IJCRR - 4(13), July, 2012
Pages: 94-100
Date of Publication: 18-Jul-2012
Print Article
Download XML Download PDF
TO ASSESS THE FUNCTIONAL CAPACITY AND HEALTH STATUS OF THE STABLE CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS
Author: Vinod K. Ravaliya, Lata D. Parmar
Category: Healthcare
Abstract:Background of objectives: There are various studies in western countries suggesting that there is ignificant reduction in functional capacity and health status of stable Chronic Obstructive Pulmonary disease(COPD) patients. However, no such studies were found in Indian population to the best of our knowledge therefore, the present study was undertaken to assess the functional capacity and health status of stable COPD patients. Materials and Methods: This was a cross-sectional, observational study. 30 stable COPD participants attending outpatient department of chest medicine were compared with age matched normals with regards to demographic status, BMI, functional capacity and health status using Six minute walk test and Medical Outcome Study Short Form-36 Item Questionnaire(MOS SF-36). Results: All the participants were chronic smokers. All of them had dyspnea related to physical activities with increased work of breathing. Although 63.33% reported to have normal dietary intake with only 33.6% complaining of reduced appetite, the overall weight of the COPD participants was significantly reduced when compared to normal's. There was marked decrease in distance walked by COPD participants (mean 258.53+/-18.31 m) compared to normal's (mean 421.37+/-14.76 m). The Respiratory rate and Rate of perceived exertion of COPD group were markedly increased at p-value < 0.01 compared
to normal's, both in pre and post six minute walk test. The mean score of total health of COPD subjects (55.83+/-3.11) was markedly lower compared to normal's (95.17 \? 0.71). Also, there was significant positive correlation between six minute walk distance and MOS SF-36(r=0.499, p< 0.01) score in stable
COPD participants. Conclusion: Stable COPD subjects showed impaired functional capacity and health status compared to age matched healthy population. Strategies aiming at modifying these factors could be implemented to improve the well being of stable COPD subjects.
Keywords: Stable COPD, Functional capacity, Six minute walk test, Health status
Full Text:
INTRODUCTION
The COPD is progressive and irreversible disorder of the airway with widespread involvement of pulmonary as well as extra pulmonary systems. It is commonly associated with varying degree of dyspnea related to activities of daily living. Dyspnea having greater impact on functional capacity which is described as the ability to perform predominantly aerobic activity, a fundamental requirement for many activities of daily living that renders an individual physically inactive and sedentary. The reduction of functional capacity in turn additionally affects health status of the sufferers1 . Various studies have indicated that irreversible airway narrowing, reduced FEV1 does not improve with any medications but the functional capacity and health status have been found to show significant improvement with implementation of pulmonary rehabilitation program. Till date, to the best of our knowledge there are no studies that assess the functional capacity and health status of stable COPD patients in Indian population. Therefore the present study aimed to identify and study the problems of stable COPD patients of our area. This would help us to device and establish the strategies that would improve their quality of life.
MATERIALS AND METHODS
The study proposal was approved by the Human Research Ethical Committee of H M Patel Center for Medical Care and Education, Karamsad. The study design was hospital based, cross sectional study. Two groups of population were recruited into the study. One group consisted of participants with stable COPD diagnosed by chest physician and second group consisted of age matched normal healthy individuals (healthy as self reported and not on any medications) from the local population. In both groups, male population has been selected as no female COPD patients reported during study period in our set up. The participants with acute exacerbations of COPD, pulmonary tuberculosis, asthma, restrictive lung disease, neuromuscular dysfunctions, muscle problems of spine or lower extremities, metabolic disease, hypertension, heart failure, unstable angina, peripheral vascular disease were excluded from the study. All the participants were assessed through general format. The height was measured using wall mounted height measuring scale without footwear. The body weight (wt) was measured using weighing scale with Standard deviation of + 0.5 kg. Body mass index (BMI) was calculated as the weight (in kg) divided by square of height (in M2 ). The Six minute walk test and MOS SF-36 questionnaire were used as an outcome measures to assess the functional capacity and health status of both the groups.
