IJCRR - 4(18), September, 2012
Pages: 100-108
Date of Publication: 29-Sep-2012
Print Article
Download XML Download PDF
PREVALENCE OF ANAEMIA IN SCHOOL CHILDREN OF BIJAPUR, KARNATAKA
Author: Shamshad Begum .A.Loni, Irshad Ahamed, Lizzy Sunny
Category: Healthcare
Abstract:Objectives: Prevalence of anemia is high in India .Anemia is a serious health problem in Indian school children. Material and methods: Children of age group 6-15 years of Secab institution of Bijapur district of Karnataka were included in our study .Hemoglobin was determined by Salhi's method taking WHO standard .Result. Of the 1033 students included in the study, 594 were boys and 439 were girls. Overall prevalence of anemia was 67.1% with higher prevalence in girls (79.7%) as compared to boys (57.7%). The difference in prevalence was higher in the age-group >12 years (boys = 48.5%, girls = 82.5%) as compared to12 years the mild prevalence of anemia in boys was 38.21 % and moderate 12.19 %. In girls 51.68% mild and 27.3% moderate. Conclusion: Anemia is a significant problem in our apparently healthy school going children of age group 6-16 years.
Keywords: Anemia, Salhi’s method, Hemoglobin
Full Text:
INTRODUCTION
Anemia is a serious health problem in Indian school children. The nutritional status of children is a good indicator of the health status of a community1.According to Dreyfuss et al (2000)2 two billion children are affected with iron deficiency anemia worldwide. There is now need for the development of clear policy guidelines based on these simple and integrated intervention3 . Anemia is estimated to effect one half (50%) of the school age children in developing countries4 . Iron deficiency anemia affects a substantial portion of the world population pocking severe health problem to the people suffering these condition5 . Iron deficiency is probably the only nutrient deficiency of significant prevalence in virtually all developed countries 6 . Recent studies on the nutritional status of Indian children in this age group have showed prevalence ranging from 10- 60 % 7, 8, 9,10,11,12.Adolescence is defined by WHO as the period of life between 10- 19 years (WHO 1996)13 .Causes of anemia are manifold ranging from nutritional deficiencies which includes iron deficiency, which is the world’s largest nutritional problem (WHO) B12 and folate deficiency14. Dietary intake of haem iron (animal origin) is negligible in developing countries. Ascorbic acid, presence of food items of animal origin and low PH enhance while milk, coffee and tea inhibit the iron absorption. Likewise, deficiency of Vitamin A limits the body ability to use stored iron, resulting in an apparent iron deficiency because Hb levels are low even though the body stores are normal15.Daily iron requirement of children aged 6-11 years is 40ug/kg/day.14 . Many south East Asian countries including India have started iron and folic acid supplementation in target population .Indonesia has covered 60% of its target population via iron and folic acid supplementatary16 . We Indian still have not quantified anemia in our school age population .Hence our study is an attempt to estimate the magnitude of this problem of anemia in apparently healthy school children of age group 6-16 years of both sexes. The united Nation’s subcommittee on Nutrition held in Oslo in 1998 concluded that more data on health and nutrition of school age children are needed to assess their scale of problems 17 . However, recent studies have shown that the prevalence of malnutrition and anemia is high in these age group18 . The most commonly used indicator of iron deficiency anemia is Hemoglobin. But it is true that not all anemias are due to iron deficiency and not all iron deficiency will reflect in anemia
Aim of study
The present study was conducted with the object of assessing the nutritional status of children of age group 6-15 years attending school in Bijapur. And to compare Hematological Measurements with the WHO standards for that age and sex groups.
MATERIALS AND METHODS
An observational descriptive cross sectional study was conducted in apparently healthy children of age group 6-15 years in Secab Intuitions of Bijapur.
