IJCRR - 4(18), September, 2012
Pages: 10-23
Date of Publication: 29-Sep-2012
Print Article
Download XML Download PDF
A PROSPECTIVE RANDOMIZED CONTROL STUDY COMPARING RUBBER BAND LIGATION WITH INJECTION SCLEROTHERAPY FOR GRADE II HAEMORRHOIDS
Author: Brahadeeswaran.S, Tirou Aroul.T, Robinson Smile.S
Category: Healthcare
Abstract:Background: Various modalities of treatment for haemorrhoids were attempted but the best treatment remains unanswered despite the wide variety of treatment options in use. Although surgical haemorrhoidectomy is a more definitive procedure, it has a reputation of having a significant postoperative pain and an extended recovery time. Hence non-surgical procedures such as Rubber band ligation, injection sclerotherapy, cryotherapy, etc. are becoming popular nowadays. Aim: This prospective study to compare the results of rubber band ligation and injection sclerotherapy in grade II haemorrhoids. Methods: A Prospective cross sectional study of 60 patients attending the outpatient department of general surgery in MGMC & RI with complaints suggestive of haemorrhoids were undertaken from September 2009 to June 2011. DRE & Proctoscopy done for all these patients to identify the grade of haemorrhoids. All patients were randomized into group B (Rubber band ligation) and group S (Injection sclerotherapy) with 30 patients in each group. Procedure was performed and patients were observed immediately following the procedure and at 2 weeks, 1 month, 3 month, 6 months and 1 year. Results: In group B, it was uneventful when observed immediately with p < 0.001 where as in group S, bleeding and pain were noticed with p < 0.001 and p = 0.024 respectively. At 2 weeks follow up, pile mass was sloughed out in group B and fibrosed in group S without any significant difference. At the end of 1 year, all 30(100%) patients in group B and 26(86.7%) patients in group S were symptom free with p = 0.038.Conclusion: Thus the outcome of both Rubber band ligation and Injection sclerotherapy were the same in treating grade II haemorrhoids except for the fact that the immediate post procedure complications like bleeding and pain were significantly more in patients who had Injection sclerotherapy
Keywords: Haemorrhoids, Rubber band ligation, injection sclerotherapy, pain, bleeding.
Full Text:
INTRODUCTION
Haemorrhoid is one of the commonest surgical diseases1 . Haemorrhoids are frequently found on routine rectal examination in patients who have never had any complaints related to the disease. They are merely prolapsed mucosa with congested venous plexus. About 75% of people will have haemorrhoids at some point in their lives2 .Haemorrhoids are most common among adults ages between 45 to 653 . The terms ‘haemorrhoids’ and ‘piles’ are used quite commonly but they have entirely different meaning. The term haemorrhoid is derived from Greek which means bleeding (haima = blood: rhoos =flowing).The term pile is derived from the Latin word PILA which means ‘a ball’4 . The frequencies of II degree haemorrhoids are more common than other types. There are various modalities of managing haemorrhoids, both surgical and non- surgical such as rubber band ligation, injection sclerotherapy, cryotherapy, laser ablation, haemorrhoidectomy, stapled haemorrhoidopexy etc., Barron introduced Rubber band ligation in 1963. It has proved over the years to be the most successful, non-operative, method of treating I, II and III degree haemorrhoids. The success rate for band ligation reaches 78% of cases; the rest would need a second line of treatment5 . It has always been a relatively difficult procedure because of the equipment used. It needed two people, one to hold the Proctoscope and the operator to apply the bands using two instruments: one to draw the tissue and the other to fire the band. The instrument needed reloading of the bands after each application to each haemorrhoid. Newer instruments provided a use of suction to draw the tissue, so that the operator uses one hand to hold the proctoscope and the other to apply the suction and fire the band. The difficulty in stretching the rubber band to load the firing mechanism of the instrument continued to be a major one. The difficulty in application of rubber band resulted in introduction of other methods such as cryosurgery, laser treatment, infrared coagulation and radio frequency coagulation678 . In case of injection sclerotherapy, sclerosant is injected using Gabriel syringe or using a spinal needle over the pedicle of the pile mass. Common sclerosants used are Sodium Tetra Decyl Sulphate, 5% phenol, ethanolamine etc. The purpose of the present study is to compare rubber band ligation with injection sclerotherapy in grade II haemorrhoids in terms of resolution, recurrence and complication. AIM OF THE STUDY To compare the results of rubber band ligation and injection sclerotherapy in grade II haemorrhoids As regards. 1. Resolution 2. Recurrence 3. Complication
MATERIALS AND METHODS
- A prospective cross sectional study of 60 patients attending the general surgery OPD in Mahatma Gandhi Medical College with complaints of bleeding and mass descending per rectum were undertaken from September 2009 – June 2011
- All age groups of both sexes were included.
