IJCRR - 8(21), November, 2016
Pages: 35-37
Print Article
Download XML Download PDF
POSTPARTUM ACUTE KIDNEY INJURY: FALLING TREND IN DEVELOPING WORLD
Author: Nikunj Navadiya, Hina V. Oza, Pallavi Ninama, Hafsa Vohra
Category: Healthcare
Abstract:Aims and Objectives: To study epidemiological factors, risk factors, morbidity and mortality among patients in postpartum period having acute kidney injury at a tertiary care centre. Materials and Methods: This is a Retrospective Study based on obstetric patients with oliguria/anuria or referred for high s.creatinine to Civil Hospital, Ahmadabad, Gujarat, India from July 2014 to January 2015. Details of these patients like history, examination and investigation findings were recorded and final data analysis done. Results: All of the patients with postpartum AKI had oliguria/anuria and /or high serum creatinine. Most of the patients were anaemic. Most of the AKI occurred in early (< 24 hours after delivery) postpartum period. Dialysis was required in majority of the patients. Sepsis was the cause of death in these patients; mortality was higher among patients who delivered at home.
Conclusions: Postpartum kidney injury is usually a consequence of obstetric complications. In our study, most common etiological factor was puerperal sepsis and it was the cause for morbidity and mortality so the priorities in managing AKI should include early recognition, institution of appropriate preventive measures, identification and treatment of cause, timely initiation of renal replacement therapy.
Keywords: AKI-acute kidney injury
Full Text:
INTRODUCTION
Post-partum acute kidney injury (AKI) is a challenging health problem in pregnant women, especially in the developing countries. The incidence of AKI requiring dialysis in pregnancy is approximately one in 20,000 births in developed countries. But pregnancy is still responsible for 9–25% of total AKI cases in developing countries[1-3].The marked decline in this complication over the past 50 years is a result of improved antenatal care, advancements in obstetric practice and legalization of abortion. Acute kidney injury associated with late obstetrical complications is well described in literature in developed countries but the data on postpartum AKI from India is limited[4-6]. Therefore, this study was designed to study the incidence and clinical spectrum of maternal outcomes of AKI in postpartum period. Hypertensive disorders during pregnancy, Antepartum hemorrhage, Post-partum hemorrhage, HELLP syndrome and puerperal sepsis are considered to be the major causes of post-partum AKI. Although the incidence of AKI has declined sharply in the past 40 years in developed countries, its prevalence is still significant in the developing countries.
MATERIALS AND METHODS
- Study type: Retrospective study
- No. of patients: n=36
- Institute: B. J. Medical College, Civil Hospital, Ahmedabad, Gujarat, India.
- Exclusion criteria: -Obstetric patients having chronic renal failure,
-AKI associated with non-obstetric conditions.
- The obstetrical outcomes studied:
- Postpartum maternal morbidity and mortality.
- Study period: Between July 2014 to January 2015.
- AKI was defined based on changes in serum creatinine or changes in urine output or both.
- Obstetric records including age, parity data, pregnancy-related disorders and delivery information were recorded. The post-partum course was also reviewed, with specific attention to post-partum complications and timing of recovery of kidney function. RESULTS
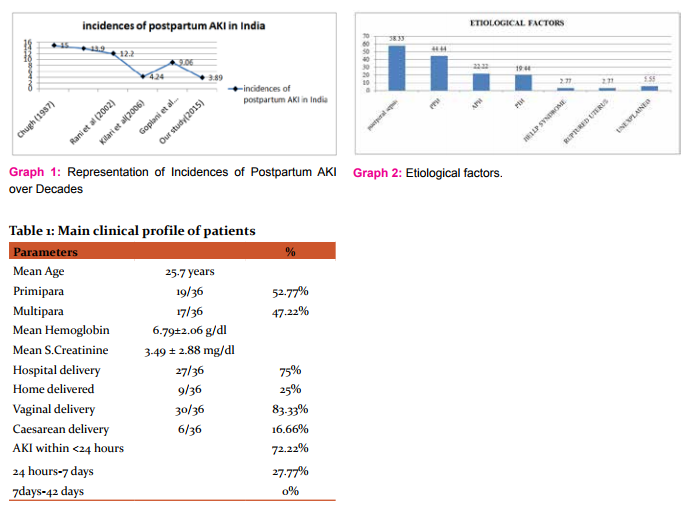
- Incidence of postpartum acute kidney injury was 3.89 % in our study.