Measurements
Hemoglobin was determined by Salhi’s method. WHO standard values were considered to compare the value for those age groups and sexes. Salhi’s method of hemoglobin estimation has been used since long20 . Inspite of the availability of newer techniques which give more reliable and accurate results, this method is still in vogue 21. In our study children having Hb level 11.5 were classified as having sever, moderate, mild and no anemia respectively22 (WHO 2001). Statistical analysis – was done by statistical package for SPSS software .Mean and SD of mean was computed for each group and sex.
RESULTS
The study was carried out in apparently healthy school children of age group 6-16 years attending the schools of Secab institution of Bijapur district of South India. Relevant history was taken and completes physical examination done. Of the 1033 students included in the study, 594 were boys and 439 were girls. Overall prevalence of anemia was 67.1% with higher prevalence in girls (79.7%) as compared to boys (57.7%). The difference in prevalence between boys and girls were higher in the age-group above 12 years (boys = 48.5%, girls = 82.5%) as compared to 12 years or below 12 years (boys = 65.6%, girls = 78.0%). Further stratification of the age into smaller groups showed a highly significant difference in the mean hemoglobin levels between boys and girls in the age-group 6 to 8 years (boys = p=0.002). Among older children, the difference in the mean hemoglobin levels between boys and girls were highly significant for 13, 14, &15 years (p=0.001), In the age group of 6-15 years our study showed the prevalence of Anemia of the total children screened (N=1033), 67.1% had Hb level below the normal (12 g dl) values, indicating anemia, out of which 57.7% were boys and 79.73% were girls.
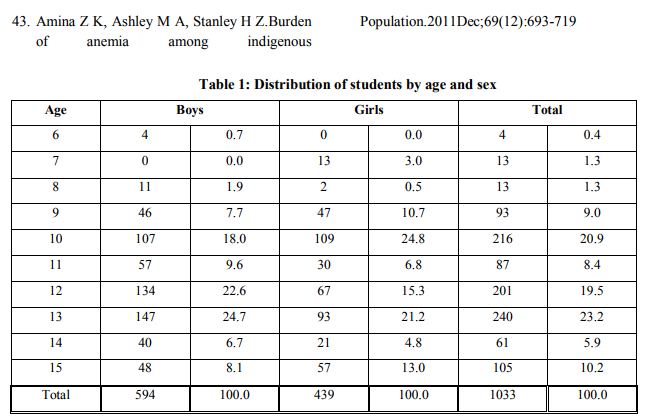
In 57.75 of anemic boys 41.07% had mild and 16.66% had moderate anemia .In girls of 79.33%, 53.07% were mild and 26.65% were moderate anemia .In age group of < 12 years we could find 30.69% mild and 25.1% moderate . In girls 12 years the mild prevalence of anemia in boys was 38.21 % and moderate 12.19 % In girls it was 51.68% mild and 27.3% moderate out of which none had severe anemia... Table 1 of our study shows the number of school going children selected. Of 1033 children 594 boys (57.7%) and 439 girls (42.5%) of age group 6-15 years. Among 6-15 years age groups children selected highest number of children was in the age group of 10 years and 12-13 years. Table 2 of our study shows the overall % of anemia in the school children. Higher Prevalence of anemia was found in girls (79.7%) as compared to boys (48.5%).Among the girls of 6-15years high prevalence of anemia was found in age group of above 12 years. When compared to below 12 years group (78%). Among the e boys higher prevalence was seen in 12 years (48.5%). The mean hemoglobin values according to the both age in both sexes are shown in table 3: The mean hemoglobin values of boys and girls aged between 13 and 15 years were highly significant The mean hemoglobin values of boys and girls at age of 6,12 were not significant . The overall mean hemoglobin values between the boys and girls were highly significant. Table 3 depict the age wise mean_+SD of Hb with P value of <0.0001 as statically significant. Higher prevalence of anemia was found in girls of age groups 9 and 14 years, and in boy of 9 years. Lowest prevalence of anemia was seen in boys of age group 15 years (18.75%). Lowest prevalence of anemia was seen in boys of age group 15 years (18.75%). Overall % of prevalence o f anemia in all age group were found to be 79.73% and boys 57.7% .Overall mild anemia in boys was 71.1% and moderate anemia 28.86%.Overall % of mild anemia in girls was 66.57% and moderate anemia was found to be 33.4%.compared to boys moderate anemia was in higher % in girls. Statically significant value was seen in age groups of 13-15 years when compared between both sexes.
