IJCRR - 4(2), January, 2012
Pages: 36-42
Print Article
Download XML Download PDF
THE ASSOCIATION BETWEEN HAND GRIP STRENGTH AND HAND DIMENSIONS IN HEALTHY
INDIAN FEMALES
Author: Umama Nisar Shah, Mohamed Sherif Sirajudeen, Padma Kumar Somasekaran, Naajil Mohasin, Manjula Shantaram
Category: Healthcare
Abstract:Background: The human hand is a very complex structure and devoted to the functions of manipulation. Hand grip strength is used in clinical settings as an indicator of overall physical strength and health. Objectives: This cross-sectional study was performed to study the association between hand grip strength and anthropometric measurements (height, weight, body mass index, hand dimensions) in healthy Indian female population. Methods and Measures: A
total of 50 healthy female subjects, satisfying the selection criteria were recruited in the study. Subjects were then assessed for height, weight, body mass index (BMI), hand and forearm anthropometric measurements. The grip strength of both dominant and non-dominant hands were measured using Jamar dynamometer. Measurements followed standardized procedures and instructions. Statistical analysis: The data was analyzed by Pearson's correlation coefficients and 5% level of probability was used to indicate statistical significance. Results: In females, dominant and non-dominant grip strength have significant positive correlation (p< 0.05 - 0.001) with height (r = 0.572, 0.570), weight (r = 0.404, 0.411), hand length(r = 0.39, 0.40), hand span (r = 0.44, 0.46), wrist circumference(r = 0.37, 0.31) and forearm girth (r = 0.39, 0.35). Conclusion: The results show that height, weight, hand length, hand span, wrist circumference and forearm girth positively correlate with hand grip strength. Hand grip strength is not associated with BMI and hand breadth in healthy Indian females.
Keywords: Hand grip strength, Jamar dynamometer, anthropometric measurements
Full Text:
INTRODUCTION
The human hand is a very complex structure and devoted to the functions of manipulation. It is also capable of relaying sensory information about temperature, shape and texture of the object to the brain1 . Its effectiveness is due to the ability to perform firm grip, together with highly elaborated nervous control and sensitivity of fingers2 . Full function and adequate strength of hand are necessary for dealing with demands of daily life. Hand grip strength is used in clinical settings as an indicator of overall physical strength and health3 . Hand strength has been identified as an important factor predicting disability in musculoskeletal diseases 4 , bone mineral density 5,6, and the likelihood of falls and fractures in osteoporosis 7,8.It even predicts complications and general morbidity after surgical interventions 9 ,general disability and future outcome in older age 10-1 Hand grip strength can be quantified by measuring the amount of static force that the hand can squeeze around a dynamometer. The force has most commonly been measured in kilograms and pounds13 . The Jamar dynamometer has been found to give the most accurate and acceptable measures of grip strength14 . Anthropometric data is very useful in designing functions concerning with human. Without such data, the designs cannot fit the people who are going to use them. Therefore the information regarding the human sizes is essential to be implemented in the design of various facilities. Hand dimensions (anthropometry) is very important and used in designing objects dealing with human hands15 . Hand grip strength is positively correlated to height, weight, body mass index (BMI) and hand anthropometric measurements in healthy Indian men16. The information regarding hand grip strength and anthropometric measurements of healthy women is scanty from India. Since women are the most important source of work force in India, their hand grip strength and anthropometric data are essential in the implements from ergonomic considerations. Keeping these factors in view, a study has been undertaken to generate hand grip strength and anthropometric data of normal adult Indian women and to determine whether these parameters are associated.
MATERIALS AND METHODS
This was a cross-sectional descriptive study and was conducted in post graduate research laboratory at Yenepoya University, Mangalore, Karnataka. Approval was taken from Yenepoya University Ethical Committee prior to the commencement of the study. The data was collected from 50 healthy adult females of age group 20-80 years. Informed consent was obtained from all subjects prior to data collection. The inclusion criteria in the study was that subjects should be healthy. Subjects were excluded if they reported any neurological or musculoskeletal impairment of upperlimbs, cardiovascular or systemic illness.
Procedure
Healthy females were assessed for the - height (cm), weight (kg), body mass index (BMI) as recommended by World Health Organization (WHO).
Hand dimensions: The precision of the measures was 0.5 cm. The hand length, hand breadth, hand span, wrist circumference and forearm girth measurements were therefore rounded to the nearest whole centimeter.
