IJCRR - 4(6), March, 2012
Pages: 56-62
Print Article
Download XML Download PDF
INTER AND INTRA-RATER RELIABILITY OF THE CRANIOCERVICAL FLEXION TEST BY USING MODIFIED
SPHYGMOMANOMETER AS A PRESSURE BIO-FEEDBACK
Author: Harshit Soni, Dharti Hingarajia, Sushant Dey, Nishant Tejwani
Category: Healthcare
Abstract:Background and Objective: The Cranio-Cervical Flexion Test (CCFT) is a reliable clinical and research test to measure the endurance of the Deep Cranio-Cervical Flexors (DCCF) muscles via Activation Score (AS) and Performance Index (PI) by using Chattanooga Pressure Biofeedback unit (CPBU). In India, we use modified sphygmomanometer instead of CPBU for this test, but the data on reliability of the instrument is scarce. So present study was carried out to check inter and intra-rater reliability of the CCFT by using modified sphygmomanometer. Methods: 50 subjects were selected from the age group of 17 to 22 years. For inter-rater reliability the AS and PI were measured on each subject by two different experienced Physiotherapists and For intra-rater reliability the same was measured on two occasions with 7 days gape by the same therapist. ICC-Pearson was calculated to check inter and intra-rater reliability. Results: For AS and PI good inter-rater reliability determined by the ICC= 0.709 and 0.752 respectively and excellent intra-rater reliability determined by the ICC=0.820 and 0.885 respectively. Conclusion: The CCFT by using modified sphygmomanometer showed
good inter-rater and excellent intra-rater reliability.
Keywords: Cranio-Cervical Flexion Test, Modified Sphygmomanometer, Deep Cranio-Cervical Flexors, Reliability
Full Text:
INTRODUCTION
The Cranio-Cervical Flexion Test (CCFT) is a clinical test of the anatomical action of the deep cervical flexor muscles, the longus capitis, and colli.1 It has evolved over 17 years as both a clinical and research tool and was devised in response to research indicating the importance of the Deep Cranio-Cervical Flexors (DCCF) in support of the cervical lordosis and motion segments and clinical observations of their impMATERIAL AND METHODSairment with neck pain.1-5 CCFT is a low-load test performed in the supine position with the patient guided to each stage by feedback from a pressure sensor placed behind the neck.1 The features assessed in this test are the Activation Score (pressure that subject can achieve and hold for 10 seconds) and the Performance Index (calculated by multiplying the activation score by the number of successful repetitions) of the DCCF during the performance of five progressive stages of increasing craniocervical flexion range of motion.1,6 The CCFT using Chattanooga Pressure Biofeedback unit (CPBU) is considered as the most reliable tool as proven by both clinical and EMG studies compared to other tests for the measurement of DCCF muscle endurance in subjects with and without neck pain.1,7,8,9 In previous Indian studies, modified sphygmomanometer has been used as a pressure sensor instead of CPBU for the measurement of DCCF muscle endurance.10,11,12,13 The modified Sphygmomanometer has been found to be a reliable instrument for the measurement of the DCCF isometric muscle strength in subjects with and without neck pain,14 but the data on reliability of the instrument for the measurement of DCCF muscle endurance is scarce which signifies the need of the present study. The main aim of this study is to check inter and intra-rater reliability of the CCFT by using modified sphygmomanometer as a pressure biofeedback to measure DCCF muscle endurance.
MATERIAL AND METHODS
This study was a Co-relational study, conducted at the SPB Physiotherapy College, Surat. The co-relational procedure was ethically revised and approved by the Research and Ethical committee of SPB Physiotherapy College, Surat
Sample Population and Sample Size: 50 asymptomatic subjects; male (n=20) and female (n=30) were selected from the age group of 17 to 22 (Mean age 19.86) years. The study population covers the students of SPB Physiotherapy College, Surat and were recruited according to the inclusion and exclusion criteria mentioned below:
Inclusion Criteria: 1. Subjects with no history of neck pain and 2. Subjects within the age group of 17 to 22 years.
