IJCRR - 4(12), June, 2012
Pages: 87-93
Date of Publication: 22-Jun-2012
Print Article
Download XML Download PDF
SOLITARY BONE CYST AN INCIDENTAL FINDING DURING ROUTINE ORTHODONTIC EVALUATION A CASE REPORT
Author: Anila Charles, Sangeetha Duraisamy, Herald J Sherlin
Category: Healthcare
Abstract:Solitary bone cyst is a non-epithelial lined cyst occurring frequently in the long bones and occasionally in
the jaw bone. This cyst is most commonly located in mandibular posterior region and incidence rate is higher in the second decade of life. Clinically the cyst is asymptomatic in the majority of cases and is often accidentally discovered during routine radiological examination. Panoramic radiograph is a routine diagnostic radiograph used in the orthodontic patients. The lesion is manifested in Orthopantomograms (OPG) as a well defined unilocular radiolucent lesion with characteristic scalloping of the border when extending between the roots of the teeth. The definite diagnosis of solitary bone cyst is achieved during surgery when an empty bone cavity or cavity filled with a straw colored fluid without epithelial lining is observed. Careful curettage of the lesion favors progressive bone regeneration, offering a good prognosis and an almost negligible relapse rate. A case of incidental finding of solitary bone cyst in the routine radiographic investigation of an orthodontic patient is presented.
Keywords: Solitary bone cyst, incidental finding, orthodontic diagnosis, Orthopantomograms
Full Text:
INTRODUCTION
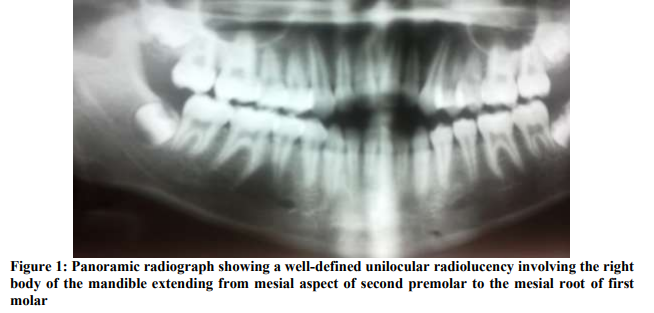
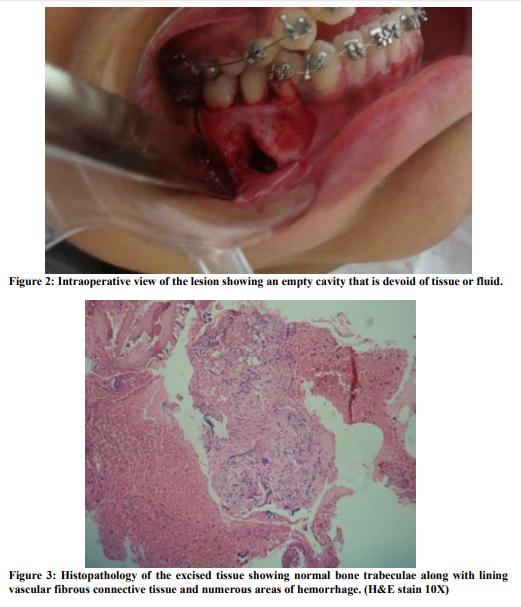
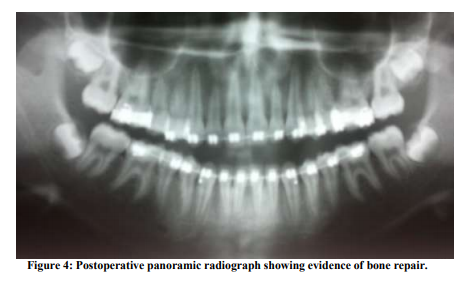
Lateral cephalogram and Orthopantomograms are commonly used diagnostic radiographs for orthodontic treatment planning.1,2 It has been reported in the literature that more than 90% of orthodontists advice these radiographs routinely for orthodontic diagnosis. 3 Solitary bone cysts are fluid-filled or empty intra-osseous lesions found frequently in the mandible and rarely in the maxilla. Commonly used names include simple bone cyst, traumatic bone cyst, hemorrhagic bone cyst and unicameral bone cyst, extravasation cyst, idiopathic bone cyst, and primary bone cyst.4,5 The solitary bone cyst is described in the WHO classification as a non-neoplastic osseous lesion because of lack of epithelial lining.6 The prevalence of solitary bone cyst is estimated to be 1% of the jaw cyst with a sex predilection for males.7 The solitary bone cyst is most frequently diagnosed in the second decade of life with age distribution ranging from 25 to 75 years.4,8,9 In an evaluation carried out on 26 cases of TBC, 30.77% had trauma history, 69.23% had some relation to orthodontic treatment, and 50% of all cases had been diagnosed during initial orthodontic documentation. 10 Positive history of trauma is frequently associated with solitary bone cyst and is regarded as an etiological factor in the development of the lesion. The cyst is usually asymptomatic and majority of the cases are diagnosed as an incidental finding in the radiographs, while in few cases pain and swelling may be a presenting symptom.11,12 Other unusual symptoms include tooth sensitivity, labial paresthesia, fistulas, and delayed eruption of permanent teeth adjacent to the cyst and displacement of the inferior dental canal.11,4,9,12,13,14 The associated teeth are usually vital without any mobility or displacement. The lamina dura may or may not be lost and occasional root resorption may occur.11,15,16,4,8,9 Occasionally the bony cavity is filled with sero-sanguineous or serous fluid. In majority of the cases no visible lining was seen, rarely a thin membrane, granulation tissue or blood clot was described. 