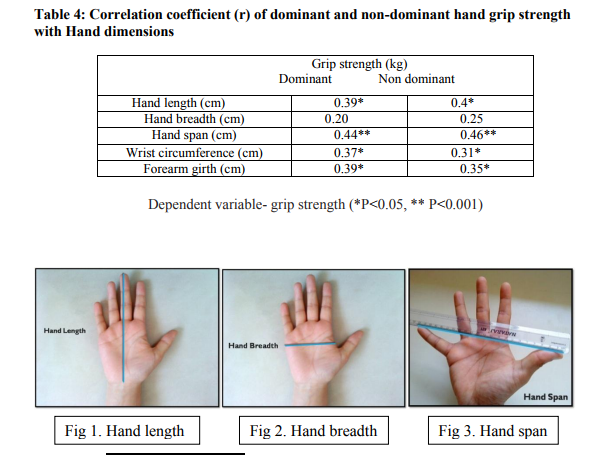
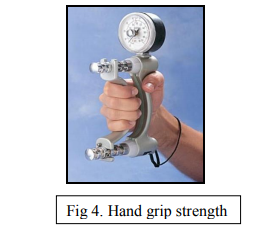
Measurement of Hand length: Measurements of the hand length was taken in both hands (perpendicular distance) from the tip of the middle finger to the distal wrist crease 17,18 (figure 1) Hand breadth Measurement: Measurements of the hand breadth was taken in both hands from the radial side of metacarpal D2 (index finger) to ulnar side of metacarpal D5 (small finger)17,18 as shown in figure 2. Measurement of hand span: Hand span was measured in both hands from the tip of the thumb to the tip of the small finger with the hand opened as wide as possible19 (figure 3). Wrist circumference: Measurement of the wrist circumference was taken for both sides around distal wrist flexion crease20 . Forearm girth: Measurement of the forearm girth for both sides was taken around the maximum girth immediately distal to the elbow with arm extended in front of the body and palm up21 . Handgrip strength was measured using a Jamar dynamometer (figure 4). Grip strength is tested by placing the subject in seated position with his arm side, elbow flexed 90°, forearm in mid-prone position, wrist extended between 0°- 30° and ulnarly deviated 15°. The subject alternatively grips the dynamometer with his dominant and non-dominant hands, performing 3 trials, using different grip spans in random order, allowing a 1-minute rest between the measurements22-24. The reported precision of the device was 0.1 kg. For each measure, the hand to be tested first was chosen randomly. For Jamar dynamometer the grip span equivalence for the different positions are as follows: position 1 - 3.5 cm; position 2 - 4.8 cm; position 3 - 6.0 cm; position 4 - 7.3 cm; and position 5 - 8.6 cm.
Statistical analysis Pearson‘s correlation coefficients were applied to establish the correlations of dominant and non-dominant hand grip strength with height, weight BMI and hand anthropometric measurements. A 5% level of probability was used to indicate statistical significance.
RESULTS
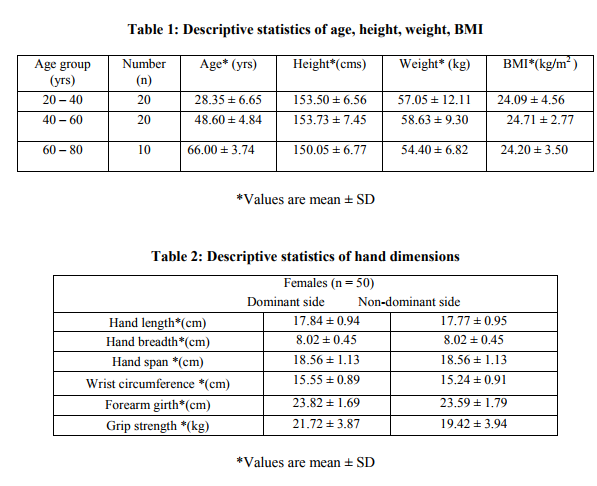
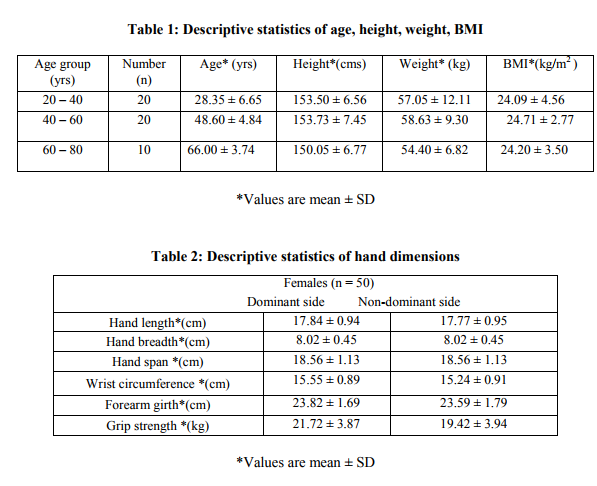
In table 1, descriptive statistics of age, height, weight and BMI of the subjects is depicted. The data regarding hand anthropometric measurements and grip strength are given in table 2. The dominant and non-dominant grip strength have significant positive correlation (p<0.05 - 0.001) with height(r = 0.572,0.570) and weight(r = 0.404,0.411), but not correlated with BMI as shown in table 3. The dominant and non-dominant grip strength have significant positive correlation (p<0.05 - 0.001) with hand length(r =0.39,0.40), hand span(r= 0.44, 0.46), wrist circumference (r = 0.37,0.31) and forearm girth(r = 0.39,0.35), but not correlated with hand breadth (r= 0.20,0-25) as illustrated in table 4.