DISCUSSION
It is evident from our result that significant populations of apparently healthy children suffer from anemia. There are very few data on the impact of undernutrition and anemia in school of age group of 6-15 years .The nutritional status of children is a good indicator of the health status of the community1. Apparently healthy school going children of lower and middle socioeconomic status in India are the one most neglected as far as health is concerned. Causes of anemia are manifold ranging from nutritional deficiency which includes iron deficiency, which is the world’s largest nutritional problem (WHO), B12 and folate14. The most commonly used indicator of iron deficiency is Hemoglobin. According to Stdtzfus RJ et al anemia is estimated to affect 50% of the school going children in developing countries4 . Correct estimation combined with the challenges of limited human and financial resources add to the complexity of combating iron deficiency in developing countries (WHO) 13 . Adolescent mainly girls, are especially vulnerable to iron deficiency due to low intake and absorption of iron and increased iron retirements for growth and replacement of menstrual blood loss23 .
Global prevalence of anemia among school age children is 37 % .It is 46 % in developing regions with highest in South Asia and Africa14 . Our study is an attempt to estimate the magnitude of this problem of anemia in apparently healthy school children of age 6-15 years of both sexes. According to WHO if the prevalence of anemia at community level is more than 40% it is considered as a problem of high magnitude24.The prevalence of anemia is disproportionately high in developing countries due to poverty, inadequate diet, certain diseases, pregnancy, lactation and poor access to health series25 . Recent studies on the nutritional status of Indian children in this age group have showed prevalences ranging from 10% to 60%.7, 8, and 9,10,11,12 Anemia prevalence among children of school age is 37.70 % 26 . The over result of our study indicated 67.1% of anemia in the school children of age group 6-15 years. The prevalence of anemia in girls was higher 79.7% when compared to boys 57.7%.The prevalence of anemia was higher in girls 82.5% for girls >12 years when compared with boys of same age 48.5%.Similarly in girls <12 years prevalence of anemia is 78% when compared with boys of same age group 65.6%. The results of our study corroborated the findings of Verma et al, that the prevalence of anemia in 5- 25 years of age groups of urban school children ,in Punjab was 51.5% 27 . Similarly a study stated that the prevalence of anemia in school children from urban slums aged 5-10.9 years was 41.8%28 . Similar prevalence is reported by CMS Rawat et al. 29 at Meerut. A higher prevalence was noted by J Rajaratnam et al. in Tamil Nadu30. Toteja GS et al. found 90.1% prevalence of anemia among adolescent girls from 16 districts of India, with 7.1% having severe anemia31 . Bulliyy et al. 32 found 96.5% prevalence among non school going adolescent girls in three districts of Orissa, of which, 45.2%, 46.9%, and 4.4% had mild, moderate, and severe anemia. They found significant association between Hb concentration and the educational level of girls, their parents' family income, and body mass index. One study examined 368 Orang Asli children aged 2–15 years living in eight villages in the state of Selangor and found that 41.5% were anemic (Hb < 120 g/L).33 And B.Sudhagandhi et al stated that overall prevalence of anemia in age group of 8-16 years was 52.88 %( in girls 67.7% and boys 38%)34 It was observed that 77.7% of tribal children of Mysore District, Karnataka were suffering from anemia and also indicated similar results that the prevalence of anemia was significantly higher in girls when compared to boys (girls 83.33% and boys 70.89%)35 . The overall prevalence of anemia among school going adolescent girls of urban Kathmandu, Nepal was 45.4%36 . Another study reported the prevalence of anemia of 66.4% amongst primary school children 6-11 years in national capital territory of Delhi37 . A single study in Kelaniya, Sri Lanka compared Veddah (tribal) children to Sinhalese (non-tribal) children