IJCRR - 4(12), June, 2012
Pages: 168-176
Date of Publication: 22-Jun-2012
Print Article
Download XML Download PDF
SCREENING OF SUBCLINICAL SENSORY IMPAIRMENT IN HAND AMONG DIABETIC BLINDS
Author: Janakiraman Balamurugan, Ravichandran Hariharasudhan
Category: Healthcare
Abstract:Background: Prior to hand rehabilitation of blinds with diabetic retinopathy, assessment of tactual deficits is the key towards the functional outcomes of rehabilitation. Force sensitivity threshold and spatial resolution testing are easy tools in detecting subclinical impairment of peripheral nerves. Both are reliable, less expensive, very accurate and less time consuming in detecting sensory deficits. This study
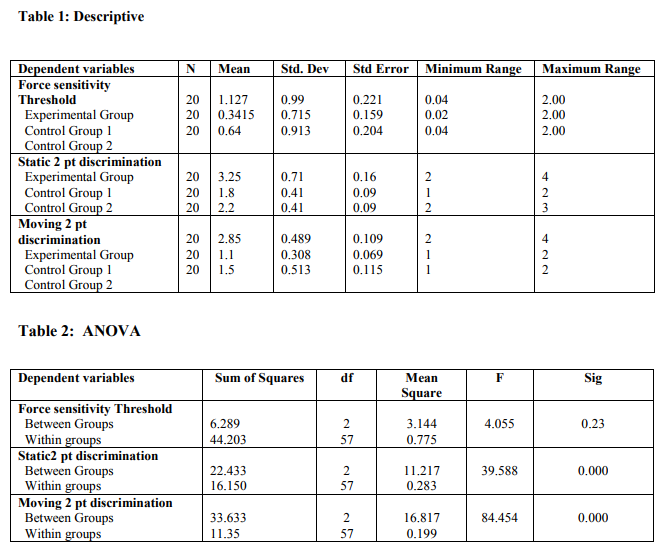
attempts to use force sensitivity threshold and spatial resolution testing to identify subclinical sensory impairment in hand among diabetic blinds. Objectives: To identify subclinical diabetic peripheral neuropathy in late blind adult subjects with diabetic retinopathy. Study Design: Observational study. Study Setting: Opthalmology and Endocrine departments of Madha Medical College and Hospital, Chennai and Sree Balaji Medical College Hospital, Chennai. Interventions: Not applicable. Outcome measures: Quantitative parameters include cutaneous force threshold and spatial resolution threshold. Methods: Sixty participants of three different categories, twenty in each category, participated in the study. The 20 subjects of each group (Diabetic blind group, Non Diabetic late blinds, and Blind folded sighted group) were subjected to force sensitivity threshold test and tactile spatial resolution test after obtaining consent. Statistical Analysis: The data was analyzed using one way ANOVA and Kruskal Wallis test, 5% level of probability was used to indicate statistical significance Result: The mean of force sensitivity among Experimental group consisting of diabetic blinds was 1.127gm, (S.D: 0.99, range: 0.04-
2.00), mean of spatial resolution capacity of static 2 point test was 3.25mm, (S.D: 0.76, range: 2 - 4), moving 2 point test was 2.85mm (S.D: 0.489, range: 2 - 4). Control group 1, mean force sensitivity was 0.3415gm, (S.D: 0.715, range: 0.02-2.00), mean of spatial resolution capacity of static 2 point test was 1.80mm, (S.D: 0.41, range: 1 - 2), moving 2 point test was 1.10mm (S.D: 0.308, range: 1 - 2). Control group 2, mean force sensitivity was 0.64gm, (S.D: 0.91355, range: 0.04-2.00), mean of spatial resolution
capacity of static 2 point test was 2.20mm, (S.D: 0.41, range: 2 - 3), moving 2 point test was 1.50mm (S.D: 0.513, range: 1 - 2). Conclusion: The study result shows that there is a significant difference between the groups. Diabetic blinds performed significantly poorer than the controls in terms of Force sensitivity threshold and spatial resolution.
Keywords: Diabetic retinopathy, Diabetic neuropathy, Monofilament testing, Two Point discrimination tests, hand rehabilitation.