- DRE (Digital Rectal Examination) and proctoscopy done for all these patients to identify the grade of haemorrhoids.
- In this study group, II degree haemorrhoids were taken into account. Much attention was focussed on selecting only uncomplicated haemorrhoids.
- The inclusion and exclusion criteria are
Inclusion criteria:
Grade II haemorrhoids
Exclusion criteria:
• Grade I, III & IV haemorrhoids.
• Thrombosed haemorrhoids.
• Infected haemorrhoids.
• Associated with malignancy.
• Inflammatory diseases of bowel.
• Bleeding diathesis.
• Patient who wants to undergo surgery.
Two different time tested methods of treatment for haemorrhoids were selected for comparative study. These procedures are preferred on the basis of
- Compliance of the patient.
- Cost factor. ? Simplicity of techniques.
- Treated as OPD basis.
- Maintenance of normal anatomy as far as possible to preserve the normal anal sensation.
- Good curative rate.
- Patient was well informed about both types of treatment and was randomized by lots.
B – Rubber band ligation in grade II
S – Injection sclerotherapy in grade II
- This study was conducted after getting clearance from ethical committee.
a) Rubber band ligation
• Patient was prepared pre-operatively by glycerine enema.
• Rubber band placed in the Barron’s banding gun as shown in the figure A.


• Rectum packed with 2% lignocaine soaked gauze after the procedure. b) Injection sclerotherapy • DRE was done to assess the tone of the sphincter muscles. • 1ml of sclerosant (sodium tetra decyl sulphate) was taken in a syringe and injected over the pedicle of the pile mass using spinal needle (24G)

• Rectum packed with 2% lignocaine soaked gauze after the procedure. Patients of both groups were treated with ? T.Paracetamol 500mg x 3 days ? Laxatives: Syp. Liquid paraffin 15ml HS x 3 days & sos ? Dietary modification (High fibre diet, plenty of oral fluids)
Patients were reviewed after 2 weeks / 1 month / 3 months / 6 months / 1 year
Statistical Analysis
- Comparison of proportion by ‘CHI SQUARE’ test
- Comparison of mean value by student ‘T’ test
Study Parameters
- Age
- Sex
- Grade of haemorrhoids
- DRE & Proctoscopy findings
- Type of treatment given
- Bleeding
- Pain
- Mucous discharge
- Recurrence
- Others
OBSERVATION AND RESULTS
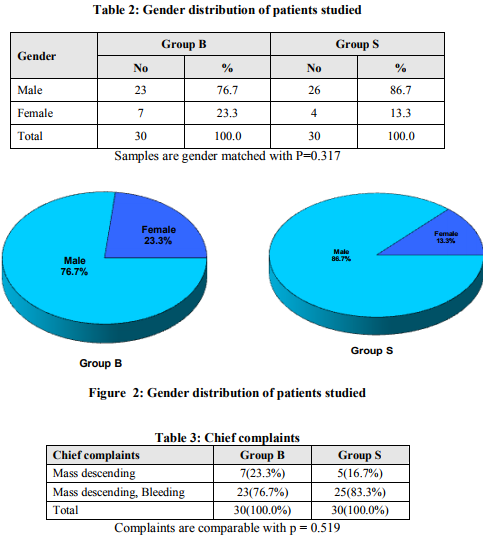
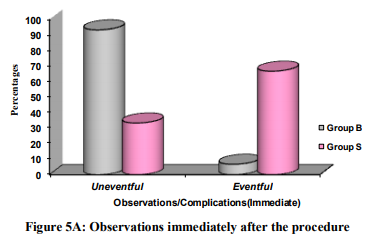
This prospective study was done to compare the results and outcome of Rubber band ligation with injection sclerotherapy in grade II haemorrhoids who presented to general surgery OPD in Mahatma Gandhi Medical College and Research Institute at puducherry. In our study, 60 patients who were diagnosed as grade II haemorrhoids were included, among them 30 patients were randomly selected in each group( B&S).The age group varied between 21 and 75 years of age with a mean of 46.27 in group B and 45.70 in group S (p =0.858) as shown in table 1 and fig 1 This study showed male predominance over female, 76.7% and 23.3% in group B, where as 86.7% and 13.3% in group S (p = 0.317) as shown in table 2 and fig 2 Among the 60 patients, 7(23.3%) patients presented with mass descending per rectum and 23 (76.7%) patients had bleeding along with mass descending per rectum as chief complaints in group B. In group S, 5(16.7%)patients presented with mass descending per rectum and 25 (83.3%)patients had bleeding along with mass descending per rectum with p = 0.519 (table 3 & fig 3) DRE revealed normal mucosa/tone in all 30 patients (100%) in group B where as in group S, 27 (90 %) patients had normal tone/mucosa and 3 patients (10 %) had sphincter spasm (table 4 &fig 4) All patients were observed immediately after the procedure and they are reviewed after 2 weeks, 1 month, 3 months, 6 months and 1 year. All patients were observed immediately after the procedure. In group B(Band Ligation), 28(93.3%) patients were comfortable in the absence of any complication with significant p < 0.001 where as in group S(Sclerotherapy), 10(33.3%) patients were comfortable. In group S, 20 (66.7%) patients had some complication with a significant p < 0.001. Out of 20 patients, 10 (33.3%) patients had bleeding with a significant p < 0.001. 6 (20%) patients had pain with a significant p = 0.024 and both in 4 (13.3%) patients with p =0.112 where as in group B, only 2(6.7%) patients had bleeding. (Table 5 & fig 5)