Exclusion Criteria:
1. Subjects with any history of neck pain,
2. Subjects with history of any surgery in and around cervical spine,
3. Subjects performing regular exercises of the neck muscles After meeting suitable criteria, the written informed consent was obtained from each subject after explaining the details of CCFT to be conducted on them. Primary assessment for demographic characteristics and outcome measures was taken. The Same procedure for CCFT was used as described by Jull G 20001 , but in present study modified sphygmomanometer has been used instead of CPBU in original procedure.
(a) Outcome Measure : Activation Score (AS) and Performance Index (PI)
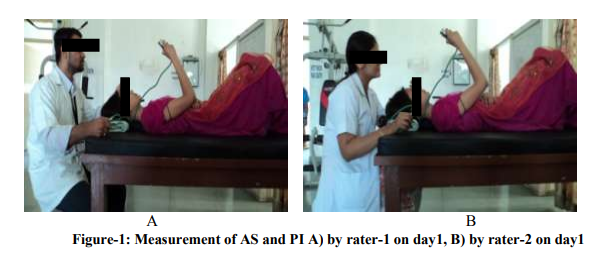
(b) Data Collection: For inter-rater reliability the AS and PI were measured on each subject by two different experienced Physiotherapists, rater-1 and rater- 2 (Figure-1 and Figure-2). For intra-rater reliability the same was measured on two occasions with 7 days gape by the same therapist i.e. rater-2 (Figure-1).
(c)Data Analysis: Two-tailed Intra-class Correlation Coefficient (ICC-Pearson) was calculated by SPSS13.0 version to check inter and intra-rater reliability at 0.01 level of significance for AS and PI separately.
RESULTS
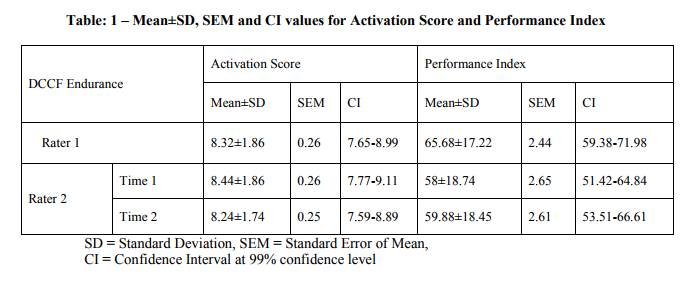
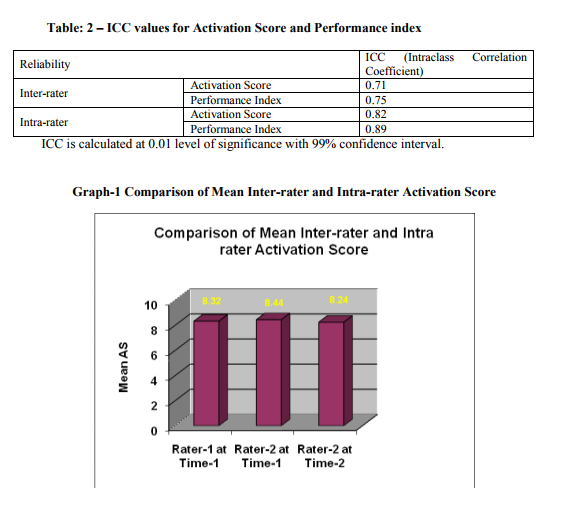
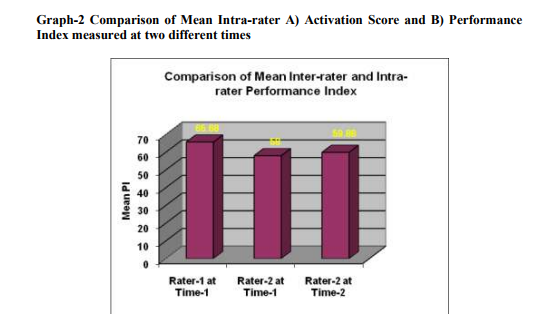
There were no drop outs throughout the study, all 50 subjects were examined by both the therapist timely as per the methodology. Mean age of the subjects was 19.86±1.25 years. Mean weight was 54.98±12.34 kg and mean height was 163.78±9.77cm. Mean BMI was 20.38±3.49. Mean, Standard deviation, standard error of mean and confidence interval at 99% confidence level for activation score and performance index were as per tabulated in table-1 ICC for activation score and performance index measured by two different therapists were 0.71 and 0.75 respectively which shows good inter-rater reliability. (Table-2) ICC for activation score and performance index measured by same therapist at 7 days gape were 0.82 and 0.89 respectively which shows excellent intra-rater reliability. (Table-2)
DISCUSSION
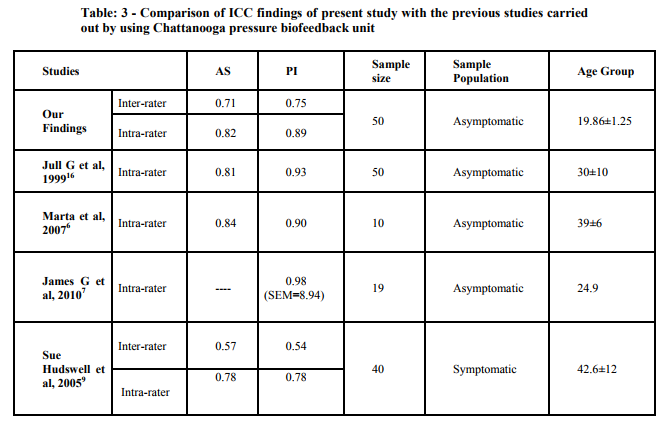