Functional capacity assessment
The 6MWT was performed using standard guidelines laid down by American Thoracic Society, 2002 on a flat, straight, 30 meter long corridor of our Hospital.2,3,4 Pre test: Pulse rate, Respiratory rate, Blood pressure and Borg's rate of perceived exertion were recorded. The Borg's RPE scale was translated from English to Gujarati and showed to participants. Post test: Six minute walk distance, Borg's RPE, Pulse rate, Respiratory rate and Blood pressure was recorded. The measurement of these parameters was taken at an interval of every two minutes till the parameters returned to the baseline value.
Medical Outcomes Study Short Form-36 Item Questionnaire
The MOS SF-36 questionnaire has been used to asses self reported domain of health status. It contains major 2 components- physical health and mental health to assess quality of life. The score ranges from 0-100 with higher score representing the better health status. This questionnaire was available in English language and therefore translated into vernacular version (i.e. Gujarati).the participants were interviewed personally by the investigator and information was gathered. Approximately 10 minute duration was required to answer the questionnaire5,6,7 . Statistical analysis: The data obtained were fed into the computer in microsoft excel sheet for statistical analysis, SPSS (statistical package for social sciences)package has been used. The dependent variables of the two groups were compared using Unpaired Student's t-test at 95% confidence limit. The correlation was found between the variable of the two groups using Pearson‘s correlation.
RESULTS
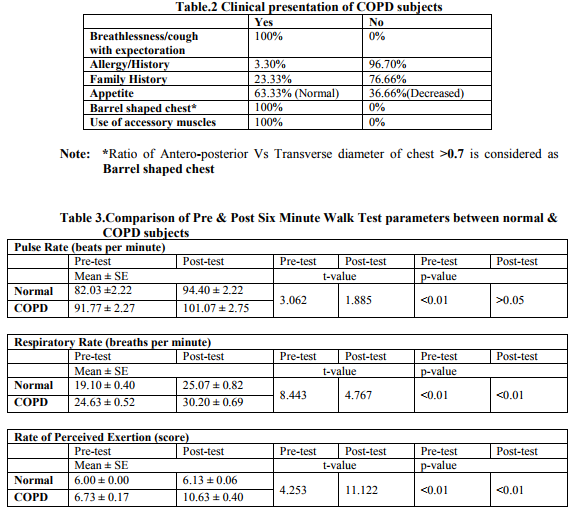
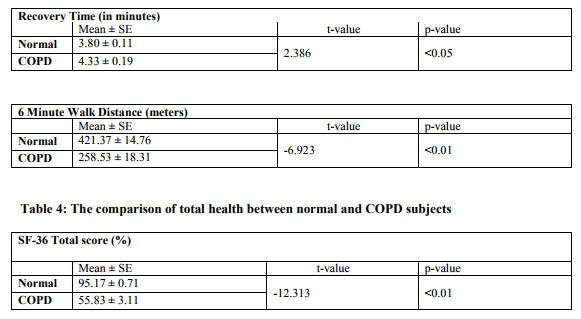
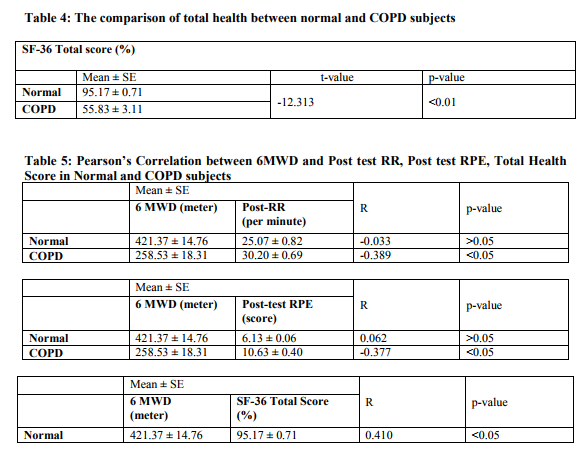
I. Table 1 and 2 indicates that the COPD participants had significant weight loss when compared to the normal‘s, although only 36.66% had complain of reduced appetite while rest of the 63.33% had normal dietary intake. Table 3: The mean value of resting PR, RR, BP and Borg's RPE of the study group was much higher than control group which was statistically significant at p-value <0.01. Post-test, RR and RPE showed statistically significant rise at p-value <0.01. With regards to recovery time following 6MWT, it was found that COPD subjects took longer time as compared to control group that was statistically significant at pvalue <0.05.The 6MWD was markedly reduced in COPD subjects (258.53+/-18.31) as compared to control group (421.37+/-14.76) with statistical significance at p-value<0.05. Table 4: The mean score of total health of COPD and normal subjects was 55.83 ± 3.11 and 95.17 ± 0.71 respectively . The difference between both the group was statistically highly significant at p-value<0.01. Table 5: In Pearson's Correlation analysis, posttest RR (r=-0.39, p<0.05) and post-test RPE (r=0.377, p<0.05) showed statistically significant negative correlation with 6MWD in COPD group. When SF-36 score was analysed, strong correlation was seen with 6MWD in COPD group (r=0.45, p=0.005) as compared to control group(r=0.410, p<0.05).