Follow Up
At 2 weeks of follow up, all patients were observed. Pile mass sloughed out in 29(96.7%) patients (p = 0.052) and 1(3.3%) patient had bleeding in group B. In group S, Pile mass got fibrosed in 23(76.7%) patients with p = 0.052, bleeding present in 4(13.3%) patients with p =0.195, mucous discharge present in 1(3.3%) patient and pain in 2(6.7%) patients. (Table 6& fig 6) At 1 month follow up in group B, 27(90%) were comfortable in the absence of any symptoms with significant p = 0.004. In group S, fibrosed piles mass seen in 6 (20%) patients with significant p = 0.010 and 5(16.7%) patients had bleeding with p = 0.448. 1(3.3%) had pain and one patient had recurrence with p = 1.000 as shown in table 7 and fig 7
At 3 months follow up, 30(100%) patients in group B were comfortable without any symptoms. In group S, 28(93.3%) patients were symptom free, 1(3.3%) had bleeding and one patient had recurrence with p = 1.000 (table 8 & fig 8) At 6 months follow up, 30(100%) patients in group B were comfortable without any symptoms. In group S, 28(96.6%) patients were comfortable. 1(3.4%) had recurrence with p = 1.000 and one patient had lost to follow up (table 9 & fig 9) At 1 year follow up, all patients were observed. 30(100%) patients in group B and 26(86.7%) in group S were comfortable without any symptoms with moderately significant p = 0.038.In group S, 3 (10%) patients had recurrence (p = 0.237) and 1 (3.3%) patients lost to follow up (table 10 & fig 10)
DISCUSSION
Over the years, various modalities of treatment for haemorrhoids were attempted but the best treatment remains unanswered despite the wide variety of treatment options in use. Safety is of paramount importance, especially when treating a benign disease such as haemorrhoids. 9 10 Although surgical haemorrhoidectomy is more definitive procedure, it has a reputation of having a significant postoperative pain and an extended recovery time.11 Nowadays, rubber band ligation is the most widely used procedure, and it offers the possibility to resolve haemorrhoidal disease without the need for hospitalization or anaesthesia, and with a lower incidence of complications when compared to conventional surgery.121314 Rubber band ligation can be used to treat grade I, II and III haemorrhoids and it is safe, effective and easy to use.15Other non-surgical treatment modalities include injection sclerotherapy, cryosurgery, infra-red photocoagulation, out of which injection sclerotherapy is widely used for its simplicity, cost effective and efficacy. Shamimqureshi et al conducted a study at Department of General Surgery, Jinnah Post Graduate Medical Centre at Karachi from January 2001 to May 2008. All Patients with II and III degree haemorrhoids were included in this study. In this study, haemorrhoids were more commonly found in males (74.88%) than in females (25.11%)16. In our study also males dominated with 81.6% than females with 18.4%. Patients were counselled regarding prospects of success of both the procedures. This study concluded that Rubber band ligation is a safe, effective and economical procedure for treating 2nd and 3rd degree haemorrhoids as outpatient basis which is similar to the present study in grade II haemorrhoids only. A comparative analysis was made by johnF et al regarding various non-surgical treatment such as rubber band ligation, sclerotherapy and infra-red coagulation in haemorrhoids. Rubber band ligation demonstrated a 25% difference with a response rate of banding being significantly better (p = 0.001) than sclerotherapy but the frequency of pain and bleeding are similar following both techniques17. In the present study, the response to treatment in both techniques were similar (p = 0.052) but bleeding (p < 0.001) and pain (p = 0.024) were present in patients immediately after injection sclerotherapy with a significant difference. GörgülAhmet et al conducted a study at Gazi University Faculty of Medicine at Ankara in which short-term results of rubber band ligation and injection sclerotherapy for II degree haemorrhoids are retrospectively evaluated and compared in a non-selected Turkish patient group. Thirty-four adult patients with II degree haemorrhoids