IJCRR - 4(8), April, 2012
Pages: 16-22
Date of Publication: 25-Apr-2012
Print Article
Download XML Download PDF
SCENARIO OF BIOMEDICAL WASTE MANAGEMENT IN THE MAJOR HOSPITALS OF SRINAGAR CITY
Author: Rumisa Nazir, G. A. Bhat
Category: General Sciences
Abstract:In order to assess the biomedical waste management; the practices currently operative and compliance with Regulatory Notification for Biomedical Waste (Management and Handling) Rules, 1998, under the Environment (Protection Act 1986), Ministry of Environment and Forestry, Govt of India; the level of awareness regarding biomedical waste management and handling rules among the hospital staff; training imparted to the waste handlers and other particulars regarding risk associated with the handling of biomedical waste, the present study was carried out during May-July 2010 which involved the use of questionnaire method, in-depth interview and personal observation to crosscheck the authenticity of information gathered. During the study, the existing practices of biomedical waste management appeared
to be unsatisfactory; hospitals did not conform to the Biomedical Waste (Management and Handling) Rules, 1998. Waste segregation was found not practiced by the hospitals surveyed and knowledge regarding biomedical waste management was found highest among the doctors i.e. 94.3% and 96% at SKIMS and SMHS hospital respectively indicating that people with higher qualification possessed more awareness regarding the prescribed rules. No specific training and awareness programs on biomedical waste management were organized by the hospital authorities.
Keywords: Biomedical waste, Segregation, Knowledge, Training, Hospital, existing practices.
Full Text:
INTRODUCTION
Hospitals are service oriented institutes that provide medical facilities vital for our life and health. In the healthcare process, waste is generated which usually includes sharps, human tissues or body parts and other infectious materials (Baveja et al., 2000), also referred to as Hospital Solid Waste? and ?Biomedical Waste? (Manohar et al., 1998). It is a real problem of living nature and human world as it carries a higher potential for infection than any other type of waste. Waste is an unavoidable byproduct of human activities, pervading our environment for centuries and will continue to contaminate it. Therefore it is essential to have safe and reliable methods for waste management, focussing both on effective training and supervision. Waste management includes responsible planning of collecting, transporting, processing, and disposing waste material (Campbell, 1988; Stamenkovic, 2007). Within waste management, the healthcare waste management is a process that helps to ensure proper hospital hygiene and safety of healthcare workers and communities (Belkin et al.,1982; Baram, 1989).The primary sources of biomedical waste are hospitals, laboratories, diagnostic centres, blood banks, veterinary hospitals, nursing homes, clinics. Noninfectious waste forms nearly 85% of the waste generated by a hospital and the remaining 10% are hazardous (Pruss and Townend, 1998). Inappropriate and inadequate handling of biomedical waste may have a serious and significant impact on the public health and the environment. Sound management of biomedical waste needs to be given priority and made an integral feature of healthcare services. There is a need to sensitize the top level waste managers by making them aware of not only the various types of waste, but also its generation, collection, containment, handling, storage, transportation, treatment and final disposal. The proper segregation at source is an essential element of the successful waste management programme (pandit, 1999). If the infectious component gets mixed with the general noninfectious waste, the entire mass becomes potentially infectious (Nugget, 2010). Waste management has become a critical issue both at national and international level. In July 1998, the Government of India Environment Protection Act 1986 (Rule 29 of 1986) issued a Notification on Biomedical Waste (Management and Handling), Rules 1998, indicating the rules for the management and handling of biomedical waste. It defined ?biomedical waste? as any waste, which is generated during the diagnosis, treatment or immunization of human beings or animals or in research activities pertaining thereto or in the production or testing of biological and including categories mentioned in Schedule I (1998). Looking into the existing scenario of biomedical waste management in the country it was planned to undertake a study to assess the current practices of biomedical waste management and its compliance with Regulatory Notification for Biomedical Waste (Management and Handling) Rules, 1998, under the Environment (Protection Act 1986), Ministry of Environment and Forestry, Govt. of India; the level of awareness among the hospital staff; training imparted to the waste handlers and other particulars regarding risk associated with waste handling at two major hospitals of Srinagar, Kashmir known for their advanced diagnostic and surgical specialties. The study lasted for a period of 3 months.
