IJCRR - 3(11), November, 2011
Pages: 66-79
Print Article
Download XML Download PDF
EFFECT OF DIODE LASER IN THE TREATMENT OF PERIODONTAL POCKETS- A CLINICAL AND
MICROBIOLOGICAL STUDY USING POLYMERASE CHAIN REACTION
Author: M.Priyanka, T.Rmakrishnan, N.Ambalavanan, Pandi Suba K., Prasanna C.C.
Category: Healthcare
Abstract:Aims and objectives: The aim of this study was to compare the clinical efficiency of a Diode laser as an adjunct to SRP with SRP alone in the treatment of chronic periodontitis patients and
also to evaluate the changes in the clinical and microbiological parameters.
Materials and methods: Total number of 40 deepest sites in 10 chronic periodontitis patients was selected in this split mouth designed study. In each patient upper and lower right quadrants
were assigned into one group and upper and lower left quadrants into the other. Treatment for
each group was decided using a coin toss method, where Group A (Control) received only conventional SRP and Group B (Test) received conventional SRP and Laser assisted pocket debridement. The clinical parameters (Plaque index, Bleeding on probing, Probing pocket
depth, Clinical attachment level) were recorded at baseline and 90th day and the microbiologic
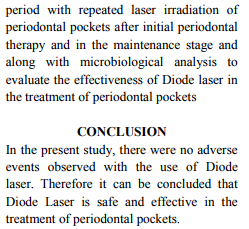
assessment for Aa, Pg and Pi were done on 7th, 21st and 90th day for both the groups.
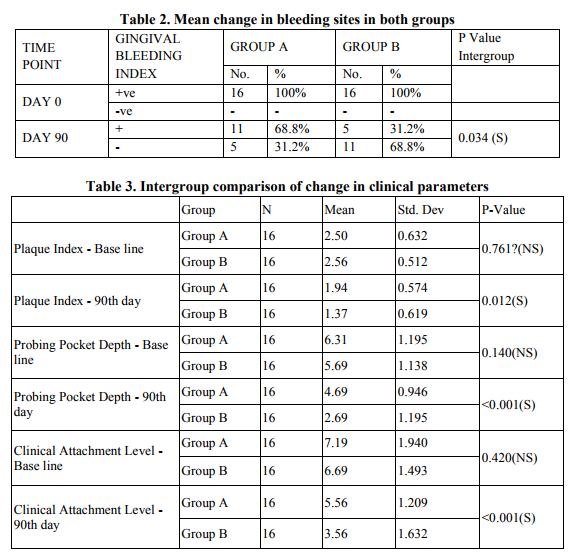
Results: Out of the 10 patients, 2 patients who were irregular for the treatment protocol were excluded. When both groups were compared there was statistically significant reduction in
Plaque index, Bleeding on probing, Probing pocket depth and gain in Clinical attachment level
in Group B when compared to Group A. There was statistically significant reduction in
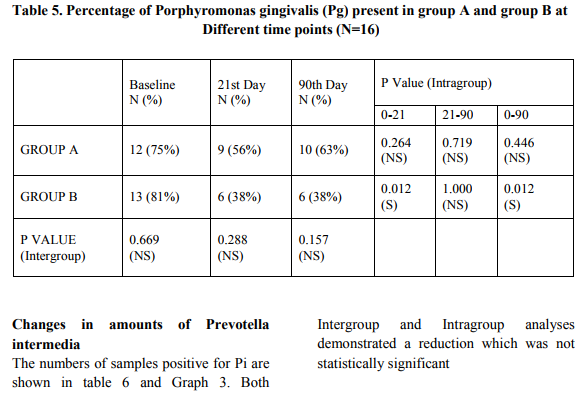
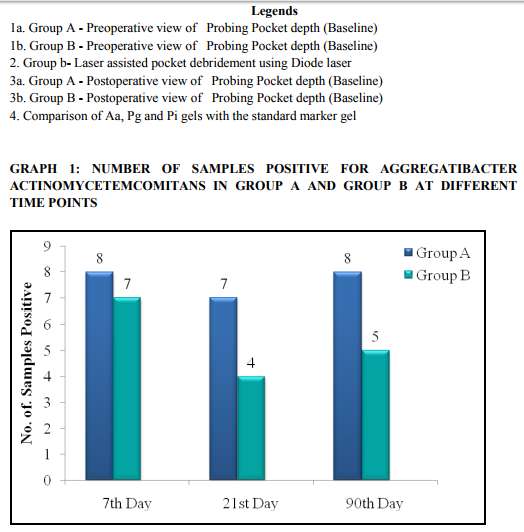
Porphyromonas gingivalis from baseline to 90th day in Group B when compared to Group A.