DISCUSSION
All the study participant were males as no female participants reported during the study period this could also possibly be explained by low prevalence of the disease in women or undiagnosed in women, also less exposure to health care services due to less dominating in gender, negligence of the disease and lastly greater occurrence in lower socioeconomic class where least importance is given to the women and women's health8 . The participants also were chronic smokers with duration exceeding 30 years which has been reported to be the approximate period to result into substantial loss of lung function to experience symptoms. All the participants in study group had dyspnea (MRC grade II-IV) as a primary symptom related to activities of daily living, barrel shaped chest, use of accessory muscles of respiration at rest. These signs are consequences of path mechanical changes of thorax in an attempt to compensate for a compromised respiratory function. When the lungs become inflated, the diaphragm gets displaced downwards, result into reduction in efficiency of contraction. These changes contribute o shortness of breath which is commonly encountered more often by COPD subjects this becomes more apparent when person with COPD performs any activity2 . Fabio Pitta et al 2005 concluded that 6MWD (< 400 mt) is the best surrogate marker of inactivity during daily life in patients with COPD9 . In the present study, 6MWD covered by the study group was 40% lesser than the normal‘s. Inactivity in COPD is not a surprising finding in itself, possibly the existence of dyspnea limit their level of physical activity. The baseline parameters were found to be higher in study group compared to control group probably due to higher BMR in patients with COPD. Immediately after 6MWT, they showed greater rise in RR and RPE, whereas no significant change occurred in circulatory response that is PR and BP. It has been agreed by various authors that mainly dyspnea which gets precipitated on walking influences RR and RPE in order to meet excessive energy requirement of body compensated by greater demand on respiratory system10. In addition to that M Decramer et al explained the peripheral muscle weakness, de conditioning and impaired gas exchange as important contributors to exercise intolerance11 .
The advancement in age is often associated with change in health status due to physical limitations and limited ability to engage in leisure time activities to some extent (Mayou et al 1990).The MOS SF-36 score of COPD group was quite lower than that of their healthy counterparts. Similar findings have been reported in various studies suggesting that it‘s a reflection of impaired functional capacity as dyspnea limit ADLs, therefore COPD subjects do not favor to socialize with people or they prefer to stay home and more often remain confined to bed12,13,14. Moreover, anxiety, depression and other factors like frequent physician visits, emergency room visits and hospitalizations for COPD have been seen to affect the health status15. Therefore, the factors contributing to dyspnea, weight loss, decreased endurance, peripheral muscle dysfunction and raised BMR should be considered to improve functional outcomes. Weight loss is an important predictor of performance of COPD subjects16. In the present study, 33% of COPD population had a reduced dietary intake and rest of them had an adequate dietary intake. Although on the whole had a drastic weight loss compared to normal subjects may be due to dyspnea related to ADL, increased resting energy expenditure, systemic inflammation, and tissue hypoxia. These patients may become short of breath in the very act of eating and so may not eat enough to replace the calories they used17, therefore, imbalance in energy ultimately reflects through weight loss significantly. Secondly, the increased resting energy expenditure may be due to an increased oxygen consumption of the respiratory muscles secondary to the increased resistive load and impaired efficiency of respiratory muscles. The poor nutritional status also has an adverse effect on the outcome irrespective of the lung functions, therefore, nutritional assessment should be made an important part of regular assessment of patients with COPD. The Cochrane database systemic reviews 2008(Y Lacasse et al) showed that an increase in 6MWD, reduction in MRC dyspnea score, enhancement of emotional function, patient's sense of control over their condition and improvement in health status occurs following pulmonary rehabilitation. The pulmonary rehabilitation targeting therapy with exercise training and nutritional intervention is found to be beneficial. It has been shown to increase functional performance independent of degree of airflow limitations. Importantly it appears that much of the improvement with exercise training is due to its effect on skeletal muscle function as well18 . The results of this study shows significant reduction in functional capacity and health status compared to control group, this should not be overlooked as although COPD is irreversible condition, there is convincing evidence that improvement in well-being of stable COPD patients occur with a structured, well planned pulmonary rehabilitation program.