DISCUSSION
The evaluation of grip strength is of paramount importance in hand rehabilitation. It assesses the patient‘s initial limitation and provides a quick reassessment of patient‘s progress throughout the treatment. In our study 50 healthy Indian adult females were evaluated for grip strength using jamar dynamometer. The mean dominant and nondominant grip strength was observed to be 21.72kg and 19.42kg respectively. The dominant grip strength is stronger than that of the nondominant side and this finding agree with results of Bansal25. Grip strength is influenced by factors like age, synergistic muscle action, state of nutrition, cooperation of patient, restricted range of motion, pain and sensory loss26 . This study investigated the correlation between grip strength and anthropometric variables like height, weight, BMI, and hand dimensions (hand length, hand breadth, hand span, wrist cicumference and forearm girth) in both dominant and non dominant sides. The findings of the study indicates that both dominant and nondominant grip strength positively correlates with all the anthropometric variables except BMI and hand breadth of the respective sides. This finding partially supports and partially contrasts with the findings of Koley etal27, where in dominant right hand grip strength strongly associated with hand length, hand width, forearm girth and was not associated with height, weight and BMI in 18-25 years aged healthy Indian collegiate females. Both dominant and nondominant grip strength positively correlates with the wrist circumference. This finding is in agreement with that of Ramakrishnan etal28, where in wrist circumference has a reasonably good correlation with nondominant hand grip strength in both males and females.
LIMITATIONS AND FUTURE SCOPE
Due to small sample size and the type of population used, these results cannot be reflected to the entire population of India. The use of electronic dynamometers should also be considered since this might reduce limitations of the measurements performed with the hydraulic dynamometer mainly due to deviation of wrist position from the optimum one. Various studies which have been reported showed significant differences between rural and industrial communities regarding handgrip strength. Our subjects in this study were from rural setting, so future research should also take urban population into consideration.
CONCLUSION
There are important findings to consider from this study on healthy Indian women. The first finding was that the dominant grip strength is stronger than that of the nondominant side. The second major finding was a clear association between hand grip strength (both dominant and nondominant side) and height, weight, hand length, hand span ,wrist circumference and forearm girth of the respective sides. The last finding was that grip strength was not associated with BMI and hand breadth in both sides. Based on the results of our study, as well as those previously published data on hand grip strength, an international effort for the establishment of coefficients for grip strength evaluation should be the future target. These coefficients should incorporate anthropometric measurements such as height, weight and hand dimensions in order to evaluate the optimal normal grip strength for the postoperative or the post-traumatic hand based on hand dominance and on grip strength of the contra-lateral side.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. BlairVA. Hand function. In: Durward BR, Baer GD, Rowe PJ, eds. Functional Human Movement. Oxford: Butterworth-Heinemann; 2002. p. 160- 79.
2. Markze MW. Origin of the human hand. Am J Phys Anthropol.1971; 34: 61-84.
3. Nicolay CW, Walker AL. Grip strength and endurance: Influences of anthropometric variation, hand dominance and gender. International journal of industrial ergonomics.2005;35:605-618.
4. Oken O, Batur G, Gündüz R, Yorganciogly RZ. Factors associated with functional disability in patients with rheumatoid arthritis. Rheumatol Int. 2008; 29(2):163-166.
5. Barnekow-Bergkvist M, Hedberg G, PettersSon U, Lorentzon R. Relationships between physical activity and physical capacity in adolescent females and bone mass in adulthood. Scand J Med Sci Sports. 2006; 16(6):447-455.