As a result of present study we found good inter-rater and excellent intra-rater reliability determined by ICC (Table - 1 and Table – 2). For quantitative measurements, ICC is the principal tool with Intra-class correlation 0.93 and confidence limits 0.88 – 0.96.15 The criteria for reliability have been defined as ICC: 0- 0.2 = poor, 0.21-0.4 = fair, 0.41-0.6 = moderate, 0.61-0.8 = good and 0.81-1 = excellent.16,17 These findings are matched with the findings [ICC(1,1)=0.81 and 0.93 for AS and PI] of study carried out by Jull G et al, 1999 using CPBU on asymptomatic subjects with age group (30±10) and sample size (n=50) similar to our study16 and also with the findings [ICC(1,1)=0.84 and 0.90 for AS and PI] of study carried out by Marta et al, 2007 with smaller sample size (n=10)6 . However, findings of our study differ from the findings of studies carried out by James G et al, 2010 [ICC(1,1)=0.98, SEM=8.94 for PI]7 and Sue Hudswell et al, 2005 [ICC(1,1)=0.78 for AS and PI, ICC(2,1)=0.57 and 0.54 for AS and PI]9 . The clarification of difference in these findings can be attributed to smaller sample size (n=19) and large SEM (8.94) in the former study and to the selected sample population (which included patient with neck pain) in the later study. (Table-3) Hence, modified sphygmomanometer can be used as a clinical and research tool as a pressure biofeedback instead of CPBU in CCFT as it shows good inter-rater and excellent intra-rater reliability. Cost effectiveness and easy availability of modified sphygmomanometer also accounts for its preference instead of CPBU for Indian therapists.
Future Implications: 1. This study can be explored for all age groups; middle-aged and elderly. 2. Future studies can be carried out with large sample size. 3. Additional research on the same topic can be done which includes symptomatic patients with different cervicogenic disorders.
CONCLUSION
The Cranio-Cervical Flexion Test by using modified sphygmomanometer showed good inter-rater and excellent intra-rater reliability. So that we proved that the modified sphygmomanometer can be used as a pressure bio-feedback instead of Chattanooga Pressure Bio-Feedback in Cranio-Cervical Flexion Test as it is cost effective and easily available for all Physiotherapist.
