IJCRR - 8(18), September, 2016
Pages: 26-29
Date of Publication: 21-Sep-2016
Print Article
Download XML Download PDF
INTRODUCING VERTICAL INTEGRATED TEACHINGFOR 3RD M.B.B.S. PHASE II STUDENTS
Author: Nitin R. Mudiraj, Priya S. Patil, Manisha R. Dhobale
Category: Healthcare
Abstract:Aims: Current medical education imparts knowledge in a disjoined manner so that it is difficult for undergraduates to co-relate information in clinical context. The aim of this study was to introduce vertical integration for undergraduate medical students and to analyse its impact on the students and faculty.
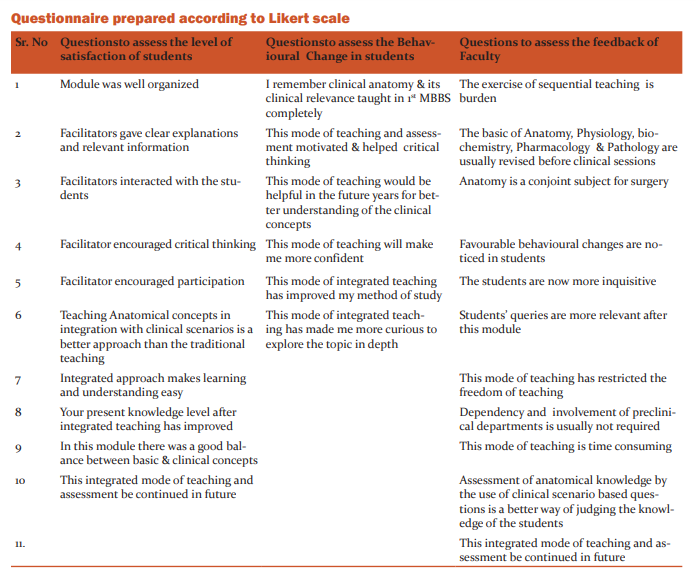
Materials and Methods: An innovative Vertical integrated teaching module was carried out at our Medical College with the cooperation of Surgery and Anatomy departments. Framing of proposed time table and curriculum design was done. 40 students and 19 faculties participated in this project. Pre-test and post-test assessment was carried out after each session. A separate questionnaire was given to students and faculties for their feedback.
Result: Statistical analysis showed that there was a significant improvement in the students' mean scores, knowledge and understanding level. The students were highly satisfied with this method of teaching and interestingly 95 % of students showed positive behavioural changes. The response of the faculty was of mixed type but most of them responded positively to the exercise of integrated teaching.
Conclusion: We conclude that vertical integrated teaching in a medical curriculum is found to facilitate attainment of knowledge and improve the affective and psychomotor domains along-with creating a positive behavioural change in the students. The results of VIT are encouraging so that it can be expanded to many more topics to enable a smooth transition from traditional to integrated teaching over the coming years
Keywords: Vertical integrated teaching, Medical curriculum, Curriculum design
Full Text:
INTRODUCTION
Current medical education imparts knowledge in a disjoined manner. Theundergraduate students are unable to co-relate and analyse information and aptly use it in clinical context. Vertical integration is defined as the integration betweenthe clinical and basic science sections of the curriculum.[1,2] Integration can occur throughout the curriculum with the basic medicaland clinical sciences beginning in the early years ofthe curriculum and continuing until the later years.[1]Integrated teaching is considered as the best reform in the medical curriculum.[2]It is found to be beneficial in facilitation of attainment of knowledge. It enables the students to correlate the topic taught in a clinical subject to biological principals and mechanisms, as taught in basic medical sciences. It is thought to enhance the skill of clinico- pathological correlation and also help to improve the cognitive and psychomotor domains of the students.[3]In 1997 the regulation on undergraduate medical education recommendedefforts to encourage integrated teaching betweenthe traditional subject areas. [2] Using a problem based learning approach would avoid compartmentalization of various disciplines and achieve both horizontal and verticalintegration in the different phases.[3,4] Considering this the present study was undertaken with the aim of introducing the method of vertical integrated teaching [VIT] for undergraduate medical students and to analyse its impact on students’ knowledge level and components of affective domain (satisfaction level and behavioural changes) as well as to assess the impact of VIT on the faculty.