MATERIAL AND METHODS
Data regarding the current biomedical waste management practices, level of awareness regarding biomedical waste management and handling rules prescribed therein was collected by the questionnaire method. The design of the questionnaire was based on the survey questionnaire of World Health Organization (WHO) with editorial changes and was framed according to the objective needs of the study. It was served to hospital administrators, doctors, nurses, sanitary staff and hospital engineers. Onsite personal observation of the management practices were carried out for confirmation and as a supplement to information gathered by the questionnaire. Formal interview was conducted to find whether the training is being imparted to the waste handlers and other particulars regarding risk associated with the waste handling. Authenticity of information so obtained was crosschecked through personal observation. The study was conducted with the prior approval of the subjects and institutions.
STUDY AREA
The historical Srinagar city is the summer capital of Jammu And Kashmir State, surrounded by hills on east and north eastern side loc E longitude. Altitude of Srinagar varies from 1580 m in the low lying vicinity of River Jhelum and 1620m on the eastern hill slopes with an average elevation of about 1586m above mean sea level (Bates, 2005). The city lies on both side of river Jhelum, which swirls through the heart of the Srinagar city. For the present study two hospitals were selected which have different characteristics in terms of their size, treatment technology and the type of patients catered. The two study stations were:
Sheri Kashmir Institute of Medical Sciences (SKIMS), Soura
It is a tertiary care hospital, catering to the average socio-economic class of people and provides a total of 600 beds.
Shri Maharaja Hari Singh Hospital (SMHS), Karan Nagar
It is a teaching hospital associated to Government Medical College, Srinagar and is the biggest general hospital in terms of bed capacity (750).
RESULTS
Current biomedical waste management practices
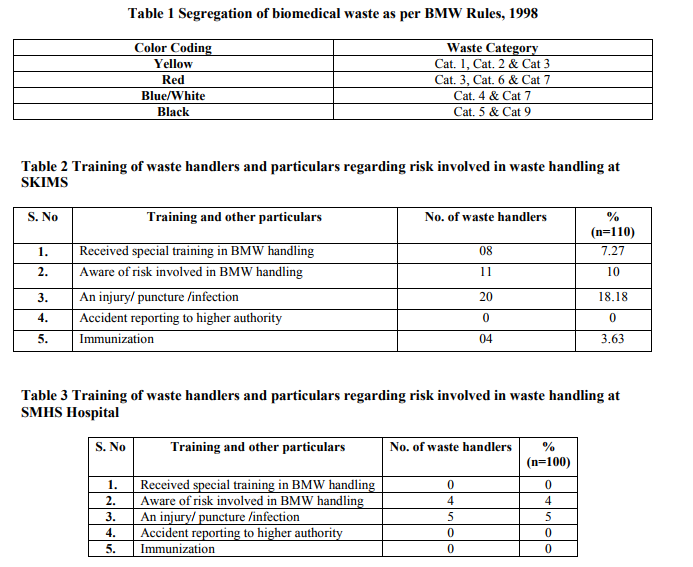
The important inferences regarding the various components of the waste management hierarchy like segregation, packaging, storage, collection, transportation and disposal were drawn and then the framework of compliance was assessed. Barring SKIMS, the waste was not segregated at source as prescribed in the Biomedical Waste Management Rules, 1998 (Table 1). Due to poor segregation practices, the general waste gets mixed up with the infectious waste. Hospitals were using uncovered plastic bins for waste collection provided with same kind of color coded labelled polybags. Polybags were not sealed properly and its integrity was found not to be preserved. In SMHS hospital, waste sharps were contained without being subjected to disinfection in open trays or in any of the bins. While in SKIMS, sharps were disinfected properly and finally incinerated. Waste storage area at SKIMS was of a size appropriate to the quantities of waste produced but did not have secured bins to eliminate the possibility of access to the waste by rodents, flies, or other natural scavengers. The waste was placed in an open area before disposal at SMHS hospital, so it was easily accessible to unauthorized personnel and animals. The transportation of waste to the storage site was done manually in SMHS hospital, while in SKIMS trolleys and pipeline system (Chute) was employed. Biomedical waste was autoclaved and incinerated (Type Brick Kiln; capacity 125 kg/hr) onsite, at SKIMS. Ash so obtained was buried in onsite ash pits, neither lined from below nor sealed above. Liquid waste was treated in the treatment plant and flushed into the sewers (Fig.1). SMHS hospital treats its biomedical waste at Common Biomedical Waste Treatment Facility (CBWTF), Lassipora Pulwama, Kashmir, while the liquid waste was flushed directly into the River Jhelum.