CONCLUSION
The present study indicates that the functional capacity and the health status are significantly compromised in stable COPD subjects compared to age matched healthy individuals. Reduction in functional capacity is attributed to alteration of pulmonary functions based on significant increase in post test RR and RPE along with baseline reduction in PEFR and chest expansion. There was no significant rise in post test PR and BP suggestive of no affection of circulatory system. The nutritional status, indicated by weight and BMI was significantly lower in COPD patients compared to normal despite the dietary intake of 66% subjects with COPD being normal.
ACKNOWLEDGEMENT
The authors acknowledge the faculty members of K M Patel Institute of Physiotherapy and Chest medicine department, Shree Krishna Hospital, Karamsad for their valuable help. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. No Conflict of Interest
References:
1. Elisabeth Stahl, et al., Health-related quality of life is related to COPD disease severity. Health and Quality of life outcomes 2005; 3:56
2. Jerome L Fleg, Gary Balady et al., Assessment of functional capacity in clinical and research applications. American heart association, 2000; 102:1591.
3. ATS statement: Guidelines for 6 MWT. ATS Board of Directors, American journal of respiratory critical care medicine, vol 16; 111- 117, 2002
4. Wise RA, et al., Minimal clinically important differences in the 6MWT and the incremental shuttle walking test. COPD.2005; 2:125-9
5. Soyyigit S, Erk M, Guler N et al., The value of SF-36 Questionnaire for the measurement of life quality in COPD, 2006,259-266
6. Mahler DA, Mackowiak JI et al., Evaluation of the short term 36 item questionnaire to measure HRQOL in patients with COPD. Chest J, 1995; 1585-9.
7. Molfino NA, et al., Current thinking on genetics of COPD. Current Opinion Pulm Med. 2007; 13:107-13
8. Anita B Varkey, et al., chronic Obstructive Pulmonary Disease in Women: exploring gender differences. Current opinion in Pulmonary Medicine, 2004.
9. Fabio Pitta, et al., Characteristics of physical activities in daily life in COPD. AM J Crit Care Med. 2005; Vol 171; 972-977
10. Gallego MC, et al., Dyspnea in COPD: relation to the MRC scale with dyspnea induced by walking and cardiopulmonary stress testing. Arch Bronconeumol. 2002; 38: 112-6
11. M Decramer, R Gosselink, Muscle weakness is related to utilization of health care resources in COPD patients. ERJ February 1, 1997 vol. 10 no. 2 417-423
12. Hutter BO, et al., functional capacity and Quality of life in patients with COPD: instruments of assessment and methodological aspects. Pneumologie. 1999; 53:133-42.
13. Marc Miravitlles et al., Factors determining the Quality of life of patients with COPD in primary care. Therapeutic advances in Respiratory Medicine, 2007; Vol.1, No.2, 85- 92
14. Larson JL, et al., Functional performance and physical activity in COPD: theoretical perspectives. COPD. 2007; 4:237-42
15. H. Florence Seung Kim, et al., Functional impairment in COPD patients: the impact of anxiety and depression. Psychosomatics 2000; 41:465-471
16. Deveci F, et al., Nutritional status, pulmonary functions, and exercise performance in COPD cases. Tuberk Toraks 2005; 53:330-9
17. Consensus on why dyspnea occur? Am J Resp Crit C Med, 2008
18. Y Lacasse et al., Pulmonary rehabilitation for COPD. Cochrane Database of Systemic Reviews 2008 Issue 4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





