IJCRR - 4(1), January, 2012
Pages: 29-33
Print Article
Download XML Download PDF
A DIFFUSE CORONARY SPASM - A VARIANT OF A VARIANT?
Author: A.Noel, B. Amirthaganesh
Category: Healthcare
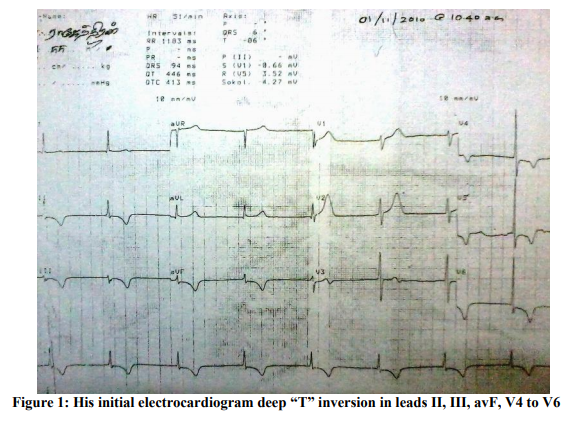
Abstract:A 55 year old mild hypertensive presented with typical angina pain associated with giddiness and profuse sweating. His initial Electrocardiogram showed „Junctional rhythm? with diffuse „T? wave changes in leads II, III, avF, V4 to V6. 2D Echocardiogram, on the same day, showed regional wall motion abnormality of Left Anterior Descending (LAD) and Left circumflex (LCX) /or Right Coronary Artery (RCA) territories with moderate Left Ventricular dysfunction. Subsequently, Coronary Angiogram done two weeks later showed normal epicardial coronaries.
Keywords: Coronary Spasm; Prinzmetal; ECG abnormalities; Regional Wall Motion Abnormality (RWMA); Acute coronary syndrome
Full Text:
INTRODUCTION
Prinzmetal variant angina has always been a medical curiosity and thought to be a rare entity, nonetheless increasing number of cases are being reported every year. It was first described as "A variant form of angina pectoris" in 1959 by the American cardiologist Dr. Malcolm Prinzmetal. [1] Prinzmetal angina most commonly affects a single site (usually the RCA) and presents as a focal spasm, which may vary for each attack (migratory spasm). [2,3] We report a 55 year old man who presented with multivessel involvement as evidenced by his Electrocardiogram and Echocardiogram findings.
Case Report
A 55 year old man was brought with history of typical anginal pain associated with giddiness and profuse sweating in the early morning hours lasting for half an hour. He was euglycemic and a non smoker diagnosed to have hypertension 6 months prior to the present hospitalization, which was well controlled on Enalapril Maleate (5mg). His lipid profile was normal and the family history was non-contributory. As he could reach the hospital only four hours later, his electrocardiogram that time showed „Junctional rhythm? at rate of 50/min with deep “T” inversion in leads II, III, avF, V4 to V6.
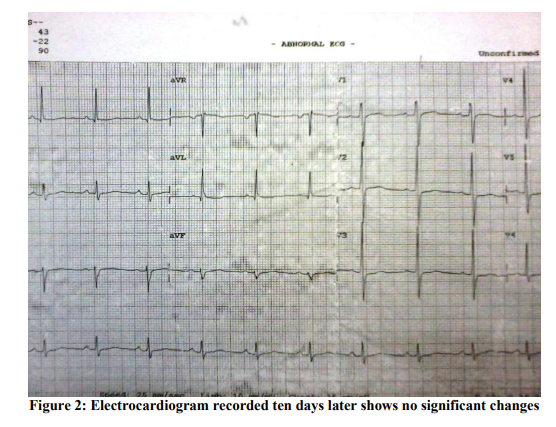
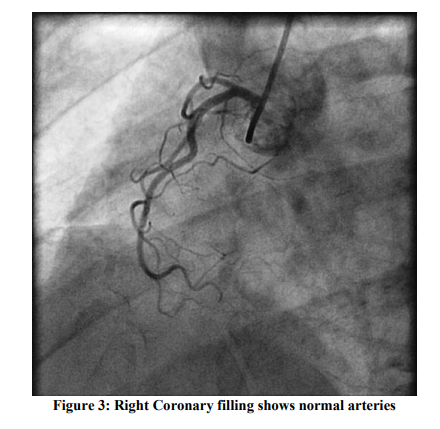
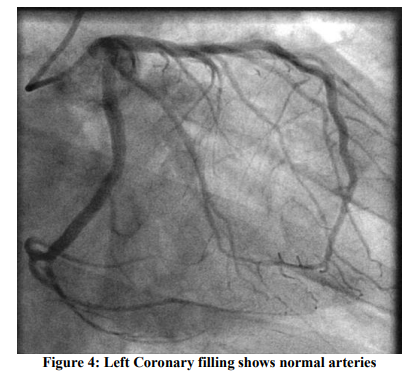
Consequent 2D Echocardiogram showed regional wall motion abnormality involving the both Left coronary artery and Left Circumflex /or Right coronary artery domains with moderate LV dysfunction (Ejection Fraction ~ 38%). A provisional diagnosis of Acute Coronary syndrome was made and was managed conservatively with low molecular weight Heparin, Statins and Anti-platelet drugs before he was referred to our hospital. On arrival at our hospital, he was totally asymptomatic, his ECG was within normal limits (Figure: 2) and his ECHO showed normal LV systolic function with no RWMA. A coronary Angiogram was done which showed normal epicardial coronaries with left dominant system (Figures: 3 and 4). Provocative tests could not be done due to ethical and safety concerns. Intra Vascular Ultra sonogram (IVUS) could not be performed on him due to lack of technical expertise and economical consideration. He was managed with Diltiazem hydrochloride 90 mg (sustained release) along with Asprin 75 mg and Rosuvastatin 10 mg. His hospital course was uneventful and there were no further angina attacks till date (on 10 months follow up).
