IJCRR - 4(6), March, 2012
Pages: 139-145
Print Article
Download XML Download PDF
A STUDY TO EVALUATE AND COMPARE ORAL STEREOGNOSTIC ABILITY AND ORAL TACTILE SENSIBILITY OF SATISFIED AND DISSATISFIED SUBJECTS WEARING COMPLETE DENTURE PROSTHESIS
Author: Anupama Prasad, Chethan Hegde, Krishna Prasad D.
Category: Healthcare
Abstract:Context: Evaluating oral stereognostic ability and tactile sensibility in subjects wearing complete denture prosthesis may provide not only useful information about the sensory abilities of denture patients, but may also aid in interpreting the role of adaptation and adjustment to thecomplete denture prosthesis and its co-relation with advancing age. Aim: To evaluate and compare oral stereognostic ability and oral tactile sensibility of subjects wearing removable complete denture prosthesis. Settings and Design: Subjects who are wearing complete denture prosthesis for a period of more than six months . A set of six three dimensional test pieces with different shapes. A standardized, sterilized, machine rolled cotton bud. Materials and Methods: Denture satisfaction of subjects wearing complete denture prosthesis was analysed with the help of a questionnaire. A set of six three dimensional test pieces with different shapes were used for the assessment of oral stereognostic ability of the subject . Another set of same shapes but larger to correlate the shape of the test piece in the mouth with the one on display. The stereognostic ability to identify the shape was scored. A standardized, sterilized, machine rolled cotton bud was used for the assessment of oral tactile sensibility. The sensual perception when the bud lightly touched the dorsal surface of the tongue was assessed by the time taken by the subject to respond to the sense of touch. Statistical analysis used: Statistical analysis carried out using Spearman's rho, and Mann- Whitney U test . Results : There was high negative correlation(p< 0.05) between oral stereognostic ability and denture satisfaction ,no significant correlation(p=0.498) between denture satisfaction and tactile sensation. Conclusion: As the oral stereognostic ability increased, denture satisfaction decreased .Oral tactile sensibility and patient denture satisfaction had no correlation.
Keywords: oral stereognosis, oral tactile sensibility, denture satisfaction.
Full Text:
INTRODUCTION
The loss of teeth may be a significant factor in declining the oral sensory ability of an individual. Due to increased life expectancy there are more elderly citizens who are now seeking a more comfortable oral environment and improved appearance1 .The ability to predict patient‘s performance with complete denture prosthesis remains deceptive2 , irrespective of the clinical proficiency employed in the fabrication of the prosthesis. There are reasons to assume that adaptation and adjustment to the complete denture prosthesis play a role in patient‘s satisfaction3 . Evaluating oral stereognostic ability and tactile sensibility in subjects wearing complete denture prosthesis may provide not only useful information about the sensory abilities of denture patients, but may also aid in interpreting the role of adaptation and adjustment to the complete denture prosthesis and its co-relation with advancing age4 . METHODS Source of data: The study was conducted on fifty edentulous subjects wearing complete denture prosthesis for more than six months.
MATERIALS AND METHODS
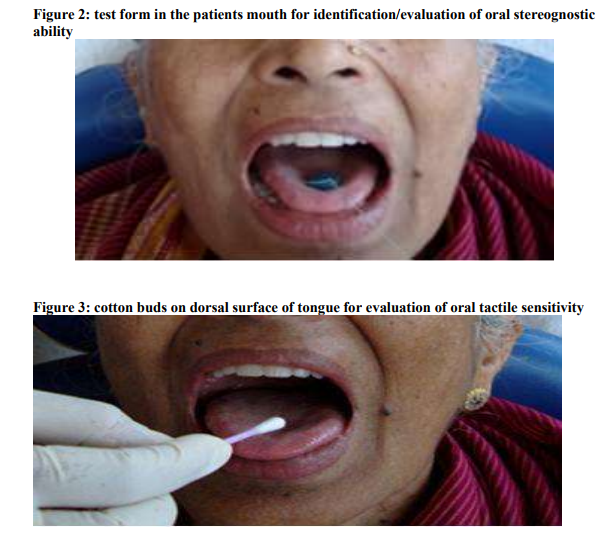
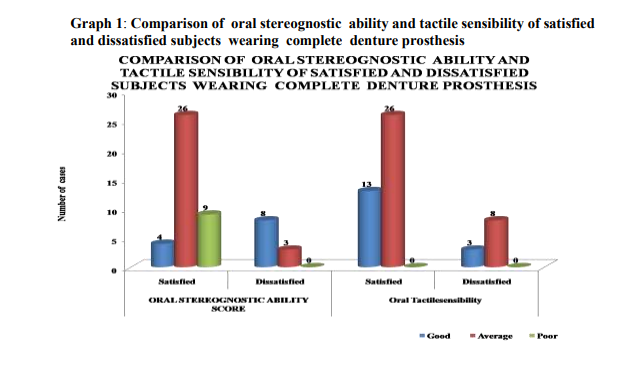
