IJCRR - 8(18), September, 2016
Pages: 36-39
Date of Publication: 21-Sep-2016
Print Article
Download XML Download PDF
BROAD SPECTRUM ANALYSIS OF URINARY CRYSTALS: A CLINICOPATHOLOGICAL AND MICROBIOLOGICAL STUDY
Author: G. Bhuvaneshwari, Sonti Sulochana
Category: Healthcare
Abstract:Aim: The aim of this study is to evaluate the association between urinary crystal and urinary tract infection (UTI) in patients attending Saveetha Medical College and Hospital.
Method: A cross-sectional study was conducted with 1500 urine specimens. A total of 1500 urine specimens received to microbiology and pathology laboratory were included in the study. Urine with crystals were analysed for culture positivity. Urine routine examination was done for urine crystals analysis. Semi-quantitative method (standard loop technique) was done for analyzing significant bacteriuria. The correlation between the urinary crystal and urinary tract infection were analysed by odds ratio.
Results and Conclusion: A cross-sectional study was conducted with 1500 urine specimens. A total of 1500 urine specimens received to microbiology and pathology laboratory were included in the study. Urine with crystals were analysed for culture positivity. Urine routine examination was done for urine crystal analysis. Semi-quantitative method (standard loop technique) was done for analyzing significant bacteriuria. The correlation between the urinary crystal and urinary tract infection were analysed by odds ratio. Out of 1500 urine sample, 155 were found to be crystal positive, in which bacterial isolation rate was more from uric acid crystal positive samples. Escherichia coli was the maximum yield from the crystal positive samples with the colony forming unit (cfu) of 10000 cfu per mL (less than significant bacteriuria of 1,00,000 cfu/mL). Other organisms isolated were Klebsiella spp, Pseudomonas spp, Citrobacter spp, Enterobacter spp, Acinetobacter spp. and Proteus spp. Their resistance pattern was also analysed.
Keywords: Bacteriuria, Crystal positivity, Routine examination, Standard loop technique, Urinary tract infection
Full Text:
INTRODUCTION
Crystals in the urine is known as crystalluria. Sometimes crystals are found in healthy people and other times they are indicators of organ dysfunction, the presence of urinary tract stones of a like composition (known as urolithiasis), or an infection in the urinary tract. Some of these disease processes that are associated with these crystals will be the focus of this lesson. Urinalysis is not only used for the diagnosis of urologic conditions such as calculi, urinary tract infection (UTI), and malignancy. It also can alert the physician to the presence of systemic disease affecting the kidneys. A large number of people (up to 20% of the population worldwide) are suffering from urinary stone problem. The majority of stones are composed of oxalates, calcium salts, and phosphates. Among phosphates, magnesium ammonium phosphate hexahydrate (MAPH; MgNH4PO4•6H2O), known as struvite, is the predominant crystalline component. Struvite crystallization is related to urinary tract infections by microorganisms producing urease. Infection-induced urinary stones form as a result of a urinary tract infection by urease-producing bacteria. Infection stones make up approximately 15% of urinary stone diseases and are thus an important group. The basic precondition for the formation of infection stones is a urease positive urinary tract infection. Urease is necessary to split urea to ammonia and CO2 . They are mainly the microorganisms from species of Proteus, which are isolated in the case of 70% of the so-called infectious stones. Proteus species, the motile, Gram-negative bacteria within the Enterobacteriaceae that cause urinary tract infections, primarily in patients with long-term urinary catheters in place or structural abnormalities of the urinary tract. Proteus infections are known to be frequently persistent and difficult to treat and can lead to several complications such as acute or chronic pyelonephritis. Additionally, these species are the most common bacilli associated with the formation of bacteria-induced bladder and kidney stones. Urease is the essential virulence factor of these bacteria involved in stone formation. Ammonia, produced by the enzymic hydrolysis of urea, elevates urine pH, causing super saturation and crystallization of magnesium and calcium ions as struvite (MgNH4PO4.6H2O) and carbonate apatite [Ca10(PO4)6.CO3], respectively. It has been found that, in addition to urease activity, bacterial exopolysaccharides contribute to stone formation. Polysaccharide produced by bacteria may aggregate precipitated urine components to form a stone. When these crystals deposit themselves infection stones form. If these infections are not treated and the stones are not removed, the kidney will be damaged. Thus recurrent urinary tract infection and crystal formation should be analysed promptly and correlated in order to avoid infection induced urinary stones. Thus, the goal of this study is to correlate the urinary tract infection and urine crystal, in order to find the bacteria commonly associated with the crystal positive cases, their significance and also to find their antibiogram.