DISCUSSION
The typical presentations of Prinzmetal?s variant angina (PVA) are: Pain at rest, not related to any physical or emotional stress [4] and associated ST segment elevation. [3, 5] Some studies say that not all ECG changes are accompanied by symptoms, sometimes there are ECG changes even in the absence of symptoms. [6] Moreover the attacks tend to have a circadian rhythm usually between 12:00 am and 8:00 am [2] and occur in clusters. They generally are not associated with any classical risk factors (except for heavy smoking). [2] They are also found to be associated with other vasospastic disorders such as Migraine and Raynaud?s Phenomena. [2,3] In our study we found that the subject had involvement of both coronary artery territories. The symptoms were present during the early morning hours and were accompanied by ECG and ECHO changes. In some cases, PVA can take a benign course without any complications but in others it can present with dreaded complications such as syncope, AV block, asystole, ventricular tachy-arrhythmias [5] or MI. [2,3] Although numerous reports are available on variant angina, very little is known about spasm involving multiple vessels. Various theories have been proposed in the pathophysiology of Prinzmetal angina such as eNOS gene mutation,[7] increased Phospholipase C activity etc.[2] Basically it is an endothelial dysfunction causing increased vasomotor tone or vasospasm and repetitive vasospasm causes injury to the vasculature, which in turn leads to coronary stenosis.[2] There are few provocative tests [1] using Ergonovine and Acetylcholine that can induce coronary vasospasm. The test induced spasm can be relieved by intracoronary nitrates or calcium antagonists. This helps in diagnosing PVA. Apart from these, 24 hours ECG monitoring can show episodic ST segment elevation, any associated arrhythmias [5] or a silent MI. [6] Exercise stress testing [4] is not very contributory. Since Prinzmetal is not a "demand" induced symptom but rather a vasospastic abnormality, it can not be induced by exercise. [3] Diagnostic hallmark of this disease has always been Angiogram; which may even be normal during an asymptomatic period. Nitrates and Calcium channel blockers (CCBs) are the mainstay of treatment for Variant angina. Nitroglycerin (in any route) effectively treats an episode of angina within minutes and CCB can be used as a prophylaxis to prevent future attacks. [8, 9] Diltiazem in particular produces coronary dilation but is a less potent peripheral vasodilator. Accordingly our patient was also started on Diltiazem hydrochloride 90 mg (sustained release) along with Asprin 75 mg and Rosuvastatin 10 mg. And there were no further anginal episodes in him at ten months follow up confirming the efficacy of the drugs on multi vessel coronary spasm. [10]
CONCLUSION
A variant of Prinzmetal Variant Angina with features of multi-vessel involvement involving normal or near normal coronary arteries, although transient and seemingly benign, can be life threatening. A multivessel presentation should not deter a physician from diagnosing a variant Prinzmetal angina because the condition can be successfully treated and prevented with Calcium channel blockers.
ACKNOWLEDGEMENT Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
1. Maile S, Moarof I, Michot M. Early morning recurrent chest pain. Cardiovascular Medicine 2011; 14(1): 24–26.
2. Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 8th ed. Philadelphia, Pa: WB Saunders; 2008. P. 1337-40.
3. Keller KB, Lemberg L. Prinzmetal’s angina. Am J Crit Care 2004; 13: 350- 354.
4. Gubbay ER. Prinzmetal’s variant angina. Can Med Assoc J 1960; 83(4): 164–166.
5. Huckell VF, McLaughlin PR, Morch JE, Wigle ED, Adelman AG. Prinzmetal's angina with documented coronaryartery spasm: Treatment and follow-up. British Heart Journal 1981; 45: 649-55.
6. Guazzi M, Fiorentini C, Polese A, and Magrini F. Continuous electrocardiographic recording in Prinzmetal's variant angina pectoris. British Heart journal 1970; 32: 611- 616.
7. Valentin Fuster, Robert O?Rouke. Hurst’s the Heart. 12th ed. McGrawHill Professional; 2007. P. 1370-72.
8. Gomez FP, De Dious RM, Rey J and Aguado G. Prinzmetal's angina: reflex cardiovascular response during episode of pain. British Heart Journal 1979; 42: 81-87.
9. Madias JE. The syndrome of variant angina culminating in acute myocardial infarction. Circulation 1979; 59:297-306
10. Harper R, Peter T, Hunt D. Syncope in association with Prinzmetal variant angina. British Heart Journal 1975; 37: 771-774.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