11,17,15,4,8 Since the specimen available for the histopathological is scant, confirming the diagnosis by histopathological examination is often difficult. The lining of the cyst is a loose vascular fibrous tissue membrane of variable thickness with no epithelial lining, although fragments of fibrin, red cells, hemosiderin pigment and scattered small multinucleate cells are often found. The adjacent bone is normal or sometimes shows osteoclastic resorption on its inner surface. 18,4,8,12,19 The following is a case report of a solitary bone cyst which was diagnosed as an incidental finding in the routine diagnostic radiographs. Case report A Sixteen year old Indian female patient reported to a private dental clinic with a complaint of protruded teeth and unaesthetic smile. On profile examination, an orthognathic profile with normal nasolabial angle, mentolabial sulcus and chin were present. Intraoral examination revealed a constricted maxilla with bilateral posterior cross bite and anterior open bite. Intraoral hard tissue and soft tissue examination did not reveal any significant findings. Lateral cephalogram and panoramic radiograph (OPG) were advised as a part of routine orthodontic diagnostic investigation. Panoramic radiograph revealed a well-defined unilocular radiolucency of 1.5cm x 2cm involving the right body of the mandible extending from mesial aspect of second premolar to the mesial root of first molar. (Fig 1) There were no clinical signs and symptoms like pain or swelling and no cortical expansion noted in the region of the cyst. Patient history does not reveal any trauma related to the orofacial region. The teeth involved were asymptomatic without any pain or mobility. The clinical diagnosis suggested includes odontogenic keratocyst and lateral periodontal cyst. Pulp testing confirmed the vitality of the teeth involved excluding the possibility of cysts of pulpal origin. Following radiographic examination needle aspiration of the lesion was done which was negative. Since the lesion was asymptomatic and patient‘s primary concern was inability to bite, an non extraction treatment plan was decided based on cephalometric and model analysis findings sparing the tooth involving the lesion. Orthodontic treatment was initiated with 0.22? slot Roth prescription pre adjusted edgewise. Under local anesthesia a triangular mucoperiosteal flap from the mandibular first premolar region to the second molar region was reflected. Using a small, round surgical bur and electric drill, the exposed cortical bone was removed between the second premolar and first molar, and the cavity was entered with an explorer through the small bur hole. An empty cavity was encountered that was devoid of tissue or fluid, and there was no evidence of lining tissue on the walls. (Fig 2) The hole was gradually enlarged and careful curettage of the inner part of the buccal cortex was performed in a vertical manner. Small chips of bone along with the soft tissue fragments obtained during the surgery were sent for histopathological examination. The operative findings were strongly suggestive of solitary bone cyst; therefore, no further treatment was performed apart from curettage. The cavity was irrigated and aspiration dried allowing blood to fill the cavity, and the mucoperiosteal flap was sutured to its original position. Sutures were removed after one week and healing was uneventful. The histopathological examination revealed normal bone trabeculae along with lining vascular fibrous connective tissue. Numerous areas of hemorrhage, extravasated RBCs and resorbing bone were also found. (Fig 3) Since the surgical and histopathological diagnoses were consistent with that of solitary bone cyst no further treatment was indicated. Postoperative recalls and vitality tests for the involved teeth were performed at frequent intervals. Panoramic radiographs 6 months after the surgical intervention revealed evidence of bone repair. (Fig 4) DISCUSSION The diagnosis