IJCRR - 4(10), May, 2012
Pages: 13-18
Date of Publication: 25-May-2012
Print Article
Download XML Download PDF
ORTHODONTIC TREATMENT NEEDS AMONG SCHOOL CHILDREN IN CHENNAI- A PILOT STUDY
Author: S.K.Balaji, C.K.Dilip Kumar
Category: Healthcare
Abstract:India lacks baseline epidemiologic data on the prevalence of malocclusion and orthodontic treatment needs among school children. Considering the fact that there is an urgent need for more epidemiologic data in this field we conducted this study in the suburban areas of Chennai. Objective: To assess the prevalence of malocclusion and orthodontic treatment needs among school children in the age group of 11 to 14 years. Materials and Methods: The study was conducted in school children in the age range of 11 to 14 years across 4 schools in the sub urban area of Chennai .1001 school students in age range of 11-14 years (Mean-12.75), comprising of 614 males (61.3%) and 387 females (38.7%) were screened for Crowding, Open bite ,Deep bite, Cross bite, Angle?s Class I Malocclusion, Angle?s Class II Malocclusion and Angle?s Class III Malocclusion. Results: The results from our study indicates nearly 73.2% of thesubjects had malocclusion out of which 88.3% had Class I malocclusion. Most of the subjects had crowding followed by deep bite. Conclusion: The data obtained in this pilot study will serve as baseline data for future studies in an Indian scenario and more importantly the results of our study can be used to other developing nations and .We also propose that the Indian population with its inherent diversity can serve as a reference population to study the multifactorial influences in the development and course of various malocclusions. Also these facts can validate all the indices which have been developed as we have studied the pattern at a more descriptive level
Full Text:
INTRODUCTION
Early recognition of developing malocclusions can help to minimize or eliminate future invasive or costly treatment. It also gives if necessary the option of growth modification .Many children have orthodontic problems which develop at a young age. Parents are also aware and conscious that the orthodontic problems need to be treated. Although most orthodontic problems are best treated with traditional brackets and some problems need to be treated as soon as they are noticed. Suresh babu et al and KM Shivakumar et al in 2006 and 2009 stated that 19.9% and 20.1% of school children had malocclusion ranging from definite to handicapping malocclusion requiring elective to mandatory type of orthodontic treatment1,2,3 . Considering the fact that there is an urgent need for more epidemiologic data in this field we conducted this pilot study in the suburban areas of Chennai, as the children and especially their parents in these areas do not have adequate knowledge ,facility and mainly the finance to identify and treat malocclusion.
OBJECTIVE:
To assess the prevalence of malocclusion and orthodontic treatment needs among school children in the age group of 11 to 14 years.
MATERIALS AND METHODS
The study was conducted in school children in the age range of 11 to 14 years across 4 schools in the sub urban areas of Chennai. Permission was obtained from the Institutional Ethics Committee to conduct the study . The children who had or who were having orthodontic treatment including those on interceptive orthodontics were excluded from the study. Consent forms printed both in english and local language were given to the students for their parent?s consent. 1001 school students in age range of 11-14 years (Mean-12.75) comprising of 614 males (61.3%) and 387 females (38.7%) were screened. The interview and examination of a single study subject took 3 to 4 minutes and parameters was recorded in a proforma. A comprehensive oral examination was carried out on all subjects by well calibrated dental team and recorded the following parameters namely
- Crowding
- Open bite
- Deep bite
- Cross bite
- Angles Class I Malocclusion
- Angles Class II Malocclusion
- Angles Class III Malocclusion
STASTICAL ANALYSIS
The Mean value and frequency distribution for various parameters was assessed, significance of association between various parameters was assessed using Chi - Square test (x2 ) . Data was analyzed using software Statistical Package for Social Sciences for Windows (SPSS Inc., version 15).