MATERIALS AND METHODS
A cross-sectional study to analyse the crystal positivity and culture positivity was conducted in the Department of Microbiology at Saveetha Medical College and Hospital after obtaining the university scientific review board approval and ethical committee clearance. A total of 1500 urine specimens received to microbiology and pathology laboratory were included in the study. Urine samples were processed by standard urine route examination and standard loop technique as follows. Microscopic Urinalysis: To prepare a urine specimen for routine examination, a fresh sample of 10 to 15 mL of urine were centrifuged at 1,500 to 3,000 rpm for five minutes. The supernatant then is decanted and the sediment resuspended in the remaining liquid. A single drop is transferred to a clean glass slide, a cover slip is applied and observed under 40X. Standard loop technique: Specimens arriving at the laboratory were inoculated onto a blood agar plate and a MacConkey by using a 0.001-ml calibrated loop. The well-mixed urine was sampled with the calibrated loop and plated onto the surface of the blood agar plate. A single streak of the inoculum was spread across the center of the plate, and the inoculum was then spread perpendicular to the primary streak to ensure a semiquantitative colony count. MacConkey agar plate was also inoculated in the same manner. Plates were incubated at 37°C and examined once at 18 to 24 h. If no growth was observed or if the colony count was less than 10 CFU per plate, the plates were kept for an additional 24 h and read again. Positive cultures and obviously contaminated cultures were reported at 24 h.
RESULT
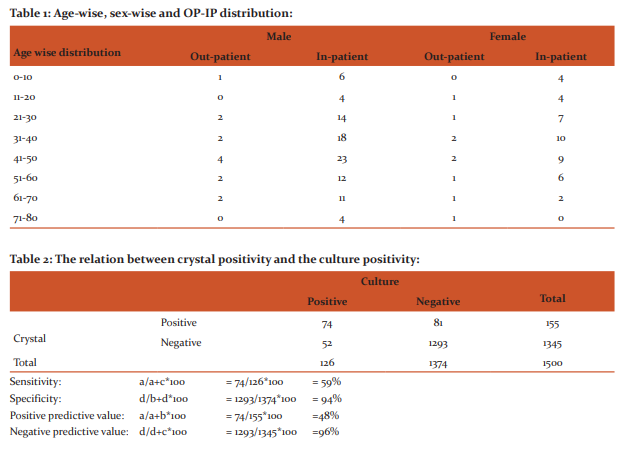
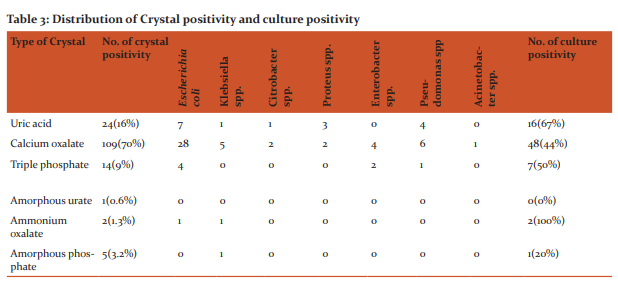
Out of 1500 urine sample, crystal positivity was found more in male in-patients (68%) of age group 41-50(17%). The agewise, sex-wise and IP-OP distribution was shown in table 1. Among the 1500 urine specimens, 155(10%) was found to be positive for urinary crystals. Out of which calcium oxalate were 109(70%), uric acid 24(16%), Triple phosphate 14(9%), Amorphous phosphate 5(3.2%) and Amorphous urate 1(0.6%). The bacterial isolation was higher (67%) from the uric acid crystal positive samples. Patients infected with uric acid crystal yielded higher frequency of Escherichia coli (44%) that too of 10000 colony forming unit per mL in 22% cases. Out of which, 56% were found to be ESBL producers, 1.2% were found to be multi-drug resistant and 0.5% was Pan-drug resistant organism. The relation between crystal positivity and culture positivity and their sensitivity, specificity, positive predictive value and negative predictive value is shown in table 2. The distribution of crystal positivity and culture positivity was shown in table 3. The antibiotic resistance of those culture positive cases was shown in Figures 1,2,3 and 4.\
DISCUSSION
A large number of people (up to 20% of the population worldwide) are suffering from urinary stone problem [9]. The majority of stones are composed of oxalates, calcium salts, and phosphates. Among phosphates, magnesium ammonium phosphate hexahydrate (MAPH; MgNH4PO4•6H2O), known as struvite, is the predominant crystalline component [10,11]. Formation of infectious urinary calculi is the most common complication accompanying urinary tract infections by members of the genus Proteus. The major factor involved in stone formation is the urease produced by this bacteria.7 It has been found that, in addition to urease activity, bacterial exopolysaccharides contribute to stone formation. Polysaccharide produced by bacteria may aggregate precipitated urine components to form a stone which is also said to be infection induced urinary stones.8 In our study the findings of 1500 urine samples are, 155 cases (10%) were found to be crystal positive. Out of which 19 were out-patient and 136 were in-patients. Out of 155, 104 (67%) were male and 51 (33%) were found to be fe-male. Another study done by Naseri et.al., revealed that, out of 183 patients, 130 cases (71%) were female and 53 patients (29%) male. Most of the patients (61.9%) were between 2 years of old. In our study, 27 crystal positive samples were between the age group of 41-50. 