Methodology
An innovative vertical integrated teaching module was carried out at our Medical College with the co-operation and active participation of departments of Surgery and Anatomy. Framing of proposed time table: The head of departments and faculty from departments of Surgery and Anatomy together framed a time table. At the same time the faculty was sensitized regarding such an activity. The interested faculty volunteered to conduct the sessions. Work flow charts and curriculum design: Curriculum committee consisted heads of department of Anatomy and Surgery. Series of meetings were held and the four topics selected for Vertical integrated teaching were Anatomy and Surgery of inguinal canal, mammary gland, venous drainage of lower limb and thyroid gland. The time-table was finalized accordingly. Implementation and execution: 40 students and 19 faculties participated in this project. Pre-test and post-test assessment was carried out for each vertical integrated session. A separate questionnaire was given to students and faculty for their feedback on such integrated teaching methodology.
Observations
The data obtained from the pre and post-test questionnaire and feedback from students and faculties was analysed statistically. The observations were tabulated and results were drawn.
RESULTS
Impact of VIT on Students:Statistical analysis of the pretest and post-test questionnaire was performed to assess the impact of VIT on students at three different levels through separate questionnaires. The following levels were assessed and analysed.
i. Knowledge level
ii. Satisfaction level
iii. Behavioural change
Impact of VIT on Faculty:
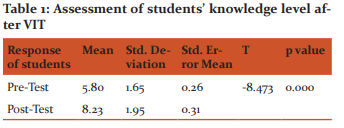
The perception of faculty regarding VIT and their feedback was taken through questionnaire and was also analysed. i] Assessment of knowledge level: Statistical analysis of the pre-test and post-testquestionnaire showed that there was a significant improvementin the mean scores of students as well as their knowledge and understandinglevel. The p value was < 0.001 which was statistically highly significant. [Table 1]
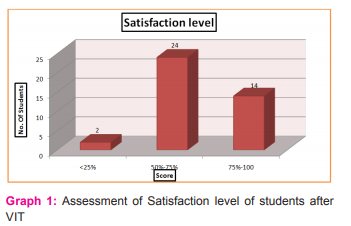
ii] Assessment of satisfaction level:
On the basis of the feedback of students itwas seen that 35 % students were highly satisfied and 60 % weresatisfied with vertical integrated teaching program while only 5 % students feltthat it did not matter to them, as shown in Graph1.
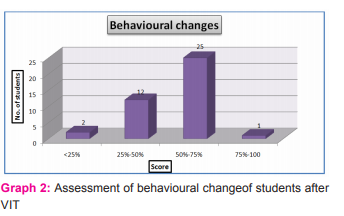
 iii] Assessment of behavioural change:
iii] Assessment of behavioural change:
The behavioural changes were divided into three categories as follows- those showing no or slight behavioural change, positive change and excellent behavioural change. 65 % students showed excellent behavioural change, 30 % showed positive change while 5 % students showed no behavioural changes. Graph 2
iv] Assessment of faculty:
The response of the faculty was of mixedtype. 35 % responded positively to the exercise of sequential teaching. 64 % faculty revised the basic of Anatomy, Physiology and other subjects prior to thelecture. 94% faculty agreed that Anatomy is a conjoint subject for Surgery. 82% faculty supported the fact that integrated teaching brought about favourable behavioural changes in students, 70 % felt that such teaching sessions made students more inquisitive and 94 % agreed that students’ queries were more relevantafter vertical integrated teaching.