RESULTS
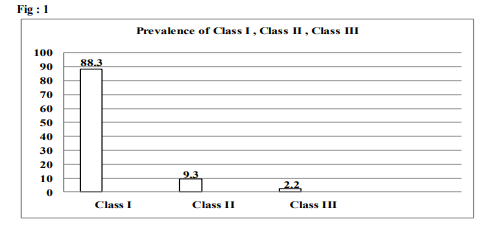
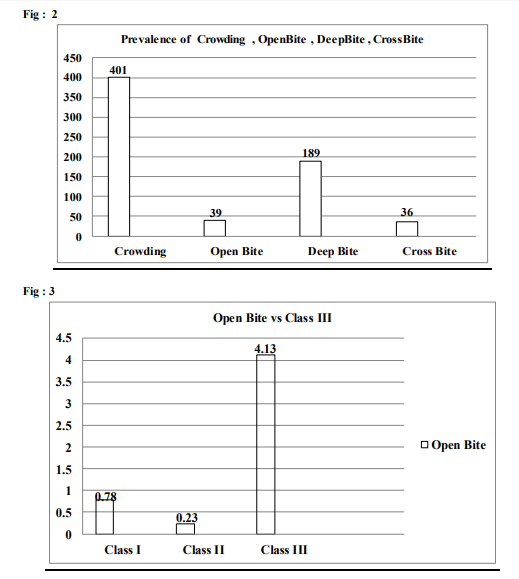
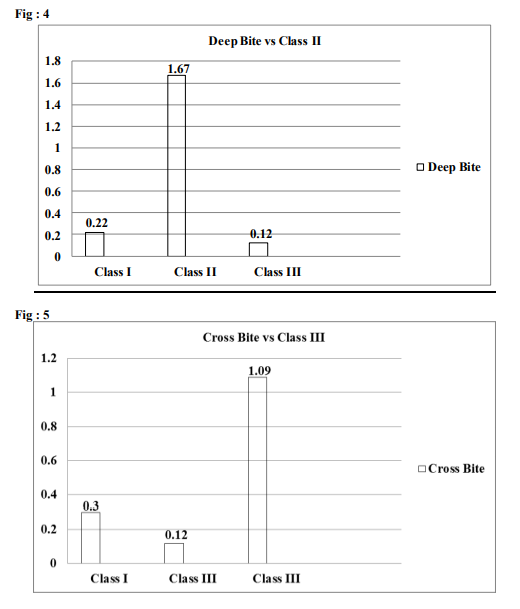
Subjects in the age group of 13 years were found to have the highest prevalence of malocclusion. The overall prevalence of malocclusion was 73.2%, out of which the prevalence of the CLASS I, CLASS II, CLASS III are summarized in Fig 1. The prevalence of various parameters assessed are tabulated in Fig 2. Prevalance of crowding, openbite, crossbite, deepbite - Fig 2 Open bite vs Class III Subjects who had class III malocclusion were found to be 4.13 times at a higher risk to develop open bite and this association was found to be statistically significant (p value =0.017) - Fig 3 Deep bite vs Class II Among subjects who had class II malocclusion only deep bite showed a statistically significant association (p value =0.038). Subjects with class II malocclusion were found to be 1.67 times more prone to develop deep bite as compared to other subjects - Fig 4 Cross bite vs Class III Subjects who had class III malocclusion were found to be 1.09 times at a higher risk to develop cross bite and this association was found to be statistically significant (p value =0.011) - Fig 5
DISCUSSION
Malocclusion is not a single entity but rather a collection of situations, each in itself constituting a problem, and any of these situations can be complicated by a multitude of genetic and environmental causes3. Guidance of the eruption and development of the primary and permanent dentitions is an integral part of the care of pediatric patients. Such guidance should contribute to the development of a permanent dentition that is in a harmonious, functional and esthetically acceptable occlusion Large number of studies have suggested that children have developed a relative degree of awareness of orthodontic treatment needs .The trends in the studies seems to suggest that though the subjects are aware of their malocclusion traits, they do not perceive a need for treatment to the same extent as a dentist or an orthodontist along with the cost concerns 4,5,6. Age, gender and socio-economic background are also thought to play a role in the perception of malocclusion, with females and higher social class individuals considered to be more critical of their dental aesthetics. 7,8,9 Lately , occlusal indices have been formulated in order to categorize the treatment of malocclusion into groups according to the importance and need for treatment. The Index of Orthodontic Treatment Need (IOTN) ranks malocclusion on the basis of the significance of various occlusal traits for dental health and aesthetic components.
