.
11. Aina ENHisham ANExternal laryngeal nerve in thyroid surgery: recognition and surgical implications. ANZ J Surg 2001 April; 71(4):212-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