- Mean age was 25.7years. Majority of the patients belonged to the peak reproductive age ranged between 20 and 30 years. Primipara and multipara constituted 52.77% and 47.22 % of the patients, respectively.
- Most of the patients were anemic and mean hemoglobin concentration was 6.79±2.06 g/dl.
- The mean peak serum creatinine and blood urea concentration were 3.49 ± 2.88 mg/dl and 96.24 ± 37.21 respectively.
- Mode of delivery was vaginal delivery in 30 (83.33%) patients and caesarean section in 6 patients (16.66%). Most of the patients developed AKI in early (<24 hours of delivery) postpartum period 26(72.22%), 10(27.77%) patients developed AKI between 24hrs to 7days, 0 patients had in late postpartum period (7 to 42 days). The main clinical profile of patients is shown in Table 1.
- In this study, the predominant etiology was puerperal sepsis (58.33%) followed by postpartum haemorrhage (44.44%), Hypertensive disorders of pregnancy (19.44%), antepartum haemorrhage (22.22%), HELLP Syndrome (2.77%), ruptured uterus (2.77%), unexplained(5.55%). The etiology of AKI is shown in Graph 2.
- Dialysis was required in 80.55% patients, of which 55.55% patients recovered completely.
- In the present study, mortality rate was 18.5%, sepsis being the cause of death in these patients. Mortality was higher among patients with home delivery.
DISCUSSION
- Obstetrical AKI is now a rare entity in the developed countries. The incidence of AKI in pregnancy has drastically decreased in the past 50 years from 20 to 40 % in 1960 to <10% in recent studies due to meticulous antenatal management. The incidence of pregnancy-related AKI in developed countries is 1–2.8%[7,8].
- Though the incidences of AKI in pregnancy are on a declining trend in developing countries including India, it is still prevalent in certain regions of the developing countries. Recent epidemiological studies have confirmed the decreasing incidence of PRAKI in India, with a decrease from 14.5% in 1987 to 4.3% in 2005[9,10]. The incidence still remains at 9–25%, mostly due to late referral for pregnancy related complications. In our study the incidence of postpartum kidney injury is 3.89%. The incidence of pregnancy related acute kidney injury in India among various studies is shown in Graph 1.
- AKI in pregnancy affects peak reproductive age group. Mean age of patient in our study were 25.7 years. Similar observations with respect to age of pregnant women was reported by other workers[11,12]
- Sepsis accounted for post-partum AKI in 58.33% of our study subjects. Similar to our observation, Ansari et al. reported puerperal sepsis in 31% of AKI during pregnancy[12], Kumar et al. reported puerperal sepsis in 29% of patient in PRAKI, Goplani et al noted puerperal sepsis as the most common (61%) etiology of post-partum AKI in their study[11]. Patients with sepsis present with generalized vasodilation, which causes renal hypo perfusion and, consequently, renal injury.
- In our study, uterine haemorrhage was the dominant(67%) cause of AKI, Similar to our study uterine haemorrhage was the dominant cause of PRAKI in the studies by Naqvi et al (58%), Ansari et al (38%), and Alexopoulos et al (38%)[3,12,15].In contrast to our observation, Kumar et al. observed that haemorrhage of pregnancy constitutes 17% of PRAKI[13].