The subjects who were wearing complete denture prosthesis for a period of more than six months , aged between 50 to 60 years were selected for the purpose of the study whose prosthesis were professionally assessed to be good. The subjects were thoroughly examined to rule out any mucosal lesions that might influence the results of the evaluation. Subjects who were under the influence of drugs, drug addicts, intoxications, sedatives, psychic and perverted habits were not included in the study. Subjects were selected irrespective of their gender, caste, creed, colour and socioeconomic status. Patient‘s denture satisfaction was analysed with the help of a questionnaire based on which they were categorized as satisfied (11-21 score) and dissatisfied (0-10 score). A set of six , three dimensional test pieces with different shapes fabricated with heat cure acrylic resin, having 5mm thickness, diameter varying from 10-14mm and secured with threads to prevent accidental swallowing were used for the assessment of oral stereognostic ability of the subjects3,4,5,6,7. Another set of same shapes but bigger in size was kept outside for identification (figure1). These different shapes are: Heart- shaped, triangular, circular, square, semi- circle, rectangle. Heart- shaped and triangle, circle and semi-circle, square and rectangle were taken as similar shapes 3,4,5,6,7 . Heat cured acrylic resin test forms of six different shapes were obtained by processing wax patterns of planned thickness and radius. Each test form was placed on dorsal surface of extended tongue and then taken into mouth (figure2). Subject was instructed to move the form around, manipulate the test forms which helped him or her in identification- e.g. Sucking, chewing, pressing against palate or lips and then to point to one of the reference forms on display as soon as the oral identification of the stimulus was achieved. The stereognostic ability to identify the shape was then scored on a three point scale7,8 .The test was conducted on fifty subjects blindfolded during the procedure randomly. The answers were scored on a three point scale: two points for correct identification of test form , one point for identification of similar test form, zero point for incorrect identification of the test form. The answers given by patient on each form were then summed. Hence each patient received a total oral stereognosis score varying from 12 for all correct identification and 0 for all incorrect identification. It was then finally categorized as good (9-12 score), average (5-8 score) and poor (0-4 score). A standardized, sterilized, machine rolled cotton bud was used for the assessment of oral tactile sensibility. Tactilekinaesthetic perception (TKP) is the processing, arrangement, evaluation, and integration of sensations, which are transmitted via both surface and depth sensibility. The cotton bud was lightly touched on to the dorsal surface of the tongue(figure 3) and the sensual perception was assessed by the time taken (120+/-4seconds) by the subject to respond as YES or NO to appreciate and respond to the sense of touch and was thus scored on a three point scale. An answer by patient as ?NO? even after the roll of cotton touched the surface of tongue for more than 120+/-4 milli seconds was scored as ?0? points and was considered to have poor oral tactile sensibility. An answer by patient as ?YES? when the roll of cotton has just lightly touched the surface of the tongue for less than 120+/-4 milli seconds was scored ?2? points and considered to have an good oral tactile sensibility. An answer by patient as ?YES? when the roll of cotton touches the surface of the tongue properly was scored ?1? points and considered to have an average oral tactile sensibility.