between the ages of 6 and 15 years and found anemia (Hb < 115 g/L) was present in 67% of Veddah children compared to 36% of Sinhalese children 38 .It is evident from our results that a significant population of apparently healthy children suffers from anemia. Our result also corroborated with the study documented by Sena et al as 67.8% where in the prevalence of anemia of mild and moderate as 32.6% and 34.7% respectively and no severe anemia in this age group39 . However Zimmermann et al.40 (2003) suggested lower prevalence’s of anemia among rural school age. .Children in a mountainous region from northern Morocco was 35 per cent. The frequency of iron deficiency anemia is not uniform in the same country (Morocco) as well as in different global regions. Similar study was done by Ruchika Handa et al in the age group of 7-10 years and showed that the prevalence of anemia was 65.33%, out of which 53.33% had mild and 12% moderate and none had severe anemia.19 Our study of 67.1% was close to that of Ruchika Handa et al19 In India, the National Nutritional Anaemia Prophylaxis Programme (NNAP) has been in operation for more than 30 years, yet anemia remains a major public health problem.41 The effectiveness of daily iron-supplementation programs has been questioned because of poor efficiency of health services and lack of compliance by targeted groups42.The study by Arlappa et al in West Bengal found that none of the rural preschool children (indigenous and nonindigenous) had received the government-funded iron plus folic acid tablets, indicating that strategies and funds to improve administrative efficiency and ensure need of transparency41
Limitation of our study
Our results could have much better and accurate if the Hb estimation was done by cynometh hemoglobin method. Prevalence of various parasitic infestations and chronic illnesses were not considered. A comprehensive study including anthropometric data, biochemical data, clinical sign and dietary intake data among the children will give better insight.
CONCLUSION
In our study more than 50% were anemic and higher prevalence of anemia was found in girls compared to boys of the same age groups. This may be due to India being a developing country, poor bioavailability of dietary iron, coupled with low intake of haem iron derived from animal sources. Recommendations There is now need for the development of clear policy guidelines based on these simple and integrated intervention25.
ACKNOWLEDGEMENT
We are grateful to school children and the administrative department of Secab School Bijapur. We are acknowledging the immense help received from the scholars whose articles are cited and included in references of our manuscript. We are also grateful to authors /editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Ujjwal Chakraborty,Sutanu Dutta,Chowdhury, Goutam Dutta, Tusharkanti Gosh.A Comparative study of Physical Growth and Nutritional Status in Santal Children of Ghatsila and Bolpur.Tribes and Tribals 2008,sp:(2):79-86.
2. Dreyfuss ML, Stolt JR, Sherstha BJ, Worms H. Malaria and vitamin A deficiency contribute to anemia and iron deficiency among pregnant women in the plains of Nepal. J. Nutr. 2000; 130: 2527-2536.
3. Muthayya S,ThankachanP,Zimmermann MB, Anderson M,Eilander A,Misquith D et al.Low anemia prevalence in school aged children in Bangalore, South India: possible effect of school health initiatives;Eur J clin Nutr 2007;61(7):865-9.
4. Stoltzfus RJ, Chwaya HM, Tielsch JM, Schutze KJ, Albonico JM .Epidemiology of Iron deficiency Anemia in Zanzibari school children .Am J clin Nutr 1997; 65:153-159.
5. Jose R, Boccio and Venkatesh Iyengar .Iron deficiency causes, consequences and strategies to overcome this nutritional problem. Biological trace element research 2003; 94 (1):1-31.
6. RamakrisihnanU, Semba RD . Iron deficiency anemia.In:Semba RD,Bloem MW et al . Nutrition and Health in Developing Countries.2nd editionTotowa NJ :Human Press 2008:479- 505.
7. Mauro MB, Alves GMS, Fagundes Neto U.Nutritional Status Of Terena Indian Children from Mato indian children from Mato Grosso do Sul, Brazil: Follow up of weight and height and current prevalence of anemia Pediatr2005;81(5):383-9.