Full Text:
INTRODUCTION
Sense of touch is a critical component of normal tactile hand function and provides us the ability to effectively perceive and manipulate the environment with our hand28. Diabetic retinopathy is an ocular neurovascular complication which has emerged as one of the fore most cause of blindness 20 years ago7, 21 . The age of onset for Diabetes mellitus has also gone down considerably so, people who get Diabetes early in their life is at greater risk of developing Diabetic neuropathy4 . Paramedic those who dealt with diabetic blinds has reported that tactual disturbances caused by Diabetic peripheral neuropathy is a major impedance and residual tactile sensitivity is an important predictor of outcomes of hand rehabilitation5, 27 . It‘s very important to understand that in subjects with total or partial visual compromise, the sensorimotor ability of hand will determine the quality of life and degree of independence6 . So the re-education and rehabilitation of the diabetic blinds is banked on their intact sensory cues and sensory integrity 18. There are only few studies that have really emphasized focus on addressing the sensory deficits of upper extremities in Indian diabetic subject. In contrast more studies were love on more sensorimotor function of the lower extremities in diabetic subjects8 . In order of decreasing sensitivity for two point discrimination, the tongue was found to be most sensitive, followed by the lips, fingers, palm, toes, forehead16(Weber‘s and Weinstein 1968)17. Motor control alone doesn‘t ensure skilful use of hand; rather, the synthesis of movement and sensitivity endows the hand with its exquisite abilities9 . So, greater the loss of sensibility the more significantly the hand function is impaired1 . The static and moving two point discrimination tests are tests of innervations density to find out the ability to discriminate between two identical stimuli placed close together on the skin2 . The monofilament discrimination test assesses the threshold of stimulus necessary for the perception of light touch to deep pressure and its value in detecting early nerve changes3 . Sensory deficits precedes the clinical onset of Peripheral neuropathy in Diabetes Mellitus subjects (Ozaki I 2001)26. To build a pre evaluation test battery is essential towards the special challenges faced by blindness rehabilitation professionals10. This study quantifies sensibility deficits in diabetic blinds.
MATERIALS AND METHODS
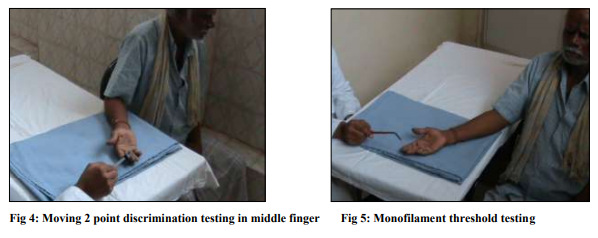
All the subjects were approached through private advertisement and through demographic data collected from various eye and diabetic rehabilitation centres. A total of 60 subjects of three different categories were approached for their consent to participate in the study after their willingness, the subjects were explained about the procedures of screening after inclusion and exclusion criteria‘s were done. All 60 subjects were right handed, both sex and with age limit of 55 – 65 years. The data collection was done in Madha college of physiotherapy. Inclusion criteria for, Experimental Group (diabetic blinds) are total duration of diabetes > 15 years, duration of blindness ≥ 5 years11, for Control Group 1 (Non Diabetic late blind) was subjects without Diabetes mellitus as a cause for blindness. Inclusion for Control Group 2 (Blind folded sighted subjects) was Non-Diabetic sighted subjects. Exclusion criteria for all groups were previously diagnosed Peripheral neuropathy25 , any systemic or regional diseases affecting sensory functions, Cervical disc disease or spondylosis, radiculopathies, any central nervous system disorders, Cognitive disorders15,24 . Among the three groups the Diabetic blind group contains 20 diabetic late blind subjects with the cause of blindness was diagnosed by Physician as Diabetic retinopathy, the period of blindness being 5 years. The other two group i.e., Late blind group contains 20 non diabetic blind adult subjects and normal blinded sighted group contains 20 subjects. In keeping with BellKorotsky testing procedures 5 set monofilaments of different colour like Blue, Purple, Orange, Light red, and Dark red of increasing diameters was used to assess / evaluate the force threshold sensitivity of subjects in their finger pads in their right hand12. Cutaneous force sensitivity threshold were measured in grams. The patient‘s hand is fully supported and vision occluded (control group 2). The subject is instructed to give a verbal response when the filament is felt. The stimuli were applied with sufficient force to just produce skin deformation13. Static and moving two point discrimination test was then performed in sitting position, with the right hand supported on a table and vision occluded using a discrimination device the millimeter calibrations of the device is checked for its validity22. The device has adjustable ends so the width between the ends was varied in millimeter increments. One or Two points were randomly applied parallel to the longitudinal axis of finger pulps13, 25. To eliminate the subject ability to guess the answers almost/at most care was taken to ensure that 2 point was applied at same time and with equal force14. The subjects were instructed to respond by verbal answers, if the subject were not able to accurately detect two points, the width between the points is increased until the two points were perceived30. To acquire accuracy and reliability the sensory testing requires concentration by the patient and should be performed in a great distraction free environment19 .