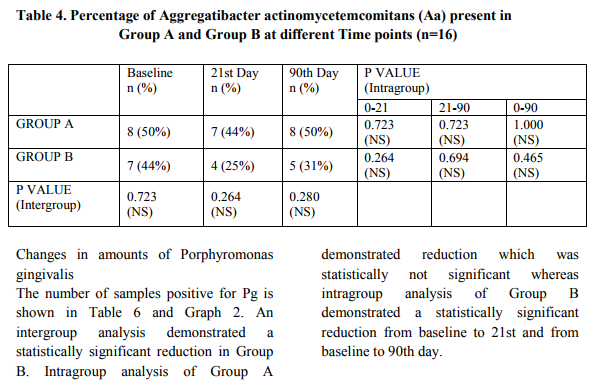
There was no statistically significant reduction in Aggregatibacter actinomycetemcomitans and
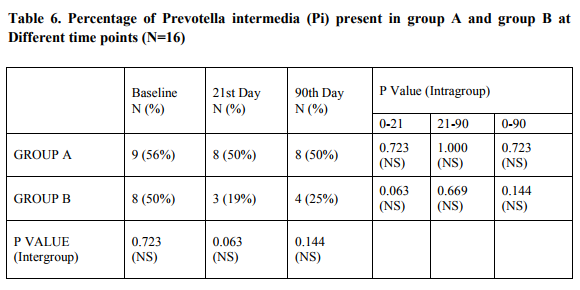
Prevotella intermedia in both the groups.
Conclusion: From the results observed in this study it can be concluded that use of Diode laser
as an adjunct to SRP was found to be efficacious and safe.
Full Text:
INTRODUCTION
Chronic periodontitis is initiated by microbial plaque, which accumulates on the tooth surface at the gingival margin and induces an inflammatory reaction. The inflammatory response in patients with chronic periodontitis results in the destruction of the periodontal tissues. With a constant bacterial challenge the periodontal tissues are continuously exposed to the specific bacterial components that have the ability to alter many local cell functions.1 Basically the aim of the periodontal treatment is to restore the biological compatibility of the periodontally diseased root surfaces for subsequent attachment of periodontal tissues to the treated root surfaces.2 EFFECT OF DIODE LASER IN THE TREATMENT OF PERIODONTAL POCKETS- A CLINICAL AND MICROBIOLOGICAL STUDY USING POLYMERASE CHAIN REACTION M.Priyanka1 , T.Rmakrishnan1 , N.Ambalavanan1 , Pandi Suba K.2 , Prasanna C.C.2 1Department of Periodontology, Meenakshi Ammal Dental College MAHER University, Chennai 2Central Research Laboratory, Meenakshi Ammal Dental College and Hospitals, MAHER University, Maduravoyal, Chennai E-mail of Corresponding Author: Priyanka13_28@yahoo.com 67 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 Complete removal of the bacterial deposits and their toxins from root surface and within the periodontal pockets is not necessarily achieved with conventional mechanical therapy and access to areas such as furcations and grooves is limited owing to the complicated root anatomy.2 There has been growing interest in recent years to search for new machine driven therapeutic devices which are capable of improving and simplifying mechanical root surface management and displaying antibacterial properties in order to decrease the number of bacteria associated with periodontal pockets. In this respect laser radiation at different wavelengths has been investigated as a novel system and an adjunct to conventional therapy.2
Although dental plaque ;harbours a great number of bacterial species, only a limited group of organisms has truly pathogenic potential. Dzink3 and Takeuchi4 et al in their studies have shown that Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans are responsible for destructive periodontal diseases. Yano-Higuchi5 et al stated that the proportion of Porphyromonas gingivalis is significantly correlated to the aggrevation of the clinical parameters. Lopez6 et al in their study have shown the elevated levels of Prevotella intermedia in progressing sites of chronic periodontitis. Tseng7et al stated that besides eliminating Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Prevotella intermedia, subgingivally, it has been affirmed that laser can enhance SRP. This study was designed to compare the clinical efficiency of a Diode laser as an adjunct to SRP with SRP alone in the treatment of chronic periodontitis patients and also to evaluate the changes in the clinical and microbiological parameters.
