IJCRR - 4(3), February, 2012
Pages: 53-58
Print Article
Download XML Download PDF
A REVIEW ON M-HEALTH SYSTEM AND TECHNOLOGIES
Author: Arvind Rehalia, Rajat Kumar
Category: Technology
Abstract:Rapid advances and developments in information technology and telecommunication have brought in picture a promising technology, called mhealth, for delivery of health-care facilities via mobile communication technologies. For accelerating the potential of mhealth, it is important to carefully study the barriers and gaps in policies and collaboration between governments and health-care institutions. This paper presents a detailed analysis of current and emerging trends in mobile health, with particular emphasis on case studies.
Keywords: Child-Count, Colecta-Palm, Mobile Midwife, mhealth.
Full Text:
INTRODUCTION
In 1983, the DynaTAC 8000X was the first mobile phone to be commercially available. From then onwards, mobile technologies have grown many-folds with an initial start from telephony systems to the modern systems that support a large array of services like text messaging, email, gaming, photography, internet access, short range wireless communication etc. Mobile phones have successfully bridged the the digital divide among different sections of developing economies and have reached the bottom of the economic pyramid. No other innovation has ever provided such parallel and distinct opportunities for instant communication and thus the utilization of potential of such a technology for health-care facilities has become important and obvious. Mhealth refers to the delivery of health care facilities supported by mobile devices using cellular, blue-tooth or wireless networks. The field of mhealth has emerged in the last decade or so and has put in place various applications of health-care service delivery for remote monitoring, emergency telemedicine, telematics, tele-radiology, education, awareness and other direct provisions of care. In recent years, several mhealth technologies have been implemented all across the globe under various research and health-care projects. The objective of the current paper is to present a review on mhealth systems and technologies. This paper has been divided into different independent sections and provides analysis of the concerned section accordingly. Next section presents a brief overview of current mobile communication technologies and their future design and considerations. After that a section on overview of related work done through published conference and journal papers has been placed. Next, a section on case studies has been presented and finally the paper wraps up with concluding remarks.
CURRENT MOBILE TECHNOLOGIES
This section describes the main wireless technologies used in mhealth systems and their future designs and considerations. SMS functions and real-time voice communication collectively forms the backbone of cellular communication. However with the development of technologies like that of smart phones and PDAs, the scope of mhealth is not just limited to cellular network integration. GSM is the current technology in use and was developed by European Telecommunications Standards Institute under the secondgeneration (2G) technologies. GSM operates under a carrier frequency range of 900 MHz to 1800 MHz with a limited data transfer rate of 9.6 Kbit/s. However, in recent years 2.5G (iDEN, GPRS, EDGE) and 3G ( TD-CDMA, W-CDMA, CDMA) technologies have evolved having higher data transfer rates as compared to GSM. Apart from GSM and 3G systems, Wireless Local Area Network (WLAN) and satellite systems also provide a means for data transfer for mhealth systems. The satellite systems provide global coverage and can operate under various frequencies and data transfer rates. WLAN links two or more devices using speed spectrum or OFDM radio methodology and provide data connectivity with user mobility (roaming unit). After a detailed analysis, the following limitations were observed in the current mobile communication technologies:
1. High cost of Communication Links and Infrastructure.
2. Limited bandwidth and data transfer rate.
3. Lack of network reliability of cellular networks.
4. Security challenges during data transfer.
5. Absence of guidelines for cellular phones to be used as imaging device.
The next generation mobile technologies must eliminate the limitations of the current system and on the other hand it should seamlessly integrate the current technologies for a better and advanced design. It is expected that the 4G technology will incorporate the fundamentals that will ensure costeffectiveness and high data transfer rates. The LTE Advanced technology (4G) promises to provide download speeds up-to 1Gbit/s and 100Mbit/s to mobile users. Further, the 4G will be based on iPv6. Considering the continuous improvements, it is almost certain that the ability of mhealth will grow many times as with larger bandwidths and faster data transfer rates, good imaging will become possible.
RELATED WORK
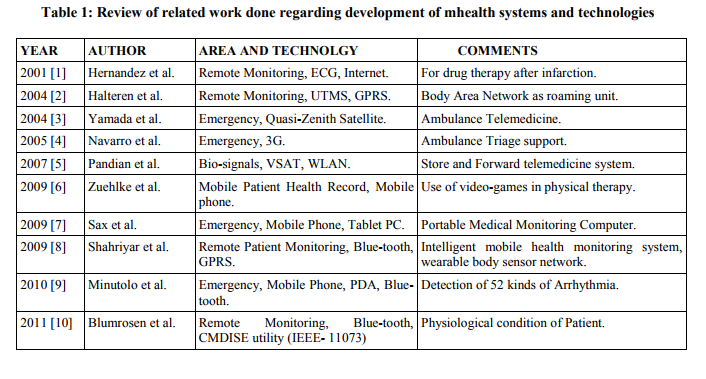
This section reports the related work done by research community all across the globe for development of an effective system for implementation of mhealth for health-care service delivery. Different databases like IEEE, INSPEC etc. were searched and finally a total of ten research papers published in various journals and conference proceedings were selected on the basis of the technologies involved and the area of application. The work listed table 1 provides a snapshot of implementation and integration of different technologies for health-care service delivery by mhealth concept. It was found that the current topic of focus among biomedical researchers is about development of systems for remote patient monitoring and wireless BODY AREA NETWORK. Further, there has been a continuous work going on for improving and integrating ambulatory emergency services and mhealth for better care of patient. Table 1, clearly suggests that mhealth is now not just confined to cellular network technologies and other technologies like ZigBee, Blue-tooth, satellite etc. have also stepped in as other communication network technologies for the development of mhealth systems.