STATISTICAL ANALYSIS AND RESULTS
For statistical calculations, the mean of force sensitivity threshold and spatial resolution of three groups was used. The results were evaluated with one way Analysis of variance/ Non – parametric Kruskal wallis test were done with the help of SPSS package 1.4 for windows. The mean of Experimental Group consisting of Diabetic blinds was 1.127gm, (S.D – 0.99, range- 0.04-2.00), mean of spatial resolution capacity of static 2 point discrimination test was 3.25mm, (S.D – 0.76, range- 2 - 4), moving 2 point discrimination test was 2.85mm (S.D – 0.489, range- 2 - 4). Control Group 1, mean force sensitivity was 0.3415gm, (S.D – 0.715, range- 0.02-2.00), mean of spatial resolution capacity of static 2 point discrimination test was 1.80mm, (S.D – 0.41, range- 1 - 2), moving 2 point discrimination test was 1.10mm (S.D – 0.308, range- 1 - 2). Control Group 2, mean force sensitivity was 0.64gm, (S.D-0.91355, range0.04-2.00), mean of spatial resolution capacity of static 2 point discrimination test was 2.20mm, (S.D – 0.41, range- 2 - 3), moving 2 point discrimination test was 1.50mm (S.D – 0.513, range- 1 – 2) (Table 1). There is a significant difference when comparing Diabetic blind group with the Non diabetic late blind group and Blind folded sighted groups. The significance was set as P < 0.01. This significance existed in both Force threshold and spatial resolution testing methods, implies that Diabetic blinds are bilaterally prone to loss of tactile sensation along with the blindness caused by retinopathy, while the data‘s of blindfolded sighted subjects and non diabetic late blinds were kept as the reference values.
DISCUSSION
Diabetic retinopathy is responsible for 4.8% of the 37 million cases of blindness due to eye diseases throughout the world i.e. 1.8 million persons (WHO 2010 released to IAPB). The evaluation of hand sensation is of paramount importance in guiding the hand rehabilitation outcomes among Diabetic retinopathy blinds. It assesses the patient's current ability of tactile functions and forms a basis for constructing an effective screening tool and hand rehabilitation approach for Diabetic blind subjects, who mostly relies on their dominant hand in future for their object localisation and identification. The current study clearly shows that there is significant evidence suggestive of detectable sensory impairment in diabetic blind adults prior to the appearance of clinical symptoms of peripheral neuropathy. Interestingly Table 1 shows that non diabetic blinds are more sensitive to cutaneous force sensitivity and more spatially accurate than the control group 2. The same has been supported by Daniel Goldreich et al (2003). This noteworthy tendency is attributed to the increased manual experience in the non diabetic blind controls, which resulted in sensory enhancement effect and shows statistical significance Bernbaum et al (1989). Though the tools used in current study possess high reliability and validity, the slightest limitation of this study would be the usage of 5 set nylon monofilaments; future studies can be performed with multiple fraction sets like a 14 set monofilament to easily identify subclinical sensory impairment in diabetic patients so as to prevent complications.
CONCLUSION
This study with the statistical results (figure 1) concludes that diabetic blinds are also impeded by peripheral neuropathic changes in the upper limb nerves, along with Diabetic retinopathy. This may pose a mammoth challenge for hand rehabilitation professionals, treating these subjects. Both cutaneous force sensitivity threshold and spatial resolution testing have proved to be very reliable in identifying the subclinical changes in the peripheral nerves of Diabetic blind subjects.
CLINICAL IMPLICATIONS
Early diagnosis helps prevention and improves prognosis. So to develop a sensory evaluation tools to identify sensory impairment sustained by diabetic blind subjects due to upper limb peripheral neuropathy, which is important to hand rehabilitation professionals to develop a appropriate prevention program and rehabilitation protocol.