The index incorporates a dental health component (DHC) based on the recommendations of the Swedish medical board11 and an aesthetic component (AC) 10, 11, 12 The purpose of this study is to provide information about the prevalence of malocclusion and orthodontic treatment needs among 11-14 years old school going children. Though, assessment of malocclusion in nongrowing population is more reliable, this age range (11-14 yrs) was considered because it represents the majority of school children with developing malocclusion who require orthodontic treatment. The results from our study indicates nearly 73.2% of the subjects had malocclusion out of which 88.3% had Class I malocclusion. Most of the subjects had crowding followed by deep bite. The prevalence of malocclusion in our study is much higher than reports from previous studies clearly suggesting that the ethnic and socio economic background along with a strong trait differs as far as malocclusion is concerned and it throws light on the fact that such studies should be conducted at every state and region level especially in a vast country like India with its varied geography, ethnicity, religion and seasonal background. To the best of our knowledge this is the first study conducted in Tamil Nadu that gives a comprehensive overview of status and prevalence of malocclusion .The data obtained in this pilot study will serve as baseline data for future studies in an Indian scenario and more importantly the results of our study can be used to other developing nations .We also propose that the Indian population with its inherent diversity can serve as a reference population to study the multifactorial influences in the development and course of various malocclusions. Also these facts can validate all the indices which have been developed as we have studied the pattern at a more descriptive level .Our study will help establish guidelines for prevention and care targeted towards the population of developing countries. The assessment of malocclusion and treatment needs is necessary to plan for orthodontic treatment and training programs for specialists.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript . The authors are also grateful to authors / editors / publishers of all those articles , journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Sureshbabu AM, Chandu GN, Shafiulla MD. Prevalence of malocclusion and orthodontic treatment needs among 13 - 15 year old school going children of Davangere city, Karnataka, India. J Indian Assoc Public Health Dent 2005;6:32-5.
2. Shivakumar KM, Chandu GN, Subba Reddy VV, Shafiulla MD. Prevalence of malocclusion and orthodontic treatment needs among middle and high school children of Davangere city, India by using Dental Aesthetic Index. J Indian Soc Pedod Prev Dent 2009;27:211-8
3. KM Shivakumar GN Chandu, and MD Shafiulla Severity of Malocclusion and Orthodontic Treatment Needs among 12- to 15-Year-Old School Children of Davangere District, Karnataka, IndiaEur J Dent. 2010 July; 4(3): 298–307.
4. Lindsay SJE, Hodgkins JFW. Children?s perceptions of their own malocclusions. Br J Orthod 1983; 10: 13–20.
5. Roberts EE, Beales JG, Dixon L, Willcocks AJ, Willmott DR. The orthodontic condition and treatment status of a sample of 14-yearold children in North Derbyshire. Commun Dent Hlth 1989; 6: 249–256.
6. Tulloch JFC, Shaw WC, Smith A. A comparison of attitudes towards orthodontic treatment in British and American communities. Am J Orthod1984; 85: 253– 259.
7. Mandall NA, McCord JF, Blinkhorn AS, Worthigton HV, O?Brien KD. Perceived aesthetic impact of malocclusion and oral self-perception in 14–15 year-old Asian and Caucasian children in Greater Manchester. Eur J Orthod 1999; 21: 175– 183.
8. Shaw WC, O?Brien KD, Richmond S. Quality control in orthodontics: factors influencing the receipt of orthodontic treatment. Br Dent J 1991;170: 66–68.
9. Jenkins PM., Feldman BS, Stirrups DR. The effect of social class and dental features on referrals for orthodontic advice and treatment. Br J Orthod 1984; 11: 185–188.
10. Otuyemi OD, Jones SP. Assessing and grading malocclusion: a review.Austr Orthod J 1995; 14: 21–27.
11. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod 1989; 11(3): 309– 320.
12. Evans R, Shaw WC. Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod 1987;9: 314– 318.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





