IJCRR - 4(18), September, 2012
Pages: 176-183
Date of Publication: 29-Sep-2012
Print Article
Download XML Download PDF
THE EFFECT OF COMBINED VITAMIN E AND C SUPPLEMENTATION ON THE OXIDATIVE STRESS PARAMETERS IN PATIENTS WITH SCHIZOPHRENIA
Author: Santoshi R. Ghodake, A. N. Suryakar, Abdul Kayyum Shaikh, Prabhakar M. Kulhalli, R.K. Padalkar, A. M. Raut
Category: Healthcare
Abstract:Recently, it is proposed that oxidant- antioxidant imbalance may have a role in the pathophysiology of schizophrenia. The present study was performed to assess differences in plasma levels of Malondialdehyde (MDA), as an oxidant product, antioxidant such as superoxide dismutase (SOD), reduced glutathione (GSH), vitamin E (\a-tocopherol), vitamin C (ascorbic acid) etc., and total antioxidant capacity(TAC) in the patients with schizophrenia as compared with healthy controls. Our secondary aim was to further evaluate the effect of combined supplementation of antioxidant vitamins E and C along with antipsychotics treatment on these parameters. The study includes prospective, double blind, non-crossover, and 12 weeks intervention of antioxidants. Plasma levels of MDA, erythrocytes SOD, GSH, vitamin E, vitamin C and TAC levels in plasma in patients with schizophrenia before (n=40) and after regular antipsychotic treatment (n=20) and treatment with antipsychotics plus antioxidant E and C supplementation (n=20) were compared with healthy controls (n=40). The levels of MDA were significantly increased in patient before treatment while the levels of SOD, GSH, vitamin E and C and TAC in plasma shown significant reduction. However, the antioxidant supplementation along with antipsychotics reverses the above levels. PANSS (positive and negative syndrome scale) change scores at 12 weeks improved statistically significant with antioxidant E and C supplementation as compared to alone antipsychotics treatment. So oral supplementation of antioxidants in combination reduces oxidative stress and improves clinical symptoms suggest the application of antioxidant in clinical trials is beneficial to prevent or reduces the progression of disease.
Keywords: oxidative stress, schizophrenia, Treatment, vitamin C, vitamin E.
Full Text:
INTRODUCTION
Schizophrenia is a devastating mental disorder, expressed in the form of abnormal mental functions and disturbed behavior. It has a life-time prevalence of approximately 1% of the world?s population. The disorder has a bad outcome, regardless of different treatment (pharmacological, social, cognitive etc.). Oxidative stress is common to several neuropsychiatric disorders. The mechanisms have been most widely studied in schizophrenia, employing various areas of research, including oxidative biomarkers, psychopharmacology and clinical studies with antioxidants (1). The aetiopathogenesis of neuropsychiatric disorders is incompletely understood, which may partly account for the persisting dominance of the syndrome nosology in neuropsychiatry, despite its widely recognized inadequacies. Oxidative stress mechanism have been implicated in the pathogenesis has theoretical appeal, as the brain is considered particularly vulnerable to the damage for several reasons (2). The oxidative vulnerability of the brain, with growing evidence for neuropsychiatry syndromes, suggests that oxidative damage may be a plausible pathogenic candidate (2). In fact, experimental models have demonstrated that oxidative stress induces behavioral and molecular anomalies strikingly similar to those observed in schizophrenia. Thus the extant evidence for the role of oxidative stress in the pathophysiology of neuropsychiatric disorders such as Schizophrenia, Depression, Alzheimer?s disease, Epilepsy etc. offers a hypothesis derived therapeutic approach in the form of antioxidants. Vitamin E and vitamin C are well known antioxidants that are postulated to protect against damage to biological membranes by their ability to scavenge free radicals. Accordingly, several studies have examined the efficacy of vitamin E or vitamin C in the treatment of schizophrenia (1, 3). Treatment of schizophrenia, particularly the most disturbing symptoms is considered to be very difficult. This is because treatment with both typical as well as atypical antipsychotics has serious side effects that lead to a significant loss of quality of life. It is important to develop alternative or adjunctive treatment strategies that may augment the antipsychotic action and reduce the side effects. Clinical trials investigating adjunctive antioxidants in the treatment of schizophrenia and depression have utilized vitamin E and vitamin C, Ginkgo biloba extract and N-acetyl cysteine (NAC) have been considered for some to improve the outcome of these diseases (2). Supplementation has been done, first with vitamin C with haloperidol reported no symptomatic improvement (4). Then vitamins E/C along with omega – 3 fatty acids, shown significant symptomatic improvement, but no significant change in oxidative products has been found (5). Some studies showed reversal of MDA, ascorbic acid and SOD levels along with improved positive and negative symptoms, extrapyramidal side effects and superior BPRS outcome (6,7). As the evidence is increasing for the increased oxidative stress and oxidative cellular injury in various neuropsychiatric disorders, use of more than one antioxidant vitamin may be the preferred supplementation. Thus the use of antioxidants is critical since peroxidative membrane injury may