in this present case is well documented radiographically and histopathologically. Most of the clinical and radiographic characteristics were typical of solitary bone cyst. Panoramic radiograph is the most commonly requested radiograph in the dental practice since various hard tissue and soft tissue pathologies can be detected 20. In orthodontic diagnosis panoramic radiograph is used to detect the clinically missing teeth, presence of impacted supernumerary teeth, to evaluate the periodontal status, eruption patterns and the status of impacted third molars.21 Almost 95% of cases reported in the literature are seen in the posterior region of the mandibular body and symphysis. Fewer cases are reported in the ramus, condyle and the maxilla, predominantly in the anterior part.4,8,18,19,22 Studies have shown that the 8.7% of patients undergoing orthodontic treatment are diagnosed with pathology or abnormality as an incidental finding during pretreatment panoramic radiographs. The most common incidental findings include idiopathic osteosclerosis, thickening of mucosal lining in maxillary sinus, periapical granuloma, cysts, marginal bone loss and odontomas. Certain incidental findings like idiopathic osteosclerosis and thickening of sinus lining do not require any intervention. Cysts, odontomas and periapical inflammatory lesions require management regardless of the orthodontic treatment.26 In radiographs the cyst appears as a radiolucent area with an irregular but definite outline with or without bone condensation in the periphery. Scalloping is a prominent feature of solitary bone cysts especially when the cyst envelops the roots of the erupted teeth. Occasionally expansion of the cortical plate is observed.4, 23 Numbers of theories have been proposed for the pathogenesis of the solitary bone cyst. The most widely accepted explanation is based upon the traumatic etiology.15 According to this theory, there is a failure of organization of the blood clot with resultant degeneration of the clot producing an empty cavity within the bone. Other theories include low-grade infection, intra-osseous vascular abnormalities, degeneration of bony tumours and local alteration of bone metabolism.8,12 Accurate radiographic interpretation and diagnosis is essential 21 to suggest the finding. Although some bone cysts resolve spontaneously surgical intervention is usually indicated not only for confirming the diagnosis, but also because the simple exploration of the cyst may be curative. Therefore, curettage of the cyst wall is generally indicated. Careful curettage of the cystic lining without causing damage to the dental roots or inferior alveolar nerve results in uneventful healing and resolution of the cyst in most of the cases. Hemorrhage in the bone cavity results in clot formation and normal healing15,18,4,8,24,25 Osseous regeneration can be verified after some months, which was also observed in the described case. Accurate pulp vitality tests supported by good-quality roentgenograms are necessary to determine whether the lesion is pulpal in origin, requiring endodontic therapy. CONCLUSION Incidental findings are more common during routine orthodontic diagnostic procedures and diligent care needs to be employed in assessing any changes during the treatment, as these asymptomatic cysts are detected only by radiographic examination. Surgical intervention should be done to prevent further expansion of the cyst. Periodic assessment of the tooth and cystic region help patients avoid subsequent complications.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Morris CR, Steed DL, Jacoby JJ: Traumatic bone cysts. J Oral Surg 1970; 28:188-195
2. Nolan PJ, West KS, Lovett CR. The clinical examination. In: McNamara JA Jr, Burdon WL, eds. Orthodontics and Dentofacial Orthopedics. Ann Arbor, Mich: Needham press Inc; 2001:13-30.