are reported. All patients were supplemented by high fibre diet one week prior to the procedure. Rubber band ligation was applied to 18 patients and sclerotherapy to 16 patients. Both symptomatic status and objective healing criteria were evaluated. During a follow-up period exceeding 6 months (6-10 months), the success rate of Rubber band ligation with high-fibre diet was 88.9% (16/18), while it was 68.8% (11/16) in the Sclerotherapy group18. In our study, the success rate after one year is 100% in rubber band ligation group and 86.7% in sclerotherapy group. Both the methods in their study were free from notable complications where as in the present study, sclerotherapy group had immediate complications like bleeding (p <0.001) and pain (p = 0.024) The short-term results of this study indicate that both Rubber band ligation and Sclerotherapy performed on an outpatient basis are encouragingly effective in the treatment of II degree haemorrhoids which is similar to the present study. In a study by Savioz D et al concluded that only 55% of patients of II degree haemorrhoids were completely symptom free after treatment by Rubber band ligation19 where as in our study 30 patients (100%) were symptom free following Rubber band ligation. Wani NA et al conducted a retrospective study in evaluation of rubber band ligation as a treatment of haemorrhoids in 2009 at SMHS hospital at Srinagar, India where 50 patients were included. The results were excellent or good in 90% cases, fair in 4% and poor in 4%, with failure after completion of treatment in 2% of cases. Out of 50 cases, 49 (98%) patients had pain during procedure, on the contrary to the present study, all patients of banding group are free from pain but 6(20%) patients in sclerotherapy group had pain( p = 0.024)20 Watson et al stated in his study that application of multiple rather than single band may prove more effective in those patients for whom bleeding was the predominant symptom prior to Rubber band ligation to improve their satisfaction where as in our study, haemorrhoids were banded in single session with Barron’s method which is also equally good.21 KanellosI et al conducted a study to compare simultaneous application of sclerotherapy and rubber band ligation, with sclerotherapy and rubber band ligation applied separately for the treatment of II degree haemorrhoids between 1993 and 1996. 255 patients were involved. After a period of 4 years all patients were examined and their symptoms were recorded. They concluded that Sclerotherapy group developed significant complications after treatment compared to the other two methods (P < 0.001).Similarly our study also had significant immediate complications such as bleeding-33.3% (p < 0.001) and pain-20% (p =0.024) in sclerotherapy group than banding group.22 MacRae HM et al conducted a meta-analysis of all randomized controlled trials assessing two or more treatment modalities for symptomatic haemorrhoids. Outcome variables included response to therapy, need for further therapy, complications. A total of 18 trials were available for analysis. It is proved that Rubber band ligation was better than sclerotherapy in response to treatment for all haemorrhoids (P=0.005) with no difference in the complication rate (P=0.35) 11.Present study showed similar response to treatment in both groups with significant difference in immediate complication rate (p < 0.001) in sclerotherapy group.
CONCLUSION
The outcome of both Rubber band ligation and Injection sclerotherapy in this study were the same in treating grade II haemorrhoids except for the fact that the immediate post procedure complications like bleeding and pain were significantly more in patients who had Injection sclerotherapy.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are citied and included in references of this Manuscript. The authors are also grateful to authors/ editors/publishers of all those articles, journals and books from where the literature for this article has been review and discussed. The authors also thank all the residents and staffs in the department, Prof.N.Ananthakrishnan(PG coordinator), Dean and Vice Chancellor of MGMC & RI for their support throughout the study period without which this study would not have been possible.