contribute to pathophysiology and must be prevented (8). It is also important to point out that the number of studies has reported variable therapeutic effects of dietary antioxidants, primarily vitamin E on tardive dyskinesis (9). Supplementation with vitamin C, an effective intracellular antioxidant, has not been tried, although its use in preventing intracellular peroxidative injury and restoration of active vitamin E for the prevention of membrane lipid peroxidation has been suggested (8). There is a lack of information on oxidative process in cerebrospinal fluid and brain. Considering the size of the CNS in comparison to the other compartments of the human body, it seems reasonable to assume that changes in the levels of various biomolecules inside the brain can influence the plasma levels of those biomarkers. This was concluded by various studies on CNS (CSF, post mortem or animals) showed at least correlative tendencies with studies assaying biomarkers in erythrocytes, plasma or polymophonuclears (1). So most of the oxidative stress in patients with schizophrenia have made on peripheral tissues. The patients with schizophrenia had increased serum Malondialdehyde levels and decreased plasma ascorbic acid levels, which proves increased oxidative stress. These levels were significantly reversed after treatment with vitamin C along with atypical antipsychotics compared to placebo with atypical antipsychotics. BPRS scores improved significantly with addition of vitamin C as compared to placebo after 8 weeks of treatment (6). The supplementary use of vitamin C in schizophrenia requires caution since a high dietary intake of iron will result in vitamin C having a pro-oxidant rather than an antioxidant action. Vitamin E is a lipid soluble antioxidant with the potential to prevent oxidative damage. However, vitamin E cannot prevent oxidative damage to cytosolic proteins, mitochondria, and nuclei, where most of the ROS are generated. Therefore, it may be important to use vitamin E in combination with vitamin C. Addition of vitamin C probably reduces this risk because of its interactions with vitamin E, i.e. vitamin C reduces vitamin E radicals formed when vitamin E scavenges the oxygen radicals (10). Also, theses vitamins are suitable for human clinical trials because they are readily available, inexpensive and relatively safe (11). We have therefore tested the safety and efficacy of combining vitamin C and E in a sample of patients. So, aim of this study was to explore the beneficial effects of combined supplementation of vitamin E and C on oxidative stress parameters in schizophrenia patients. Also to suggest the new therapeutic approaches using appropriate antioxidants which might partially alleviate or prevent the symptoms of schizophrenia.
MATERIALS AND METHODS
This prospective cohort study, 12 weeks trial was carried out in the department of Biochemistry and outpatient and inpatient department of Psychiatry, PDVVPF?s Medical College, Ahmednagar, India. Study group consist of a control group of healthy subjects and that of schizophrenia selected consecutively. Healthy subjects more than 18 years of age, of both sexes, more than 50 kilograms weight, taking good diet, non-smokers, and non-alcoholic, free of any medication for at least one month prior to study were selected as controls. These were enrolled from the general population and academic community. The research protocol and consent forms were approved by institutional ethics committee. Some the patients had a decision-making capacity and consented for the study signed the consent form, but most of the cases, the consent form was signed by the family members. After taking consent and screening with routine investigations, physical examination. Fasting blood samples were obtained at 0 weeks and at the end of 12th weeks from the start of the treatment. After initial analysis subjects were divided into to two groups by stratified sampling. First group receiving regular antipsychotic treatment (consisting of haloperidol, dose decided by psychiatrist, depends on severity) and second group allow receiving antioxidant vitamins E and C along with antipsychotic treatment. The vitamin supplementation was carried out by supplying both vitamin E (400 IU, dl-α-tocopheryl acetate/day, Evion) and vitamin C (250 mg L-ascorbic acid/day, Celin). The patients were instructed to consume vitamin E and C daily for the duration of 12 weeks (3 months). After 12 weeks of supplementation, the effect of supplements was assessed by measurement of oxidant and antioxidant markers in the patient. The patient and control were excluded for high levels of dietary supplemental, sever under or malnourishment, seizure disorders, head injury, with loss of consciousness, alcohol and substance abuse and dependence, excessive smoking, type II diabetes, lipid disorders, cardiovascular diseases, hypertension or a family history of the same. These factors and obesity, which is also rarely seen in these patients, known to affect free radicals and antioxidant status were also excluded. Diagnosis of schizophrenia was derived by structured clinical interview (SCID-P) according to axis I of DSM-IV (Diagnostic and Statistical manual of Mental Disorders- fourth edition) criteria (12). Patients with WAIS-R full scale IQ<80 were excluded. The psychopathology of status of the patient was assessed on admission and after treatment by a trained physician using PANSS (positive and negative symptoms scale) score.