RESULTS
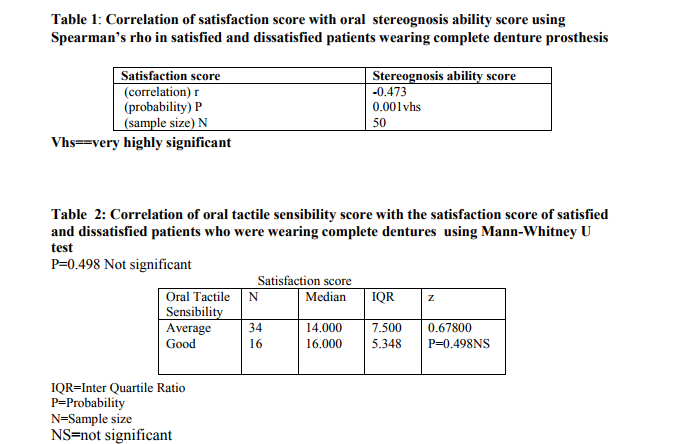
Graph 1 compares oral stereognostic ability and tactile sensibility of satisfied and dissatisfied subjects wearing complete dentures. Among 39 (78%) of satisfied subjects wearing complete denture prosthesis, four( 8%) subjects had good oral stereognostic ability, 26( 52%)subjects had average oral stereognostic ability and nine (18% )subjects had poor oral stereognostic ability .On the other hand 13 (26%) subjects had good tactile sensibility , 26 (52%) subjects had average tactile sensibility and none of the subjects had poor tactile sensibility. Among the dissatisfied group of 11(22% )subjects representing the total sample taken, eight(16%) subjects had good oral stereognostic ability ,three (6%) subjects had average oral stereognostic ability and four(8%) subjects had good oral tactile sensibility and seven (14%) subjects had average oral tactile sensibility score. Table1 correlates denture satisfaction score with oral stereognosis ability score using Spearman‘s rho test in satisfied and dissatisfied patients wearing complete denture prosthesis and was found denture satisfaction and oral stereognosis ability to be having negative correlation r = - 0.473 with P < 0.001 . Table 2 correlates oral tactile sensibility score with the median of satisfaction score using Mann-Whitney U test. Among the 34 subjects with average oral tactile sensibility correlated with median satisfaction score of 14.000, Inter quartile ratio of 7.500 was obtained and among the 16 subjects with good oral tactile sensibility correlated with median satisfaction score of 16.000, Inter quartile ratio of 5.348 were obtained with z = 0.67800 and probability P value= 0.498 showing no significant correlation between oral tactile sensibility and denture satisfaction.
DISCUSSION
The purpose of the present study was to evaluate and correlate denture satisfaction, oral stereognostic ability and oral tactile sensibility in completely edentulous patients wearing removable complete dentures which were professionally assessed to be good. It was noted that dissatisfied denture patients took less time for identification of forms than satisfied denture patients. It seems likely that correlation of tactile sensibility to adaptation occurs indirectly via denture retention. Gender is considered of no importance8 . Good denture retention requires close contact of base with underlying tissues, closer this fit is, more receptors are stimulated when the denture is loaded, and tactile sensibility therefore increases1 . In the present study, during evaluation of patient‘s satisfaction in subjects wearing complete dentures, it was seen that even with dentures which were professionally assessed to be good there were differences among subjects in denture satisfaction, which signifies that even with good dentures patients had difficulty in adaptation problems as noted by Brill N, Tryde G, Schubeler S9 . According to Capra NF 10, sensory nerves that supply mechanoreceptors in the mucosal lining of the oral cavity, pharynx and larynx provide the substrate for a variety of sensations. They are essential for perception of complex or composite sensory experiences including oral kinaesthesia and oral stereognosis2 . They also contribute to initiation of reflexes and co-ordination and timing of patterned motor behaviours. The response of oral mechanoreceptors to natural stimuli is determined to a large degree by morphological factors such as nature of relationship between nerve ending and certain cellular specializations, their distribution in mucosa, the diameter of their primary afferent nerve fibres and central distribution of these fibres in the brainstem. The ability to recognize threedimensional forms and shapes (oral stereognosis) requires a special combination of stimulation of tactile and pressure receptors and the proprioreceptors of the muscles11.Because of morphological similarities between certain cutaneous mechanoreceptors, the mucosal lining may be considered as an internal continuation of large receptor sheets for localization and detection of mechanical stimuli10 . The tongue may compensate for the loss of role of palate in oral sensation in complete denture wearers. It might suggest that role of tongue in stereognosis is far more important than the input of palatal receptors in this regard and that dentures made of appropriate occlusal vertical dimension and proper arch forms confine tongue in a normal space, allowing it to more easily recognize shapes11,12 . In the present study it is seen that denture satisfaction is subjective and one among every five patients was dissatisfied which may be due to the fact that these patients had a strong and healthy neuromuscular supply and the nerve endings on their surface mucosa was very sensitive to even minute irregularities and surface details on the denture to which they could not adapt easily. The loss of the natural teeth results in the complete loss of the sensory input which has been provided by the periodontal ligament. The same sensory rnechanism that maintained the mandibular posture in the infant is also called upon to maintain it in the adult when the natural teeth are lost. It may also have the additional input from receptors located in the tissue around the dentures13. Normal subjects could distinguish two separate points of contact at the tip and anterior part of the dorsum of the tongue when the distance between the points was greater than 2 to 3 mm. However, two-point discrimination could not be determined on the lateral and posterior dorsal regions of the tongue when the points were less than 1 cm. apart14,15 . The study had certain shortcomings in that oral tactile sensibility had only three parameters like good, average and poor with very small values 2, 1 and 0 respectively which prevented statistical correlation. It would be wise to take wide range of scoring criteria as taken for oral stereognostic testing so that the parameters could be correlated in a better way. This entire area of proprioceptive response to the placement of a prosthodontic replacement needs additional research and study.