8. Lenise Mondini,Eduardo N,Cano,Ulysses Fagundes,Evandro E,Souza Lima,etal.Nutrition status in Kamaiura Indian children .Alto Xingu, Central Brazil. Rev. Bras. Epidemiol. 2007; 10 (1): 39-47.
9. Orellana JDY, CoimbraJr.CEA, Lourenço AEP, Santos RV. Nutritional Status and anemia in surui Indian Children Brazilian Amazon. J Pediatr 2006; 82 (5): 383-8.
10. Pícoli RP, Carandina L, Ribas, DLB. Hipoacusy.Prevalence in Kiowa and Guarani indigenous children .Rev.Bras.Saude Matern.Infant 2006; 22(1):69-174.
11. Lenise Mondini,DouglasA,Rodrigues, Suely GA,et al .Nutritional status and Hemoglobin values of Aurak and Ksribe Indian children – Upper Xingu, Central Brazil ,2001- 2002.Rev.vras.epidemiol;2009;12(3):469-477.
12. Mengolla A, Dracher MdeL,Rodrigues IH et al.Nutritional Status and Social determinanats of child height in the Guarila Indigenous Territory Southern Brazil .Cad Saude Publica 2006;22(2):295-405.
13. World Health Organization 1996.Programming for adolescent health and development .WHO technical report series no 886: 2.
14. DeMaeyer, EM, Dallam P, Gurney JM, Hallberg L, Sood SK, Srikanta SG. Preventing and Controlling Iron Deficiency Anemia through Primary Health Care a Guide for Health Administrators and Programme Managers. WHO, UNICEF, Switzerland. 1989: pp: 11-14 (ISBN-10: 9241542497).
15. Sturjron VEM,.Berg M,.Kruger H,Baden,JC.Mansvely,.Lawbscher AJ .Response to an iron fortification programme in relation to vitamin A status in 06-12 years old school children;Int.J Food Sci. Nutre1997;48:41-49.
16. Stunting and wasting in relation to anemia – WHO regional office for South East Asia 1996).
17. UNICEF /United Nations University World Health Organization .Iron deficiency anemia assessment, prevention and control .A guide for programme manager Document WHO/NHD/01.3Genea :World Health Organization :2001
18. Chaturvedi S, Kapil U, Gnanasekaran N, Sachdev HPS, Pandey RM, Bhanti T. Nutrient intake amongst girls belonging to poor socioeconomic group of rural area of Rajasthan. Indian Pediatr 1996 Mar; 33:197- 202.
19. Ruchika Handa ,Faizan Ahamad,Kavindra Kumar kesari, Ranu Prasad .Assessment of nutritional status of 7-10yearsschool going children of Allahabad District: A Review. Middle-East Journal of Scientific Research 2008;3(3):109-115.
20. Wintrobe MM. 'Clinical Hematology' 7th Edition. Philadelphia: Lea and Fibiger. 1975: pp 114-115.
21. Balasubramanian P, Malathi A. Comparative study of hemoglobin estimated by Drabkin's and Salhi’s methods. J Postgrad Med. 1992; 38(1):8-9.
22. WHO .Iron deficiency anemia: Assessment, Prevalence and Control: A guide for programme Managers. World Health Organization press 2001; 7-33.
23. Rajni Dhingra. An Assessment of Health Status of Adolescent Gujjar Tribal Girls of Jammu District. Stud Tribe Tribals 2011;9(2): 133-138.
24. Seshadri S, Gopaldas T.Impact of iron supplementation on cognitive functions in the preschool and school aged children: The Indian Experience .Am J Clin Nutr 1989; 50:675-86.
25. Kaur S,Deshmukh PR,Garg BS.Epidemiological correlates of Nutritional Anemia in Adolescent Girls of Rural Wardha .Indian J Community Med 2006 OctDec;31(4):255-258.