The following laboratory investigation were carried out 1) Complete blood count to exclude anemia or any other abnormality. 2) Renal function tests (blood urea and serum creatinine) to exclude renal impairment. 3) Liver function tests to exclude liver affection, especially those with diminished albumin levels or high globulin levels. Biochemical assays The heparinised venous blood samples obtained from these subjects were used for the analysis. Plasma was separated by centrifugation at 3000 g for 15 minutes. Separated plasma was used for the estimation of MDA, vitamin E, vitamin C, TAC. The buffy coat was removed and the packed cells were washed three times with physiological saline. The erythrocytes suspension was prepared by the method of Dodge et. al. (13), modified by Quist (14). The packed cells were used for the analysis of SOD and GSH. SOD activity was measured in hemolysate, according to the method of Kajari Das (15). Superoxide radicals were generated by photo reduction of riboflavin. These radicals react with hydroxylamine hydrochloride to produce nitrite. The nitrite in turns reacts with sulfanilamide to produce diazonium compound, which subsequently react with N-naphthylene diamine to form a red colored azocompound whose absorbance was measured at 543nm. Erythrocyte GSH was estimated by the method of Beutler et. al. using dithio-bis- nitro benzoic acid (DTNB) (16). DTNB was reduced by sulf-hydryl compounds to an intense yellow colored complex which was measured at 412nm. Plasma vitamin E (alpha-tocopherol) was determined by the method of Baker and Frank (17). Vitamin E was measured by their reduction of ferric to ferrous ions which then forms a red colored complex with dipyridyl. Tocopherol and carotene were first extracted into xylene and absorbance was measured at 460nm to measure carotene. A correction for carotenes was made after adding ferric chloride and read at 520nm. Ascorbic acid levels were estimated in plasma by the method of Tietz (18). Ascorbic acid was oxidized to diketogulonic acid in the presence of strong acid solution. This ketogulonic acid reacts with 2,4-dinitrophenylhydrazine to form diphenylhydrazone which dissolved in sulphuric acid to produce red colored complex which measured spectrophotometrically at 520nm. Plasma MDA concentrations was determined as the measure of TBARS (19). MDA as an indicator of oxidative stress measuring it as a secondary fragmentation product of PUFA peroxide, a thiobarbituric acid reactive substance (TBARS) that gives a pink colored complex with thiobarbituric acid (TBA). It was read on a spectrophotometer (Systronic Co. Gujarat, India.) at 530nm. TAC was measured by the assay of FRAP (20). Ferric tripyridyl triazide (Fe III-TPTZ) complex was reduced to its ferrous form, which is intense blue colored complex and absorb light at 593nm. All the reagents used were of analytical reagent grade and purchased by local chemical distributors. Statistical analysis Statistical analysis between controls and patients was performed by using SPSS version 17 package (Chicago, USA). The test for normality was accomplished by the normality plots. Students„t? test was done for group comparison. The data were expressed as mean± SD. All analyses were two-tailed and used p of 0.05 or less to determine significance.