CASE STUDIES A total of five case studies based on different areas of application of mhealth along with results, findings and other necessary details are presented here in this section. They are as under:
1. REAL TIME BIOSURVEILLANCE PROGRAM [11]:
AREA OF APPLICATION : Disease and Epidemic Outbreak Surveillance. Description : This program was started in India and Sri-Lanka with an objective to study and analyze mhealth systems for improving early detection and notification system for disease and epidemic outbreak. Under this program, 29 front line health workers in India and 16 in Sri-Lanka were chosen for digitizing the current paper based system of forms and patient health records by using mobile phones. The mobile phones were equipped with a customized application, called mhealthSurvey, developed jointly by IIT Madras and Rural Technology and Business Incubator. 4 primary health centres and 25 health sub-centres located in Tamil Nadu in India and 17 hospitals and clinics all across the country in Sri-Lanka were selected for implementation. Front line health workers digitized the patient's data at health centres and transferred them to central server. A statistical data analysis software developed by AUSTON LAB at Carnegie Mellon University was used for analysis at central server and results were sent to regional and local health officials through mobile and other communication technologies for issue of notification, if required.
RESULTS AND FINDINGS 1. It was observed that in India about 86% of the data was submitted in other-time and only 14% data in real-time. This suggests that the health workers faced difficulty in real-time submissions, mainly, due to high frequency of visiting patients. On the other hand, in SriLanka around 70% of the data was submitted in real-time. 2. Indian health workers were almost accurate in data submissions and 100% accurate in the last four weeks of the program. However, there was very large amount of errors in submissions made by SriLankan health workers. 3. It was observed that in Sri-Lanka front line health workers were aged 18-35 and were able to complete the whole process easily. However, in India front line health workers aging 30-50, even many of them with experience of 10 years or more were unable to complete the process without guidance. This suggests that younger generation is more adaptive to newer technologies than the older ones.
2. COLECTA-PALM [12]: AREA OF APPLICATION : Patient Monitoring and Support. Description : This project was started in Peru under the initiative of University of Washington and Universidad Peruana Cayetano Heredia Lima. Collecta-Palm is a web based application delivered on PDAs to HIV/AIDS patients for antiretroviral treatment and reducing transmission by safer sex behavior. This application uses intranet based secure connection for transfer of web surveys to HIV/AIDS patients. A research analysis on 15 people with HIV/AIDS (PWLHA) in two clinics in LIMA was carried out. RESULTS AND FINDINGS : Nine out of fifteen patients were satisfied with this technology and rated 3.7/5. They found this system easy-to-use, private and innovative.
3. CHILD-COUNT [13]: AREA OF APPLICATION : Point-of-care Support and Diagnosis. Description : This program was started in July 2009 in Sauri, Kenya under the partnership of Millennium Villages Project, The Earth Institute at Columbia University, UNICEF Innovation Group, Sony Ericsson and Zain. Under this project, more than 9500 children under five years of age were monitored for community based management of acute malnutrition by measuring a child's mid upper arm circumference, home based testing of malaria and home based treatment of children with diarrheal illness using ORS and Zinc supplements. The implementation was done by using a mobile application based on RapidSMS ( a free open-source framework for data collection, logistics and communication using SMS technology ) by 100 community health workers. They used SMS messages to register a patient with all the necessary details and demographics.
RESULTS AND FINDINGS 1. Initially duplicate child registrations made problems, however, changes made to the registration algorithm later solved out this issue. 2. It was found that community health workers required additional training for efficient use of the system. 3. It was found that about 10% of the total registration messages sent by the community health workers were rejected due to improper formatting by them. 4. Many of the phones went missing or needed replacement, thus adding to the overall cost of the project.
4. m-MONEY FOR WOMEN WITH FISTULA [14] : AREA OF APPLICATION : Health Financing Description : This project was started in Kenya as a combination of mobile banking, public information and free treatment. In Kenya, money transfers through mobile phones (Safaricom), constitute about 11% of GDP. Also, in a statistical survey, called msurvey, about 42% of the respondents didn't have access to formal bank accounts but use their mobile phone for financial transactions. Considering the potential of mobile banking in Kenya, this project was started to address the problems faced by poor rural women in fistula repair services. The cost of transportation to a fistula unit and lack of information about treatment options are the main problems of the concern. Under this project, a women can call a free hot-line to aquire information about fistula repair and if money is needed by women for transportation to a fistula unit, financial transfers are made via M-PESA ( a mobile banking product of Vodafone).