- PIH was reported as the cause of AKI in 50% of cases in the series of Grünfeld et al[4], Hachim et al. reported preeclampsia and eclampsia in 41 of 55 (74.5%) cases as main etiology of PRAKI[14].We observed PIH as a cause of AKI in 19.44% of patients.
- Dialysis was required in 80.55% of patients in our study. Of them, 55.55% completely recovered on dialysis. The need for dialysis was reported in 70–100% of cases in other series as well.
- Maternal Mortality of AKI seems to be high in developing countries. Overall, maternal mortality was 18.5% in our study. Previously, mortality was very high (55.3%) due to poor antenatal care, late referral, frequent sepsis. Reported mortality from other studies varies from 23 to 33%[6,12,15].
CONCLUSION
- Postpartum kidney injury is usually a consequence of obstetric complications. In our study, most common etiological factors were puerperal sepsis and uterine hemorrhage, and they accounted for most of the morbidity and mortality.
- Routine antenatal care and institutional delivery should be provided to every pregnant woman.
- Priorities in managing AKI should include early recognition, institution of appropriate preventive measures, identification and treatment of underlying cause, and timely initiation of renal replacement therapy.
ACKNOWLEDGEMENT
This Research paper is made possible through help and support from my Professors, Seniors, Friends and Hospital staffs. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
CONFLICT OF INTEREST – NONE DECLARED
ETHICAL APPROVAL – NOT REQUIRED
FUNDING- NONE
References:
- Chugh KS, Singhal PC, Sharma BK, et al. Acute renal failure of obstetric origin. ObstetGynecol 1976;48:642-6.
- Prakash J, Singh RG, Tripathi K, et al. Acute renal failure in pregnancy. J ObstetGynaecol India 1985;35:233-8.
- Naqvi R, Akhtar F, Ahmed E, et al. Acute renal failure of obstetrical origin during 1994 at one centre. Ren Fail 1996;18:681-
- Grunfeld JP, Ganeval D, Bourneris F. Acute renal failure in pregnancy. Kidney Int.1980;18:179–191
- SelcukNY, Tonbul HZ, San A, Odabas AR. Changes in frequency of acute renal failure in pregnancy (1980-1997)Ren Fail 1998;20:513-7.
- Prakash J, Niwas SS, Parekh A, et al. Acute kidney injury in late pregnancy in developing countries. Ren Fail 2010;32:309-13
- Stratta P, Besso L, Canavese C, et al. Is pregnancy-related acute renal failure a disappearing clinical entity? Ren Fail.1996;18:575–584
- Brady HR, Clarkson MR, Lieberthal W. Acute renal failure.In: Brenner BM, ed. The Kidney. 7th ed. Philadelphia, PA:Saunders; 2000:1215–1270.
- Chugh KS. Etiopathogenesis of acute renal failure in the tropics.AnnNatlAcad Med Sci (India) l987;23: 88-99
- Chugh S, Sakhuja V, Malhotra HS et al. Changing trends in acute renal failure in third world countries—Chandigarh study. Q J Med 1989; 272: 1117–23.
- Goplani KR, Shah PR, Gera DN, et al. Pregnancy related acute renal failure: a single centre experience. Indian J Nephrol 2008;18:7–21.
- Ansari MR, Laghari MS, Solangi KB, et al. Acute renal failure in pregnancy: One year observational study at Liaquat University Hospital, Hyderabad. J Pak Med Assoc.2008;58:61–64.
- Kumar SK, Krishna CR, Kumar VS. Pregnancy related acute renal failure. J ObstetGynecol India.2006;56:308–310.
- Hachim K, Badahi K, Benghanem M, et al. Obstetrical acute renal failure. Experience of the nephrology department, Central University Hospital ibnRochd, Casablanca. Nephrologie. 2001;22:29–31.
- Alexopoulos E, Tambakoudis P, Bili H, et al. Acute renal failure in pregnancy. Ren Fail.1993;15:609–613.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