RESULTS
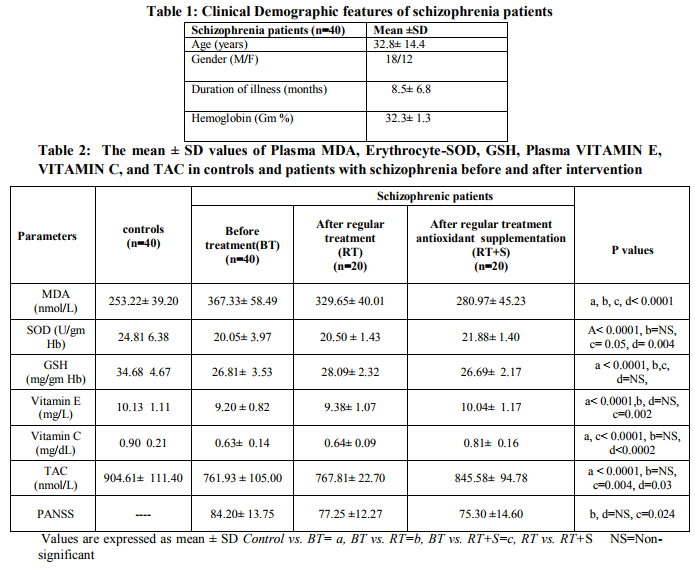
Table No. 1 shows demographic features of the schizophrenic patients. The results of the oxidative stress parameters study are illustrated in the Table 2. Significantly increased levels of MDA was seen in the patient before treatment compared to controls, whereas the levels MDA were significantly reduced after supplementation of antioxidant in the patient as compared to the patient before treatment and those taking only antipsychotics. From the results it is evident that individual antioxidant parameters like SOD, GSH, vitamin E, vitamin C etc. and total antioxidant capacity were significantly reduced in the pretreatment patients as compared to healthy controls. But the significant improvement in these parameter levels in the IInd group patients than that of Ist group patient. The results also revealed that significant improvement of clinical symptoms indicated by PANSS, in the patients receiving antioxidant supplementation as compared to patients receiving antipsychotics alone. DISCUSSION There are very few studies that the combined supplementation of vitamin E and C is effective improvement in the levels of oxidative stress parameters so as to maintain homeostasis of free radicals and antioxidants. Our results are inconsistent to the many studies the studies in the field of schizophrenia research. The use of combined supplementation of vitamin E and C is justified by few studies indicating that pathophysiology schizophrenia of involves both reduced antioxidant defense system and increased oxidative stress mediated lipid peroxidation (6, 21- 23). Few studies with supplementation with either vitamin E or C alone have reported inconsistent and variable improvement in the clinical measures. This study is also unique since it involved patients and normal controls with same racial background with similar lifestyle and dietary patterns. This suggests several ways in which ongoing oxidative stress might impact the occurrence and course of schizophrenia. Several studies have shown that alteration in the antioxidant defense system cause cognitive impairment and biochemical relevant to schizophrenia. Our study has shown highly significant increase in plasma MDA level in pre-treatment patient as compared to controls. This clearly indicates that there is increased oxidative stress mediated lipid peroxidation. Our results also reveal that the antioxidant defense system is also severely affected. A significant reduction in the SOD activity in patients, before treatment as compared to controls. The decrease in the activity of this antioxidant enzyme against lipid peroxidation due to increased oxidative stress. SOD, a chief regulator of oxidative stress, was found to be compromised with an increased oxidative stress in schizophrenia patients (23). However, there is not significant change in the SOD activity was seen in the patients receiving either regular treatment or antioxidant supplementation. The present study showed significant reduction in the erythrocyte-GSH, plasma vitamin E,C and TAC levels in schizophrenics before any treatment. The GSH deficit found in this study and previous reports indicates the role of GSH in pathophysiology of variety of neuropsychiatric disorders including schizophrenia. This may be involved in membrane peroxidation and micro lesions related to dopamine, which seem to be increased in schizophrenia, suggests that GSH may be a possible indicator of damage in neuronal membrane (24). Vitamin E is the potent lipid soluble antioxidant that stops the spread of the chain reaction in the lipid part of the cell membrane. Currently there is not enough evidence that provides the information about the supplementation with vitamin E improves symptoms of neuroleptic- induced tardive dyskinesia (9). Vitamin C is a water soluble antioxidant that scavenges reactive species. It can inhibits peroxidation of the membrane phospholipids and can also improve regeneration of vitamin E. Vitamin C is found at higher than plasma levels in a variety of tissues, including the brain (there is a greater than 10-fold gradient between the concentration of ascorbic acid in brain and serum) (1). Vitamin C is also important for maintaining levels of antioxidant vitamin E by reducing the vitamin E radical. Each antioxidant nutrient has specific activities. Yet in