26. Kotecha PV, Nirupam S, Karkar PD.Adolescent girls’ anemia control programme, Gujarat, India. Indian J Med Res.2009Nov; 130:584-589.
27. Verma M, Chhatwal J, Kaur G.Prevalence of anemia among urban school children of Punjab. Indian Pediatr1998;35:1181-6.
28. Sunil Gomer,Bhawna ,Nishi Madan,Avtarlal ,Kusum Kela.Prevalence and etiology of nutritional anemia among school children of urban slums .Indian J Med Res 2003Oct;118:167-171.
29. Rawat CMS, Garg SK, Singh JV, Bhatnagar M, Chopra H, Bajai SK. Sociodemographic correlates of Anemia among Adolescent Girls in Rural Area of District Meerut (U.P). Indian J Community Med 2001; 26(4):173-175.
30. Rajaratnam J, Abel R, Asokan JS, Jonathan P. Prevalence of anemia among adolescent girls of rural Tamil Nadu. Indian Pediatr 2000; 37(5):532-536.
31. Toteja GS, Singh Padam, Dhillon BS, Saxena BN, Ahmed FU, Singh RPet al . Prevalence of anaemia among pregnant women and adolescent girls in 16 districts of India. Food and Nutrition Bulletin 2006; 27(4):311-315.
32. Bulliyy G, Mallick G, Sethy GS, Kar SK. Hemoglobin status of non school going adolescent girls in three districts of Orissa, India. Int J Adolesc Med Health 2007Oct-Dec; 19(4):395-406.
33. Aini UN, Al-Mekhlafi MS, Azlin M, Shaik A, Sa'iah A, Fatmah MS etal . Serum iron status in Orang Asli children living in endemic areas of soil-transmitted helminthes.Asia Pac J Clin Nutr 2007;16(4):724-30.
34. Sudhagandhi B, Sivapatham Sundaresan, Ebenezer William,.Prema A :Prevalence of anaemia in the school children of Kattankulathur,Tamil Nadu,India.International Journal of Nutrition, Pharmacology, Neurology Diseases 2011July;1(2):184-189.
35. Jai Prabhakar SC, Gangadhar MR. Prevalence of Anaemia in Jenukuruba Primitive Tribal Children of Mysore District, Karnataka .Anthropologist 2009; 11(1):49-51.
36. Tiwari K, Seshadri S.The prevalence of anemia and morbidity profile among school going adolescent girls of urban Kathmandu, Nepal .J Nep Med Assoc 2000;39:319-25.
37. Sethi V, Goindi S, Kapil U.The prevalence of anemia amongst Primary school age children (6-11 years) in national capital territory of Delhi. Indian J Pediatr 2003; 70(6):519-520.
38. Chandrasena TG, de Alwis ACD, de Silva LDR, Morel RP, de Silva NR. Intestinal Parasitoses and the nutritional status of Veddah children in Sri Lanka. Southeast Asian J Trop Med Public Health. 2004Jan;35(2):255–259.
39. Sen A, Knani SJ.Delterious Functional impact of anemia on young adolescent school girls .Indian Pediatr 2006Mar; 43(3):219-26.
40. Zimmermann M.B., Zeder C, Chaouki N, Saad A, Torresani T, Hurrell RF.Dual fortification of Salt with iodine and microencapsulated iron: A randomized, double- blind, controlled trial in Moroccan school children. Am. J. Clin. Nutr2003 Feb. 77(2):425-432.
41. Ruchika Handa, Faizan Ahamad, Kavindra Kumar Kesari , Ranu Prasad. Assessment of Nutritional Status of 7-10 Years School Going Children Of Allahabad District: A Review: Middle East Journal of Scientific Research 2008;3(3):109-115.
42. Arlappa N, Balakrishna N, Laxmaiah A, Brahmam GNV. Prevalence of anaemia among rural pre-school children of West Bengal, India. Ann Hum Biol. 2010April; 37(2):231–242.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