CONCLUSION
Within the limitations of this in vivo study, the following conclusions were drawn: 1. Oral stereognosis is inversely related to denture satisfaction, as the oral stereognostic score increased, denture satisfaction score decreased .
2. Oral tactile sensibility had very little correlation with patient denture satisfaction. There was average value of oral tactile sensibility score in both satisfied and dissatisfied patients. 3. Oral tactile sensibility had very little correlation with oral stereognostic ability. Oral tactile sensibility was same in patients whether they had good, average or poor oral stereognostic abilities.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Muller F, Hasse-Sander I, Hupfauf L. Studies on adaptation to complete dentures .Part I : Oral and manual motor ability. J Of Oral Rehab 1995; 22: 501- 7.
2. Litvak H, Silverman SI, Garfinkel L. Oral stereognosis in dentulous and edentulous subjects. J Prosthet Dent 1971;139-151.
3. Mohammed Q. Al-Rifaiy, Sherfuddin H, Abdullah MA. Oral Stereognosis in predicting denture success. The Saudi Dental Journal 1996; 8:122-30.
4. Muller F, Link IK, UTZ H. Studies on adaptation to complete dentures. Part II Oral stereognosis and tactile sensibility. J Of Oral Rehab 1995; 22: 759- 67.
5. Bhandari A, Hegde C, Prasad DK. Relation between oral stereognosis and masticatory efficiency in complete denture wearers: an in vivo study. Braz J Oral Sci 2010;9:358-61.
6. Shetty M, Prasad DK, Rani G, Shetty NS . Oral Stereognosis- A diagnostic tool. JIAOMR 2007;19: 400-4.
7. Pow EH, Leung KC, McMillan AS, Wong MC, Li LS, Ho SL. Oral stereognosis in stroke and Parkinson's disease: a comparison of partially dentate and edentulous individuals. Clin Oral Investig 2001; 5: 112-7.
8. Jacobs R, Bou Serhal C, van Steenberghe D. Oral stereognosis: a review of the literature. Clin Oral Investig 1998; 2: 3–10.
9. Brill N, Tryde G, Schubeler S. Aspects of occlusal Sense in natural and Artificial Teeth. J Prosthet Dent 1962; 12: 123-8.
10. Capra NF. Mechanisms of oral sensation. Dysphagia 1995;10: 235-47.
11. Ingervall B, Schmoer R. Effect of surgical reduction of the tongue on oral stereognosis, oral motor ability and the rest position of the tongue and mandible . Am J Ortho Dentofac Orthop 1990; 64:569-72.
12. Ikebe K, Amemiya M, Morii K, Matsuda K , Furuya M , Yoshinaka, Yoshinoka M, Nokubi TA. Association between oral stereognostic ability and masticatory performance in aged complete denture wearers. Int.J.Prosthodont 2007; 20: 245-50.
13. Mantecchini G, Bassi F, Pera P, Preti G. Oral stereognosis in edentulous subjects rehabilitated with complete removable dentures. J Oral rehab 1998; 25: 185-9.
14. Crum RJ, Loiselle RJ, Oral perception and proprioception: A review of the literature and its significance to prosthodontics .J Prosthet Dent.1972; 28(2):215-30.
15. Catalanotto FA, Henkin RI. Manual and Oral Sensation in Patients with Cushing's Syndrome. J Dent Res 1977; 56 (7): 866-70.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