combination they are found to be more effective, suggesting synergistic action (25). After supplementation of these antioxidants the levels of erythrocyte-GSH, vitamin E and C, and TAC in plasma were significantly improved towards normal as compared to Ist group patients. Thus the data analysis suggested that the antioxidant vitamins particularly plasma ascorbate and vitamin E significantly contribute in reducing the oxidative stress. The previous studies, it has been found that the levels of nutrient antioxidant ascorbate and vitamin E decline as a result of the increasing oxidative stress. In the few studies a combination of both antioxidants (vitamin E and vitamin C) was used, the results showed that the dyskinetic movements total score was significantly reduced. Results of the vitamin combination are promising and further studies on this combination therapy are suggested (26). Decline in TAC is also associated with increased production of free radicals and decreased levels of antioxidant defenses. Our data regarding the TAC is consistent with the previous reports showing depletion of main antioxidants: vitamin E, C, GSH and decreased activities of antioxidant enzyme in schizophrenia (27, 28). This provides the indication that the mechanisms of free radical induced damage to lipids, proteins and DNA may be involved in the pathogenesis of schizophrenia. In the present study, we have observed that PANSS score at 12weeks improved significantly with antioxidant supplementation as compared to antipsychotics treatment. The major limitation of the present study is less sample size. Thus, further studies on larger number of patients, subgroup analysis according to age, symptoms and the duration of illness should be carried out. analyzing and comparison of the total antioxidant and total oxidant status levels among groups might have give the best results to assert the antioxidant vitamins effect and the oxidative stress involvement in the pathogenesis of the schizophrenia. CONCLUSION In conclusion, oxidative stress may be involved in schizophrenic patients and the treatment with antioxidants in the initial stage of the disease may be useful as secondary therapy to prevent the oxidative damage and deterioration of the neural tissues in schizophrenia. The results of our study have shown higher oxygen free radical production and decreased SOD activity supports the higher oxidative stress hypothesis in schizophrenic patients. It is evident from the study that increased oxidative stress in schizophrenics leads to decrease in the levels of antioxidants like GSH, vitamin E and C and disturb their metabolism, which weaken their ability to fight the growing stress.
ACKNOWLEDGEMENT
The authors are grateful to Dr. Jhalani K., Psychiatrist, and Mr. Vairal S., Jhalani hospital, Ahmednagar, for the permission and selection of the patients. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Boskvic M, Vovk T, Plesnicar BK, Grabnar I. oxidative stress in schizophrenia. Current Neuropharmacology. 2011; 9: 301-2.
2. Ng F, Berk M, Dean O, Bush A. Oxidative stress in psychiatric disorders: evidence base and therapeutic implications. I J of Neuropsychopharmacology. 2008; 11:851-76.
3. Li HC, Chen QZ, Ma Y, Zhou JF. Imbalanced free radicals and antioxidant defense systems in schizophrenia: a comparative study. J Zhejiang Univ Sci. 2006; 7:981–6.
4. Straw GM, Bigelow LB, Kirch DG. Haloperidol and reduced haloperidol concentrations and psychiatric ratings in schizophrenic patients treated with ascorbic acid. Journal of Clinical Psychopharmacology. 1989; 9:130–2.
5. Arvindakshan M, Ghate M, Ranjekar PK, Evans DR, Mahadik SP. Supplementation with a combination of omega-3 fatty acids and antioxidants (vitamins E and C) improves the outcome of schizophrenia. Schizophrenia Research. 2003; 62:195–204.
6. Dakhale GN, Khanzode SD, Khanzode SS, Saoji A. Supplementation of vitamin C with atypical antipsychotics reduces oxidative stress and improves the outcome of schizophrenia. Psychopharmacology. 2005; 182:494–8.
7. Sivrioglu EY, Kirli S, Sipahioglu D, Gursoy B, Sarandol E . The impact of omega-3 fatty acids, vitamins E and C supplementation on treatment outcome and side effects in schizophrenia patients treated with haloperidol: an open- label pilot study. Progress in Neuropsychopharmacology and Biological Psychiatry. 2007; 31:1493–9.