3 In our study crystal positivity is still 48%. In a study done by Yousefimashouf et.al., 28% of tested samples had positive culture. From the positive cases, Staphylococcus epidemidis (40.4%), Acinetobacter baumannii (10.6%) and Escherichia coli (8.5%) were the most common isolates. In our study Escherichia coli were the majority isolates from uric acid crystal positive samples. The similar views have been expressed by David et.al., that the majority of UTI are caused by Escherichia coli.1 Out of 40 Escherichia coli strains, 56% were found to be ESBL producers, 1.2% was found to be multi-drug resistant and 0.5% was Pan-drug resistant organism. The most rate of sensitivity of Escherichia coli was against to gentamicin and Psuedomonas aeruginosa to ciprofloxacin in a study done by Yousefimashou et. al., The data revealed that the bacteria isolated from crystal positive urine specimens had multidrug resistance. Yousefimashouf et.al., also reported the same. Among all chemical compositions, calcium oxalate (in either pure or mixed form) was the most common and found in 64 and 75% of the stone formers with and without bacterial isolates, respectively in a study done by Ratree Tavichakorntrakool et al., Nevertheless, limitations of our present study should be noted. Bacteria found in urine might promote formation and growth of these crystals. But it has to be confirmed with stone matrices and crystals culture. Therefore, extensive investigations of crystals are required to address this concern. In summary, our data indicate that the prevalence of UTI associated with crystal positivity is still high (48%). In addition, UTI are frequently associated with almost all chemical types of kidney stones, not only struvite, and Escherichia coli, not urea splitting bacteria, is the most common causative microorganism found in urine.
CONCLUSION
Hence in our opinion it is mandatory to check the urine complete analysis along with the urine culture and sensitivity. If not so, at least with the crystal positive urine samples culture has to be done in order to control infection induced urinary stones.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of Funding: nil Conflict of Interest: nil
References:
1. Johnson, D.E., Lockatell, V., Russell, R.G., Hebel, J.R., Island, M.D., Stapleton, A. Comparison of escherichia coli strains recovered from human cystitis And pyelonephritis infections in transurethrally challenged mice. infection and immunity. July 1998, p. 3059–3065 vol. 66, no. 7
2. Yousefimashouf, R, Molazadeh, N, Antibiotics study on staphylococcus spp. Strains isolated from venous and urinary catheters in nicu of hamadan hospitals, west ran. Arch dis child 2012;97(suppl 2):a1–539.
3. Naseri, M, Alamdaranm, SA. Urinary tract infection and predisposing factors in children doi:10.1136/archdischild-2012-302724.0890.
4. Rozalski, A., Torzewska, A., Magdalena, M. Proteus sp. – an opportunistic bacterial pathogen – classification, swarming growth, clinical significance and virulence factors. folia biologica et oecologica 8: 1–17 (2012).
5. Tavichakorntrakool, R, Prasongwattana V, Sungkeeree S, Extensive characterizations of bacteria isolated from catheterized urine and stone matrices in patients with nephrolithiasis. Nephrol dial transplant (2012) 27: 4125.
6. Torzewska, A., Staczek, P. and Rozalski, A., Crystallization of urine mineral components may depend on the chemical nature of proteus endotoxin polysaccharides journal of medical microbiology (2003), 52, 471–477.
7. Benramdane, L., Bouatia, M., Idrissi, M.O.B, and Draoui, M. “infrared analysis of urinary stones, using a single reflection accessory and a kbr pellet transmission,” spectroscopy letters, vol. 41, no. 2, pp. 72–80, 2008.
8. Lerner SP, Gleeson MJ, and Griffith DP., “infection stones,” journal of urology, vol. 141, no. 3, pp. 753–758, 1989.
9. Kramer, G, Klingler, HC., and Steiner, GE. “role of bacteria in the development of kidney stones,” current opinion in urology, vol. 10, no. 1, pp. 35–38, 2000.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