MATERIALS AND METHODS
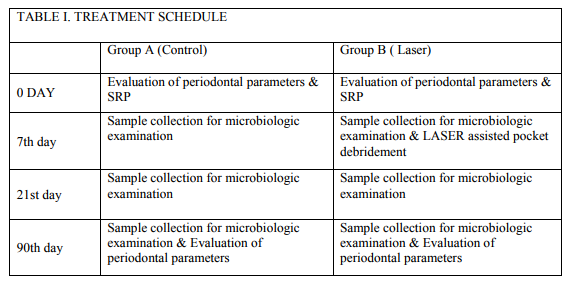
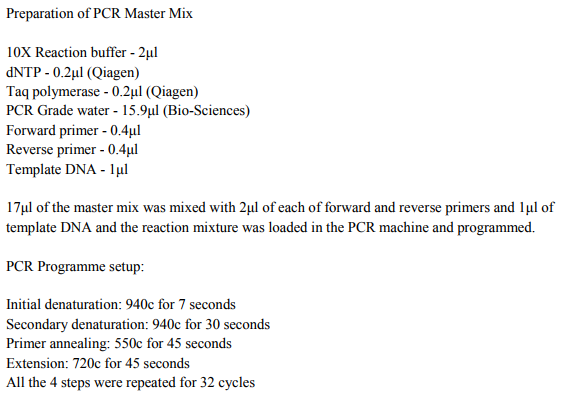
Ten Chronic periodontitis patients both males and females, aged 30 to 55 years, having a probing pocket depth of ≥5mm in 4 to 6 sites of all the quadrants were selected for the study. Patients were selected from the patient pool of the Department of Periodontics, Meenakshi Ammal Dental College, Chennai. Ethical clearance for the study was obtained from the ethical committee of the MAHER University. Written informed consent was obtained from the patients. Patients with age group 30 to 55 years, Teeth with ≥5mm probing pocket depth, Patients who can maintain good oral hygiene were included and Patients with systemic disease, Use of tobacco, Use of antibiotics or any form of periodontal treatment in the previous 6 months were excluded from the study. Total number of 40 deepest sites in 10 chronic periodontitis patients was selected in this split mouth designed study. In each patient upper and lower right quadrants were assigned into one group and upper and lower left quadrants into the other. Treatment for each group was decided using a coin toss method. Where Group A received only conventional SRP and Group B received conventional SRP and Laser assisted pocket debridement. Table 1 illustrates the treatment schedule that determined the different examination and treatment steps.
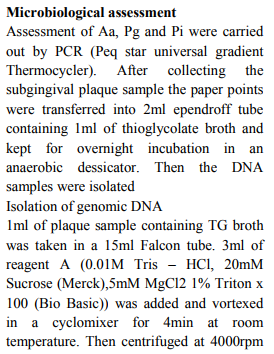
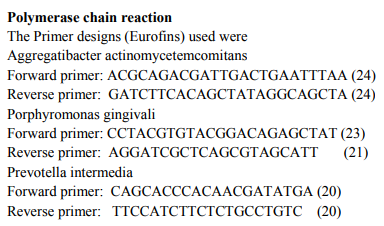
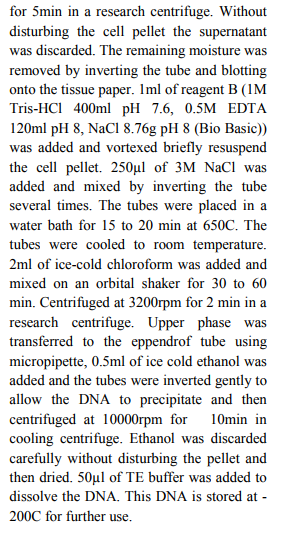
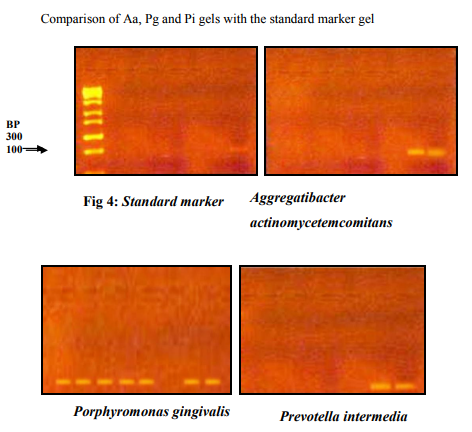
Plaque index (Silness and Loe), Bleeding index (Ainamo and Bay), Probing Pocket depth and Clinical attachment level were evaluated on baseline and 90th day. Subgingival plaque samples were collected from both the groups. The total count of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis and Prevotella intermedia were assessed at different time points using PCR.