8. Mahadik SP, Evans D, Lal H. Oxidative stress and role of antioxidant and omega-3 essential fatty acid supplementation in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2001; 25:463-93.
9. Adler LA, Edson R, Lavori P, Peselow E, Duncan E, Rosenthal M, Rotrosen J. Longterm treatment effects of vitamin E for tardive dyskinesia. Biological Psychiatry. 1998; 43, 868–72.
10. Michael N,Sourgens H, Arolt V, Erfurth A. Severe Tardive Dyskinesia in Affective Disorders: Treatment with Vitamin E and C. Neuropsychobiology 2002; 46(Suppl.1):28-30.
11. Reddy R, Reddy R. Antioxidant therapeutics for schizophrenia. Antioxid Redox Signal. 2011; 15:2047-55.
12. American Psychiatric association. Diagnostic and statistical manual of mental disorders DSM-IV-TR 4th ed. New York: American Psychiatric Publishing Inc; 2000.
13. Dodge JF, Mitchell G, Hanahan DJ. The preparation and chemical characterization of hemoglobin free ghosts of human red blood cells. Arch Biochem Biophys. 1968; 110:119- 30.
14. Quist EH. Regulation of erythrocyte membrane shape by calcium ion. Biochem Biophys Res Commun. 1980; 92:631-7.
15. Kajari Das. A modified spectrophotometric assay of superoxide dismutase using nitrate formation by superoxide radicals. Indian J Biochem and Biophys. 2000; 57: 201-4.
16. Burtis and Ashwood. Tietz text book of clinical chemistry, 3rd ed. WB Saunders Co. 1999; pp 1652-3.
17. Baker, Frank. Determination of serum tocopherol by colorimetric method.Varley?s Practical Clinical Biochemistry, Heimann Professional Publishing, 6th edition; 1988. pp 902.
18. Caraway WT. carbohydrates in Tietz N. W. (Ed). Fundamentals of clinical chemistry. W.B. Saunder Company; 1999. pp 173-6.
19. Bird RP, Draper HH. Comparative study on different methods of MDA determination. Methods Enzymol; 1984. pp 105.
20. Benzie I, strain J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant Power”: The FRAP Assay. Analytical Biochemistry. 1996; 239: 70-6.
21. Kuloglu M, Ustundag B, Atmaca M, Canatan H, Tezcan AE, Cinkilinc N. Lipid peroxidation and antioxidant enzyme levels in patients with schizophrenia and bipolar disorder. Cell. Biochem Funct. 2002; 20:171– 5.
22. Herken H, Uz E, Ozyurt H, Sö?üt S, Virit O, Akyol O. Evidence that the activities of erythrocyte free radical scavenging enzymes and the products of lipid peroxidation are increased in different forms of schizophrenia. Mol. Psychiatry. 2001;6:66–73.
23. Dadheech G, Mishra S, Gautam S, Sharma P. Evaluation of antioxidant deficit in schizophrenia. Indian J. Psychiatry. 2008; 50:16–20.
24. Schulz JB, Lindenau J, Seyfried J, Dichgans J. Glutathione, oxidative stress and neurodegeneration. Eur J Biochem. 2000; 267:4904-11.
25. Karajibani M, Hashemi M, Montazerifar F and Dikshit M. effect of vitamin E and C supplements on antioxidant defense system in cardiovascular disease patients in Zahedan, Southeast Iran. J Nutr Sci Vitaminol. 2010; 56: 436-40.
26. Nikolaus M, Hildegard S, Volker A et al. Severe tardive dyskinesia in affective disorders: Treatment with vitamin E and C. Neuropsychobiology. 2002; 46: 28–30.
27. Altuntas I, Aksoy H, Coskun I, Caykoylu A, Akcay F. Erythrocyte superoxide dismutase and glutathione peroxidase activities, and malondialdehyde and reduced glutathione levels in schizophrenic patients. Clinical Chemistry and Laboratory Medicine. 2000; 38: 1277–81.
28. Yao JK, Reddy R, McElhinny LG, van Kammen DP. Reduced status of plasma total antioxidant capacity in schizophrenia. Schizophrenia Research. 1998a; 32:1–8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