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited in references of this manuscript. The authors are also grateful to editors, reviewers and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. We are also indebted to the following people for their support, guidance, patience and willingness to share their time and expertise. Prof. V. Anandh, Principal, Saveetha college of PT for his moral support. Mr.S.Nagaraj and P.Anandha raja Asst Professors Madha college of PT for their constructive comments. We humbly acknowledge Dr. Karim, HOD, Opthalmology dept, Sree Balaji Medical college and Hospital for his immense contribution by guiding us to get patients. support and encouragements.
References:
1. Von Prince K and Butler, B. Measuringsensory function of hand in peripheral nerve injuries, American journal of Occupational therapy, 6: 385, 1967.
2. American society for surgery of the hand: The hand examination and diagnosis, ed. Z, Churchill Livingstone, Newyork, 1983, Page-106.
3. Bell-Krotoski;- Jand Tomana K.L: The repeatability of testing with Semmes Weinstein Monofilaments, Journal of hand surgery 12A (11): 155, 1987.
4. Martin JH, ?Receptor physiology and submodality coding in the somatic sensory system?, Principles of neural science, 2nd edition, Elsevier, Newyork, 1985, Pg- 287- 300.
5. Dellon, AL, ?Evaluation of sensibility and reeducation of sensation in the hand?, Williams and Wilkins, Baltimore, 1981, Pg: 29.
6. Dr. Rajiv Gupta, "Diabetes in India: Current Status" Express Health Care Magazine, August 2008.
7. A Ramachandran, AK Das et al, "Current Status of Diabetes in India and Need for Novel Therapeutic Agents", JAPI, June 2010, V0l: 58, Pg No:7 – 9.
8. Dr Aravind,"Diabetic retinopathy screening", Vol. 6 No.9 August and September 2010.
9. Saumya Paul et al, "Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetic Study (SN–DREAMS III): Study design and research methodology", BMC, Optholmology, Vol:7, 2011.
10. Mcintyre AK, ?Cutaneous receptors; The physiology of Peripheral nerve disease?,WB Saunders, Philodelphia, 1980.
11. Kandel, ER, ?Central representation of touch: Principles of neural science? 2nd edition, Elsevier, New York, 195, Pg: 323- 325.
12. Werner JL et al, ?Evaluating cutaneous pressure sensation of the hand?, American journal of occup ther, 24: 347, 1970.
13. Bell JA, ?Light touch-deep pressure testing using Semme Weinstein monofilaments?, Rehabilitation of hand, 3rd edition, CV Mosby, Philodelphia, 1990, pp: 585-593.
14. American society for surgery of the hand, ?The hand examination and diagnosis?, 2nd edition, Churchill livingstone, Newyork, 1983, pp:106.
15. Louis et al, ?Evaluation of normal values of for stationary and moving two point discrimination in the hand?,J Hans surg, 9A,(4),552, 1984.
16. Bell Krotoski j and Tomanak, ?The repeatability of testing with Semmes – Weinstein monofilaments?, J hand surg, 12A (11):155, 1987.
17. Levin SL, et al, ?Von frey's method of measuring pressure sensibility in the hand? J hand surg, 3(3), 211, 1978.
18. American Diabetes Association. Diabetes 2001: vital statistics. Washington (DC): American Diabetes Association; 2002.
19. Perkins BA. Diabetic neuropathy: a review emphasizing diagnostic methods. Clin Neurophysiol 2003; 114:1167-75.
20. Rahman M. How peripheral neuropathy should be assessed in people with diabetes in primary care A population-based comparison of four measures. Diabet Med 2003,20:368-74.
21. Bernbaum M, Albert SG, McGarry JD. Diabetic neuropathy and Braille ability. Arch Neurol 1989;46:1179-81.
22. Casanova JE, Casanova JS, Young MJ. Hand function in patients with diabetes mellitus. South Med J 1991;84:1111-3. 23. Lederman SJ. Tactual roughness perception: spatial and temporal determinants. Can J Psychol 1983;37:498- 511.
24. Turvey MT. Dynamic touch. Am Psychol 1996;51:1134-52.
25. Gibson JJ. The senses considered as perceptual systems.Boston:Houghton Mifflin;1966.
26. Moberg E. Criticism and study of methods for examining sensibility in the hand, Neurology 1962;12:8-19.
27. Oldfield RC. The assessment and analysis of handedness. The Edinburgh Inventory. Neuropsychologia 1971; 9:97-113.
28. Lamb GD, Tactile discrimination of textured surfaces:psychophysical performance measurements in humans. J Physiol 1983; 338:551-65.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