References:
1. Barron J2. Office ligation of internal Haemorrhoids. Am j surg 1963; 105: 563-673.
2. Baker H, Longe JL.Haemorrhoids. Gale Encyclopedia of Medicine 2006; 3: 1766–69.
3. Chong PS, Bartolo DCC. Haemorrhoids and fissure in ano. GastroenterolClin North Am 2008; 37:627–44.
4. Bailey and Love’s Short practice of surgery – 24th edition.
5. Finninger P. Modern treatment for Internal Haemorrhoids.Br Med J 1997; 314: 1211.
6. Liebach JR, Cerda JJ. Haemorrhoids: modern treatment methods. Hosp Med 1991 Aug: 53- 68.
7. Norman DA, Newton R, Nicholas GV. Direct current electrotherapy of internal haemorrhoids: an effective, safe and painless outpatient approach.Am J Gastroenteral 1989; 84: 482.
8. Templeton JL, Spence RJ, Kennedy TL, et al. Comparison of infra-red coagulation and rubber band ligation for 1st and 2nd degree haemorrhoids.Am J Gastrenteral 1989; 84: 475-81.
9. BatL,Meltzer E, Koler M, Dreznick Z, Shemesh E.Complication of rubber band ligation of symptomatic internal haemorrhoids. Dis Colon Rectum. 1993; 36: 287-90.
10. Bleday R, Pena JP, Rothenberger DA, Goldberg SM, Buls JG. Symptomatic haemorrhoids:current incidence and complications of operative therapy. Dis Colon Rectum 1992; 35: 477-81.
11. MacRae HM, McLeod RS. Comparison of haemorrhoidal treatments: a meta-analysis. Dis colon rect 1995; 38: 687-94.
12. Shanmugam V, Thaha MA, Rabindranath KS, KL. Campbell KL, Steele RJC, Loudon MA. Systematic review of randomized trials comparing rubber band ligation with excisional haemorrhoidectomy. Br J Surg 2005; 92: 1481-7.
13. Pezzullo A, Palladino E.Rubber band ligation of haemorrhoids:Five years follow up. Min Chir 2000; 21: 253-6.
14. Longman RJ, Thomson WH. A prospective study of outcome from rubber band ligation of piles. Colorectal Dis 2006; 8: 145-8.
15. Ayman El Nakeeb, Amir Fikry et al.Rubber band ligation for 550 patients of symptomatic haemorrhoids out of 2200 patients retrospective study. Egyptian J Surg 2008 Jul; 27(3): 125-31.
16. Shamimqureshi et al. Rubber band ligation of symptomatic internal haemorrhoids; result of 450 cases. Pak J Surg 2009 Jan-Mar; 14(1): 19-22.
17. JohnF et al. A comparative analysis of non surgical treatment of haemorrhoids. Am J gasteroenterol 1992; 87(11): 1601-5.
18. GörgülAhmet et al. The results and comparison of rubber band ligation and injection sclerotherapy supplemented by highfibre diet in the treatment of second-degree internal haemorrhoids. Tur J Gasteroenterol 1999; 10(1): 66-71.
19. Savioz.D, Roche.B, Glauser.T, Dobrinov.A,Ludwig.C, Marti.M.C. Rubber band ligation of haemorrhoids: relapse as a function of time. Int J Colorectal Dis 1998; 13: 154-56.
20. Wani NA, Fazilli A, Bhat GH, Mir IS.A Retrospective Study and Evaluation of Rubber Band Ligation as a Treatment of Haemorrhoids. Ind J prac doctors 2009: 5(6).
21. Watson NFS, Liptrott S, Maxwell-Armstrong CA. A Prospective audit of early pain and patient satisfaction following outpatient band ligation of Haemorrhoids. Ann R CollSurg Engl 2006; 88:275-79.
22. Kanellos I et al.A comparison of simultaneous application of sclerotherapy and rubber band ligation, with sclerotherapy and rubber band ligation applied separately for the treatment of haemorrhoids: a prospective randomized trial. Colorectal dis 2003 Mar; 5(2): 133-8








SIGNIFICANT FIGURES
+ Suggestive significance (P value: 0.05 * Moderately significant ( P value:0.01
** Strongly significant (P value : P<0.01)
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