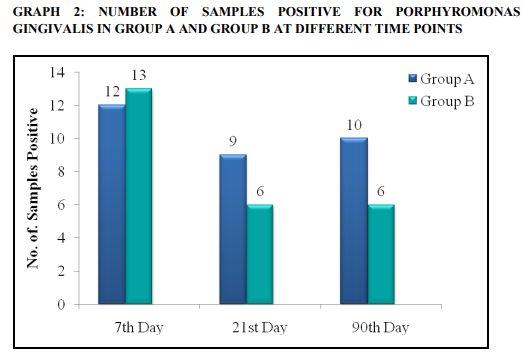
Sub-gingival plaque sample collection: The tooth with deepest pocket of the quadrant was isolated with a cotton roll and air dried and an ISO Standardized absorbent paper points of 25 size were placed within the pocket using a sterile tweezer for a period of 30 sec and then immediately transferred into a sterile ependroff tube containing thioglycollate broth and transported immediately to the laboratory. At baseline, all periodontal parameters were assessed and full mouth scaling and root planing was done. (Fig 1a and 1b shows the pre operative measurements of Pocket depths in both groups)
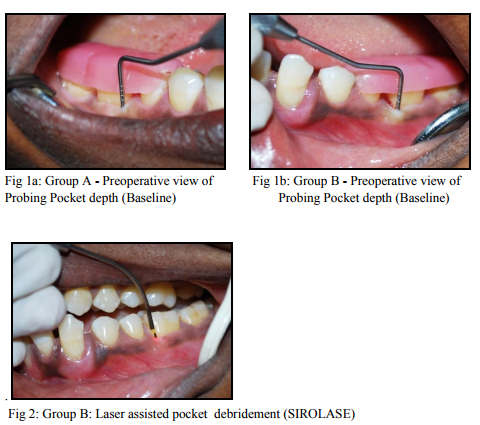
On 7th day, sub gingival plaque samples were collected from both the groups before laser assisted pocket sterilization was done in group B. Diode laser (SIRO Laser, class IV Diode Laser, with an active semiconductor medium (Gallium,
Aluminium, Arsenide) with a wavelength of 970+/-15nm) is used for the pocket debridement with an optical fiber of 320µm diameter, with an output power of 1 watts in a continuous mode with all the other parameters in a preset mode. The calibration of the fiber was the depth of the treatment site minus 1mm. This measurement allows for the laser energy to penetrate the tissue and reduce the bacterial load without the fiber actually touching the epithelial attachment at the bottom of the pocket. The fiber is placed on the tissue at the top of the sulcus, directing the laser energy away from the tooth structure, and moved towards the bottom.(Fig 2.Laser therapy in Group B) The fiber is moved both horizontally and vertically, and contact is maintained with the soft tissue down to the calibrated depth of the fiber. The pocket is sterilized with the laser for around 30 sec per tooth. The fiber must be inspected frequently and any accumulated tissue and debris must be wiped off to avoid inefficiency. Bacterial reduction is complete when signs of fresh bleeding occur. Post operative instructions following laser soft tissue procedures may include: analgesics as needed, such as Ibuprofen, avoidance of foods that could cause 69 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 irritation to healing tissue, for three to five days. On 21st day sub-gingival plaque samples were collected from both the groups On 90th day all the periodontal parameters were assessed and sub-gingival plaque samples were collected from both groups for microbiological assessment. (Fig 3a and 3b shows the pre operative measurements of Pocket depths in both groups)




References:
1. Flemmig TF, Rudiger S, Hofmann U, Schmidt H, Plaschke B, Stratz A, Klaiber B and Karch H. Identification of Actinobacillus actinomycetemcomitans in subgingival plaque by PCR. J Clin Microbiol 1995; 33(12): 3102-3105.