3. Atchison K. Radiographic examinations of orthodontic educators and practitioners. J Dent Educ 1986; 50:651-655.
4. Hansen L, Sapone J, Sproat R: Traumatic bone cysts of jaws. Report of sixty-six cases. Oral Surg 1974; 37:899-910.
5. Mervyn Shear, Paul Speight. Cysts of the Oral and Maxillofacial Regions. Fourth edition. Blackwell and Munksguard
6. Kulberg A, Norton L. Pathologic findings in orthodontic radiographic images. Am J Orthod Dentofacial Orthop. 2003; 123:182- 184.
7. Saito Y, Hoshina Y, Nagamine T, Nakajima T, Suzuki M, Hayashi T. Simple bone cyst. A clinical and histopathologic study of fifteen cases. Oral Surg Oral Med Oral Pathol 1992; 74:487-91
8. Huebner G, Turlington E: So-called traumatic (hemorrhagic) bone cysts of the jaws. Oral Surg 1971; 31:354-365.
9. Forssell K, Forssell H, Happonen RP, Neva M: Simple bone cyst – Review of the literature and analysis of 23 cases. Int J Oral Maxillofac Surg 1988; 17:21-24.
10. Guerra ENdS, Damante JH, Janson GRP. Relação entre o tratamento ortodôntico e o diagnóstico do cisto ósseo traumático. R Dental Press Ortodon Ortop Facial. 2003; 8:41-8
11. MacDonald-Jankowski D: Traumatic bone cysts in the jaws of a Hong Kong Chinese population. Clinical Radiology 1995; 50:787-791.
12. Beasley JD: Traumatic cyst of the jaws: report of 30 cases. J Am Dent Assoc 1955; 92:145-152.
13. Curran J, Kennett S, Young A: Traumatic (hemorrhagic) bone cyst of the mandible: report of an unusual case. J Can Dent Assoc 1973; 39:853-855.
14. Hughes C: Hemorrhagic bone cyst and pathologic fracture of the mandible: a case report. J Oral Surg 1969; 27:345-346.
15. Harnet JC, Lombardi T, Klewansky P, Rieger J, Tempe MH, Clavert JM. Solitary bone cyst of the jaws: a review of the etiopathogenic hypotheses. J Oral Maxillofac Surg. 2008;66:2345-8
16. Whinery JG: Progressive bone cavities of the mandible. Oral Surg Oral Med Oral Pathol 1955; 8:903-916.
17. Rushton M: Solitary bone cysts in the mandible. Br Dent J 1946; 81:37-49.
18. Kaugars G, Cale A: Traumatic bone cyst. Oral Surg 1987; 63:318-323.
19. Kuttenberger J, Farmand M, Stoss H: Recurrence of a solitary bone cyst of the mandibular condyle in a bone graft. Oral Surg Oral Med Oral Pathol 1992; 74:550- 556.
20. Bruks A, Enberg K, Nordqvist I, Stockel HA, Janson L, Svensson B. Radiographic examinations as an aid to orthodontic diagnosis and treatment planning. Swed Dent J 1999; 23:77-85.
21. Kulberg A, Norton L. Pathologic findings in orthodontic radiographic images. Am J Orthod Dentofacial Orthop. 2003; 123:182- 184.
22. Winer RA, Doku HC: Traumatic bone cyst in the maxilla. Oral Surg Oral Med Oral Pathol 1978; 46:367-370.
23. Howe GL: "Hemorrhagic cysts" of the mandible. Br J Oral Surg 1965; 3:55-91.
24. Ruprecht A, Reid J: Simple bone cyst: report of two cases. Oral Surg 1975, 39:826-832.
25. Feinberg SE, Finkelstein M, Page HL, Dembo J: Recurrent "traumatic" bone cysts of the mandible. Oral Surg 1984; 57:418- 422.
26. Lars Bondemark, Malin Jeppsson, Lina Lindh-Ingildsen, Klara Rangne. Incidental Findings of Pathology and Abnormality in Pretreatment Orthodontic Panoramic Radiographs. Angle Orthod 2006; 76:98– 102.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