5. MOBILE MIDWIFE [15] : AREA OF APPLICATION : Health Education and Awareness. Description : This project was started in east Ghana, under the program, called, Mobile Technology For Community Health (MOTECH). This initiative is a result of partnership among Ghana Health Service, Grameen Foundation and Columbia University's Mailman School Of Public Health and is funded by Bill and Melinda Gates Foundation. The objective of this project is to improve the antenatal and neonatal care of rural women. In this community health workers, register the patient using MOTECH forms on mobile phones and issue a particular patient ID number. The patient then receives voice or text messages regularly regarding health information and information on essential vaccination and childhood diseases after the birth. In case a patient has a query, then she can clarify that by making a call citing reference to her patient ID.
CONCLUSION The current paper provided a brief overview of mhealth systems and technologies. The case studies clearly suggest the need for development of low cost ,secure and effective solutions for successful implementation of mhealth. Education and awareness about new technologies among community health workers is important and organizational changes should be incorporated for a better future of the telemedicine industry. While much research and development still needs to be done, the mhealth technology has already started making its impact and the future will definitely witness a revolutionized health system that will benefit the citizen and the society as a whole.
ACKNOWLEDGEMENT Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of the manuscript. Authors are also grateful to author/editor/publisher of all those articles/journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Hernandez A.I, Mora F, Villegas G, Passariello G, Carrault G. Real-time ECG Transmission via Internet for nonclinical applications. Proceedings of IEEE Transactions on Information Technology in Biomedicine. 2011 Sept; p. 253-57.
2. Aart Van Halteren, Richard Bults, Katarzyna Wac, Dimitri Konstantas, Ing Widya, Nicolay Dokovsky et al. Mobile Patient Monitoring: The Mobihealth System. The Journal of Information Technology in Health Care. 2004; 2(5): 365-73.
3. Yoshiko Yamada, Usui S, Kohn M, Mukai M. A vision of Ambulance Telemedicine Services using the Quasi-Zenith Satellite. Proceedings of 6 th International Workshop on Enterprise, Networking and Computing in Health-care Industry, HealthCom 2004. 2004 June 28-29; p. 161-65.
4. Eduardo A. Viruete Navarro, Jose Ruiz Mas, Julian Fernanadez Navajas, Cristina Pena Alcega. Enhanced 3G- Based mhealth System. Proceedings of the International Conference on Computer as a Tool, Eurocon 2005. 2005 Nov. 21-24; p. 1332- 35.
5. Pandian P.S, Safeer K.P, Shakunthala D.J, Parvati Gopal , Padkai V.C. Interent Protocol based store and forward wireless telemedicine system for VSAT and WLAN. Proceedings of International Conference on Signal Processing, Communication and Networking. 2007 Feb. 22-24; p. 54-8.
6. Zuehlke P, Li J, Talaei-Khoei A, Ray P. A Functional Specification for mobile ehealth (mhealth) Systems. Proceedings of 11th International Conference on e-health Networking, Application and Service. Dec. 16-18; p. 74-8.
7. Christian Sax, Elaine Lawrence. Point-oftreatment: Touchable E-nursing user Interface for Medical Emergencies. Proceedings of Third International Conference on Mobile Ubiquitous Computing, Systems, Services and Technologies. 2009; p. 89-95.
8. Rifat Shahriyar, Md. Faizal Bauri, Gaurab Kundu, Sheikh Iqbal Ahamed, Md. Mostafa Akbar. Intelligent Mobile Health Monitoring System (IMHMS). International Journal of Control and Automation. 2009 Sept; 2(3): 13-28.
9. Minutolo A, Sannino G, Esposito M, Depietro G. A rule-Based mhealth System for Cardiac Monitoring. Proceedings of IEEE EMBS conference on Biomedical Engineering and Sciences. 2010 Nov. 30- Dec 2; p. 144-49.
10. Blumrosen G, Avisdris N, Kupfer R, Rubinsky B. C-SMART: Efficient Seamless Cellular Phone Based Patient Monitoring System. Proceedings of IEEE IREHSS 2011: Third International Workshop on Interdisciplinary Research on E-health Services and Systems. 2011 June 22-25.
11. Gordon A. Gow, Nuwan Waidyanathan. Using Mobile Phones in Real-time Biosurveillance Program: Lessons from the front lines in Sri-Lanka and India. Proceedings of International Symposium on Technology and Society (IEEE). 2010 June 7-9; p. 366-74.
12. Walter H. Curioso, Ann E. Kurth, Robinson Cabello, Patricia Segura, Donna L. Berry. Usability Evaluation Of Personal Digital Assistants (PDAs) to support HIV Treatment Adherence and Safer Sex Behavior in Peru. Proceedings of AIMA 2008 Symposium. 2008; p. 918.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