The level of awareness among the hospital staff
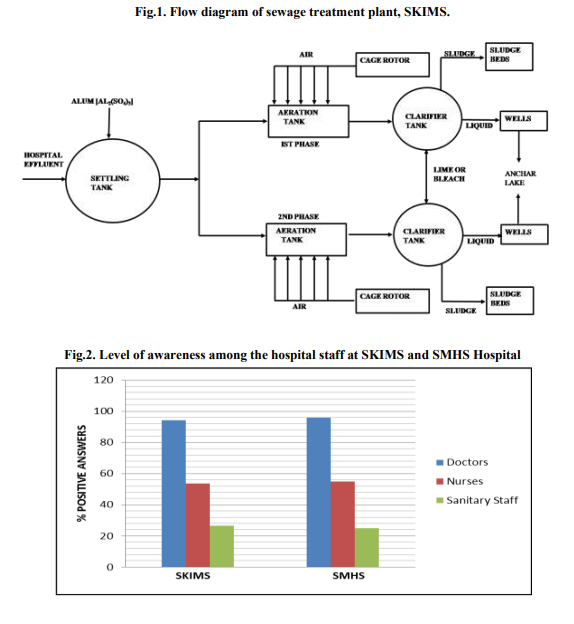
Knowledge regarding biomedical waste management and rules prescribed therein at SKIMS and SMHS hospital was found highest among the doctors in the tune of 94.3% and 96% respectively. Sanitary staff scored the least which indicates that the authority neither informed them in the form of instructions nor did they supervised their biomedical waste management practices (Fig. 2).
Training and other particulars regarding risk in the waste handling
Although 10% waste handlers were aware of risks involved in biomedical waste handling, 7.27% had received special training on this aspect. While 18.18% of waste handlers suffered from skin infections but none reported it to the higher authorities. 3.63% of waste handlers stated about being immunized (Table 2). Out of 100 waste handlers which were interviewed at SMHS hospital, 4% of waste handlers were aware of risks involved in biomedical waste handling. None has received special training on this aspect, 5% suffered from eye and skin infection and none reported to higher authority. None was found immunized against the infections (Table 3).
DISCUSSION
Biomedical waste seems to have received very little attention in waste management process in Srinagar city, Kashmir. Neither the government nor hospital authority pays proper attention to its management. Biomedical waste is disposed off randomly leading to unhealthy and hazardous environment affecting people living within the vicinity of health institutions in particular and city dwellers in general. The study revealed that the hospitals do not practice segregation, which was due to lack of trained waste handlers and proper supervision. As a result of failure to follow segregation protocols and infrastructure, the waste as a whole is potentially infectious. Rijal et al., (2007) observed segregation far from satisfactory in most of the healthcare institutions. Such a practice of non-segregation may increase the costs of final disposal of the waste. Hospitals under study were found not to be complying with the specifications for storage facilities. Untreated waste in SKIMS was transported to the collection point through pipeline system, which consists of a network of pipelines from various floors within the hospital.The vertical conduit allows the waste to be collected at a central collection point by means of gravity, thus preventing the horizontal movement of waste through the hospital corridors. But, there are some hygienic and technical problems associated with it (Bashir, 2009). Then the waste was carried to the onsite incinerator plant. In SMHS hospital, waste was collected manually and trolleys meant fo the same were not used at all. Part of the waste was taken to the CBWTF and part to the municipal site at Achan Syedpora for its disposal. Barring SKIMS, liquid waste from the other hospital was flushed into the River Jhelum without any treatment. Observation similar to the present investigation have also of course been made by the Purvi et al., (2006) in Gujarat, India. Doctors outscored nurses and sanitary staff in knowledge regarding biomedical waste management and rules prescribed therein.Doctors rated 94.3% in SKIMS, 96% in SMHS hospital with regard to knowledge.Sanitary staff exhibited poor knowledge in the tune of 26.6% and 25% respectively.This was indicative of the fact that the sanitary staff was never given even a capsule training with regard to biomedical waste management.Continuous awareness regarding biomedical waste management was needed to be promoted. It was found that the waste handlers were not in receipt of special training on biomedical waste handling which was prerequisite and necessary to ensure an understanding of the risks that wastes pose, to know how to manage waste etc. Waste handlers were found suffering from infections with no reporting to higher authorities. Reportedly, very few waste handlers were found immunized against the infections. Hence implementation of a waste management policy, training and motivation must be given paramount importance to meet the current needs and standards of biomedical waste management (Sharma and chauhan, 2008).