2. Aoki Akira, Katia Miyuki Sasaki, Hisashi Watanabe and Isao Ishikawa. Lasers in nonsurgical periodontal therapy. Periodontol 2000 2004; 36: 59–97.
3. Dzink J.L, Tanner A.C.R, Haffajee A.D and Socransky S.S. Gram negative species associated with active destructive periodontal lesions. J Clin Periodontol 1985; 12: 648–659.
4. Takeuchi, Y., Makoto, U., Motoko, I., Huang, Y. and Ishikawa, I. Prevalence of periodontopathic bacteria in aggressive periodontitis patients in a Japanese population. J Periodontol 2003; 74: 1460–1469.
5. Yano-Higuchi, K., Takamatsu, N., He, T., Umeda, M. and Ishikawa, I. Prevalence of Bacteroides forsythus, Porphyromonas gingivalis and Actinobacillus actinomycetemcomitans in subgingival microflora of Japanese patients with adult and rapidly progressive periodontitis. J Clin Periodontol 2000; 27: 597-602.
6. López Rodrigo, Gunnar Dahlén, Carolina Retamales, Vibeke Baelum. Clustering of subgingival microbial species in adolescents with periodontitis. European Journal of Oral Sciences 2011; 119(2): 141-150.
7. Tseng, P., Gilkeson, C. F., Pearlman, B. and Liew, V. J Dent Research 1991;70: 657 (abstract no. 62).
8. Ambrosini P, Miller N, Brianc¸on S, Gallina S, Penaud J. Clinical and microbiological evaluation of the effectiveness of the Nd:Yap laser for the initial treatment of adult periodontitis. A randomized controlled study. J Clin Periodontol 2005; 32: 670–676.
9. Qadri T, Miranda L, Tune´r J, Gustafsson A. The short-term effects of low-level lasers as adjunct therapy in the treatment of periodontal inflammation. J Clin Periodontol 2005; 32: 714–719.
10. Sakurai Y, Yamaguchi M, Abiko Y. Inhibitory effect of low level laser irradiation on LPS- stimulated prostaglandin E2 and cyclooxygenase- 2 in human gingival fibroblast. Eur J Oral Sci 2000; 108: 29-34.
11. Karu, T. Low-power laser therapy. In: Biomedical Photonics Handbook. Tuan Vo-Dinh, Ed. CRC Press 2003; 48: 1– 24
12. RomanosHYPERLINK "http://www.ncbi.nlm.nih.gov/pubmed ?term=%22Romanos%20GE%22%5B Author%5D" GE. Clinical applications of the Nd:YAG laser in oral soft tissue surgery and periodontology. J HYPERLINK "http://www.ncbi.nlm.nih.gov/pubmed/ 10147186"ClinHYPERLINK "http://www.ncbi.nlm.nih.gov/pubmed/ 76 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 10147186" Laser Med HYPERLINK "http://www.ncbi.nlm.nih.gov/pubmed/ 10147186"Surg 1994; 12(2): 103-8.
13. Eun-Jeong Choi, Ju-Young Yim, KiTae Koo, Yang-Jo Seol, Yong-Moo Lee, Young Ku, In-Chul Rhyu, ChongPyoung Chung, Tae-Il Kim. Biological effects of a semiconductor diode laser on human periodontal ligament fibroblasts. J Periodontal Implant Sci 2010; 40(3): 105–110.
14. Moritz A, Schoop U, Goharkhay K, et al. Treatment of periodontal pockets with a diode laser. Lasers Surg Med 1998; 22(5): 302–11.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