DISCUSSION
Curriculum renewal through integration is promoted by many medical educational organizations. The challenge that we as educationists face today is the successful integration across medical disciplines in order to obtain maximum benefit to our students. [5] Vertical integrated teaching [VIT] involves the combination and correlation of basic sciences knowledge to clinical scenarios so as to deepen the understanding and stimulate advanced learning and problem solving attitude. [6,7] Such an approach might aptly be called as holistic learning as it adds to student perception as well as satisfaction. In our study we have also seen that VIT brings about changes in student’s attitude towards learning and positive changes in their behaviour. In this study while assessing the impact of VIT on knowledge level of the students it was seen that VIT improved the knowledge level and student performance so that it was superior to traditional teaching to some extent. It makes understanding of the topic easier and correlation of clinical cases with basic science knowledge gives clarity of concepts. Though these are the advantages of VIT there are a few shortcomings too. Integration cannot be applied to all topics and many times integration leads to content overload as too much knowledge is given in short period of time. Similar observations are noted by other authors in their studies. [1,3,4] Success of any innovative teaching learning method depends on satisfaction of both the teacher or facilitator and the student or benefactor. In this study we assessed the faculty feedback in relation with the relevance of VIT, the usefulness of integration, change in students’ behaviour and attitude in class as well as their perception in terms of preparation of the topic, efforts and time required and whether such activity could be continued in future. Almost all the faculty involved in this module agreed that integrated teaching required more efforts in planning of the session; it is time consuming and needs devotion to execute it successfully. Hence only enthusiastic and voluntary faculty if involved can do the proper planning, organization and execution of VIT to make the sessions more interesting and rewarding. In the studies by other authors like Vidic et al, Bryhildsen et al have also emphasized on efforts of faculty , need for interdepartmental cooperation and time and effort needed for integrated teaching. [8,9] The students on the other hand were highly satisfied with VIT and 95% students found integrated teaching rewarding. They were happy with the planning and execution of the VIT module and thought that the interaction with the teachers helped them to get their ideas clear. The topics were well balanced, information was relevant and it encouraged their critical thinking. Most of the studies have also agreed that students found such integrated teaching sessions helpful in their bedside clinics.[ 4,5] Interestingly in the present study 95 % of students showed some positive behavioural changes. These were assessed through the questionnaire which highlighted their shift in attitude towards teaching learning. Most of them positively accepted that VIT enhanced their critical thinking, motivated them to modify their method of study and improved their approach to difficult topics. VIT made them more curious to explore topics in depth and this helped to uplift their confidence. Such an aspect of integrated teaching is not dealt with by many authors and it forms an asset of our study. The results of introducing integrated teaching to final year MBBS students are promising as they show some obvious advantages like: a] integration reduces fragmentation and compartmentalization of topics, b] it prevents repetition and c] stimulates students to apply knowledge to clinical concepts. Some of the advantages for the faculty involved are integration promotes interdepartmental collaboration and rationalization of teaching resources. However some difficulties that could be encountered during planning of such sessions are that it requires cooperation of faculty and additional inputs from them. The students also may feel burdened and there is paucity of data on long term benefits of integrated teaching. We are now prepared to introduce such modules for many more topics and more studies in the near future will help us to be ready for a transition from traditional to integrated teaching for undergraduate medical students.
CONCLUSION
We conclude that vertical integrated teaching [VIT] in a medical curriculum is found to facilitate attainment of knowledge and improve the affective and psychomotor domains alongwith creating a positive behavioural change in the students. The present era requires aparadigm shift from independent to interdependent teaching to develop competent medical graduates.VIT is encouraging, so that it can be inculcated in the curriculum and enable a smooth transition from traditional to integrated teaching over the coming years.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. I sincerely thank the institute as well as all the students, colleagues, office clerk and non-teaching staff for their co-operation during this study. Sources of funding: Nil Conflict of interest: Nil
References:
1. Nazish Rafique. Importance of vertical integration in teaching and assessment ofphysiological concepts. Journal of Taibah University Medical Sciences 2014; 9(4), 282-288.
2. Medical Council of India (1992) Recommendations of the workshop on Need based Curriculum forunder graduate medical education, MCI: NewDelhi.
3. Joglekar S., Bhuiyan, P.S. and Kishore, S.Integrated Teaching–our experience, Journal of Postgraduate Medicine 1994, 40, 4, pp 231-232.
4. Kalpana Kumari M. K., Vijaya V. Mysorekar, Seema Raja. Student’s Perception About Integrated Teaching In An Undergraduate Medical Curriculum Journal of Clinical and Diagnostic Research. 2011 November (Suppl-1), Vol-5(6): 1256-1259
5. David G. Brauer, Kristi J. Ferguson. The integrated curriculum in medical education: AMEE Guide No. 96. AMEE GUIDE 2015, 37: 312–322.
6. Rajan SJ, Jacob TM, Sathyendra S. Vertical integration of basic science in final year of medical education. Int J App Basic Med Res 2016;6:182-5.
7. Vyas R, Jacob M, Faith M, Isacc B, Rabi S, Satish Kumar S, Selvakumar D, Ganesh.A. An effective, integrated learning programme in the first year of the medical course. The National Medical Journal of India. 2008; 21:1-6.
8. Vidic B, Weitlauf HM. The horizontal and vertical integration of academic disciplines in the medical school curriculum. ClinAnat 15:233-5.
9. Brynhildsen J, Dahle LO, Behrbohm Fallsberg M, Rundquist I, Hammar M. Attitudes among students and teachers on vertical integration between clinical medicine and basic science within a problem-basedundergraduate medical curriculum. Med Teach 2002;24:286-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