CONCLUSION
The management of biomedical waste in the study centres do not conform to the Biomedical waste (Management and Handling) Rules, 1998. It seemed that no significant action has been taken by the hospital authorities in compliance with the rules. The resistant attitude of hospital staff, lack of technical knowhow, and lack of skilled manpower could be responsible for the non-compliance of biomedical waste management rules. In order to achieve an effective and sustainable biomedical waste management system in the hospitals, the following suggestions were put forward for consideration:
(i) Segregation practices were needed to be imposed within hospitals to separate infectious waste, which will result in a clean solid waste stream.
(ii) Demonstrative programs should be conducted for employees who are in direct contact with the biomedical waste in order to provide an understanding of risks and importance of health and safety measures during handling.
(iii) Periodic meetings of staff involved with the waste management be conducted in order to discuss problems and provide suggestions.
(iv) Strict enforcement of law will help in improving the overall biomedical waste management scenario in Srinagar city.
ACKNOWLEDGEMENT
We acknowledge with thanks the (i) administrative staff of SKIMS and SMHS hospital, Srinagar, India for granting permission and cooperation during the study period and (ii) Scientists of State Pollution Control Board for their support and invaluable help that provided this study much of its pace and momentum. The noted patience of respondents is also highly appreciated. Authors acknowledge the immense help received from the scholars whose articles are cited and included in reference of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Baram, M. 1989. Hospital management of medical waste: legal framework and policy issues, Ch. IV: Perspectives on Medical Waste, Albany, NY: The Nelson A. Rockfeller Institute of Government, State University of New York.
2. Bashir, F. 2009. Study of solid waste management at SKIMS. School of health sciences IGNOU.
3. Bates, E.C. 2005. A Gazetteer of Kashmir. Pp: 352.
4. Baveja, G., Muralidhar, S., Aggarwal, P., 2000. Hospital Waste Management- an overview. Hospital Today
5 (9), 485-486. 5. Belkin, N.L. 1982. Do reusable or disposal gowns give better protection against infection? Laundry News, 8 (2): 10, 17-18.
6. Campbell, D. 1988. Hospital Waste Management in Canada, proceeding of the national workshops on hospital waste incineration and hospital sterilization, U.S. EPA, San Francisco, C.A.
7. Manohar, D., Reddy, P.R., Kotaih, B., 1998. Characterization of solid waste of a superspeciality hospital – a case study. Ind. J. Environ. Health 40 (4), 319-326.
8. Nugget, Hospital Waste Management and Biodegradable Waste, Government of India, Press Information Bureau, http://pib.nic.in/infonug/infaug,99/i3008991.ht ml-downloaded on 25.04.2010.
9. Pandit, N.A. 1999. Study of biomedical waste management in teaching hospitals of Kashmir, P.hd thesis, Dept. of Hospital Administration, SKIMS.
10. Pruss, A., Townend, W.K. 1998. Teacher‘s Guide: Management of wastes from healthcare activities. Geneva, WHO. Pp: 160.
11. Purvi, M., sheth, K.N., Desai, H. 2006. Characterization and management of biomedical waste in SAE hospital, Anand- a case study, Electronic journal of environmental, agricultural and food chemistry, 5 (6): 1579-4377, 1583-89.
12. Rijal , K., Despande, A. 2007. Critical evaluation of biomedical waste management practices in Kathmandu valley. Proceedings of the International Conference on Sustainable Solid Waste Management. Pp: 142- 47.
13. Sharma, S., Chauhan, S.V.S. 2008. Assessment of biomedical waste management in three apex Government hospitals of Agra, 29(2): 159-162.
14. Stamenkovic, M., Kralj, D. 2007. Healthcare and waste management, WSEAS Int. Conference on energy planning, energy saving, environmental education, Arcachon, France. Pp: 116-19.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