6. Di Monaco M, Di Monaco R, Manca M, Cavanna A. Handgrip strength is an independent predictor of distal radius bone mineral density in postmenopausal women. Clin Rheumatol .2000; 19(6):473-476.
7. Sirola J, Rikkonen T, Tuppurainen M, Jurvelin JS, Alhava E, Kröger H. Grip strength may facilitate fracture prediction in perimenopausal women with normal BMD: a 15-year population-based study. Calcif Tissue Int .2008; 83(2):93-100.
8. Ensrud KE, Ewing SK, Taylor BC, Fink HA, Cawthon PM, Stone KL, Hillier TA, Cauley JA, Hochberg MC, Rodondi N, Tracy JK, Cummings SR. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch Int Med .2008; 168(4):382-389.
9. Mahalakshmi VN, Ananthakrishnan N, Kate V, Sahai S, Trakroo M. Handgrip strength and endurance training as a predictor of postoperative morbidity in surgical patients: can it serve as a simple bedside test? Int Surg. 2004; 98(2):115-121.
10. Al Snih S, Markides KS, Ottenbacher KJ, Raji MA. Hand grip strength and incident ADL disability in elderly Mexican Americans over a seven-year period. Aging Clin Exp Res. 2004; 16(6):481-486.
11. Rantanen T, Guralnik JM, Foley D, Masaki K, Leveille S, Curb JD, White L. Midlife hand grip strength as a predictor of old age disability. JAMA.1999; 281(6):558-560.
12. Bohannon RW. Hand-grip dynamometry predicts future outcomes in aging adults. J Geriatr Phys Ther .2008; 31(1):3-10.
13. Massy-Westropp, Gill TK, Taylor AW, Bohannon RW, Hill CL. Hand Grip Strength: age and gender stratified normative data in a population-based study. BMC Research Notes. 2011;4:127.
14. Mathiowetz V, Weber K, Volland G, Kashman N. Reliability and validity of grip and pinch strength evaluations. J Hand Surg. 1984 ;9:222–226.
15. Saengchaiya N, Bunterngchit Y. Hand Anthropometry of Thai Female Industrial Workers. The journal of KMITNB. 2004;14(1):16-19.
16. Sirajudeen MS, Shah UN, Somasekaran PK, Shantaram M. Correlation between grip strength and physical factors in men. Journal of advanced researches in biological sciences. Forthcoming 2012.
17. Vianna, LauroC, Oliveira, Ricardo B, Araujo B, Claudio GS. Age-Related Decline in Handgrip Strength Differs According To Gender, Journal of Strength and Conditioning Research. 2007; 21(4): 1310-1314.
18. Jurimae T. Hurbo T ,Jurimae J .Relationship of handgrip strength with anthropometric and body composition variables in prepubertal children . Journal of Comparative Human Biology.2009; 60(3): 225-238.
19. Ruiz-Ruiz J, Mesa JL, Gutiérrez A, Castillo MJ. Hand size influences optimal grip span in women but not in men. J Hand Surg 2002;27: 897–901.
20. Myers RS. Suanders manual of physical therapy practice. Saunders company.1995.
21. Katch VL,McArdle WD, Katch FI. Essentials of exercise physiology. LWW.1995.
22. Smith P. Lister‘s The Hand. Churchill livingstone. 2002.
23. Hunter JM, Mackin EJ, Callahan AD. Rehabilitation of the hand: Surgery and therapy. Missouri: Mosby 1995.
24. Fess EE: Grip strength. In Clinical assessment recommendations.. 2 edition. Edited by: Casanova JS. Chicago: American Society of Hand Therapists;1992:41-45
25. Bansal N. Hand grip strength: Normative data for young adults. Indian journal of Physiotherapy and Occupationaltherapy.2008;2(2):29-33.
26. Incel NA, Ceceli E, Durukan PB, Erdem HR, Yorgancioglu ZR. Grip Strength: Effect of Hand Dominance. Singapore Med J. 2002;43(5) : 234- 237.
27. Koley S, Singh AP. An Association of Dominant Hand Grip Strength with Some Anthropometric Variables in Indian Collegiate Population. Anthropologischer Anzeiger. 2009;67(1):21-28.
28. Ramakrishnan B, Bronkema LA, Hallbeck MS. Effects of Grip Span, Wrist Position, Hand and Gender on Grip Strength. Proceedings of the Human Factors and Ergonomics Society Annual Meeting. 1994;38(1):10554-558.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