ACKNOWLEDGEMENTS
First we would like to thank God to bless us enough courage and ability to pursue this work. We are thankful to ?Research Ethical Committee? of SPB physiotherapy College, Surat, for granting us permission to commence on the research. There are no words to gratitude sufficient enough to thank our honorable trusties and Principal Dr. Beena Dave. Who inspired and helped us to choose such a valuable topic for research. We are greatly thankful to all the scholars whose articles are cited and included in references of this manuscript. We are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Last but not the least We are thankful to all our subjects who participated with full cooperation and showed voluntary interest, without them this study would not have been possible. Finally we are thankful to all those who directly or indirectly contributed to this study.
References:
1. Jull G, S.O'Leary, D Falla. Clinical Assessment of the Deep Cervical Flexor Muscles: The Craniocervical Flexion Test. J Manipulative Physiol Ther. 2008;31:525-533
2. Fountain FP, Minear WL, Allison PD. Function of longus colli and longissimus cervicis muscles in man. Arch Phys Med Rehabil. 1966;47:665- 9.
3. Kamibayashi LK, Richmond FJR. Morphometry of human neck muscles. Spine 1998;23:1314-23.
4. Mayoux-Benhamou MA, Revel M, Vallee C, Roudier R, Barbet JP, Bargy F. Longus colli has a postural function on cervical curvature. Surg Radiol Anat. 1994;16:367-71.
5. Vitti M, Fujiwara M, Basmajian JV, Iida M. The integrated roles of longus colli and sternocleidomastoid muscles: an electromyographic study. Anat Rec. 1973;177:471-84.
6. Marta Pérez-de-Heredia, Alberto Molero-Sánchez, Juan C. MiangolarraPage, César Fernández-de-las-Peñas. Performance of the Craniocervical Flexion Test, Forward Head Posture, and Headache Clinical Parameters in Patients With Chronic Tension-Type Headache: A Pilot Study. J Orthop Sports Phys Ther. 2007;37(2):33-39
7. James G, Doe T. The craniocervical flexion test: intra-tester reliability in asymptomatic subjects. Physiother Res Int. 2010 Sep;15(3):144-9.
8. Chiu TT, Law EY, Chiu TH. Performance of the craniocervical flexion test in subjects with and without chronic neck pain. J Orthop Sports Phys Ther. 2005 Sep;35(9):567- 71.
9. Sue Hudswell, Michael von Mengersen, Nicholas Lucas. The cranio-cervical flexion test using pressure biofeedback: A useful measure of cervical dysfunction in the clinical setting? Int J of Osteopathic Medi. 2005;8(3):98-105.
10. Parminder Kaur et al. Relationship of cervicothoracic curvature with muscle strength and endurance in subjects with neck pain. Abstract presented in WCPT-AWP and IAP CONGRESS 2009 – Mumbai.106
11. Akash Chopra et al. Comparative study of multimodel approach and applied relaxation in computer users with intermittent chronic neck pain. Abstract presented in WCPT-AWP and IAP CONGRESS 2009 – Mumbai. 116
12. Patil S P, Torne Pratibha. Effect of endurance training of deep cervical short flexors on correction of forward head posture. Abstract presented in 45th Annual Conference of IAP 2007 – Kolkata.
13. Singh Smita, P Dakshinamurth. Effect of weak core stabilizers on functional reach performance and dynamic reach test. Abstract presented in 45th Annual Conference of IAP 2007 – Kolkata.
14. Vernon HT, Aker P, Aramenko M, Battershill D, Alepin A, Penner T. Evaluation of neck muscle strength with a modified sphygmomanometer dynamometer: reliability and validity. J Manipulative Physiol Ther. 1992 JulAug;15(6):343-9.
15. Li Lu, Nawar Shara: Reliability analysis: Calculate and Compare Intraclass Correlation Coefficients (ICC) in SAS. Statistics and Data Analysis; NESUG 2007:1-4.
16. Jull G, Barrett C, Magee R, Ho P. Further clinical clarification of the muscle dysfunction in cervical headache. Cephalalgia 1999;19(3):179–85.
17. Landis JR, Koch GG. The measurement of examiners agreement for categorical data. Biometrics 1977;33:159-71.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





