IJCRR - 4(14), July, 2012
Pages: 85-89
Date of Publication: 31-Jul-2012
Print Article
Download XML Download PDF
ARCHITECTURAL VARIATIONS ON THE EXTERNAL SURFACES OF LIVER
Author: B. Senthil Kumar, A. Anand
Category: Healthcare
Abstract:Background: In modern era of surgical advances, liver transplantations play an important role in enhancing the quality of life. Liver transplantations are now performed in many tertiary centers in our country. However in Indian population, very few studies exist regarding variations in the external architecture of liver. Aims and Objectives: To categorize the variations of external architecture of liver Materials and Methods: About 175 formalin fixed liver were utilized for the study. During routine dissection, liver was observed for architectural changes; variations in the size and shape of lobes, accessory lobes, unusual fissures, and unusual nodulated appearances were noted. Result: Varied shapes of both right and left lobes of liver were observed which included hypoplasia of left lobe, bifid caudate process, caudate lobe with papillary process , right lobe showing deep fissures, variations in the shape of Quadrate lobe, and the exit of ligamentum teres, segmented right lobe, hardened impression of ribcage on anterosuperior and lateral surfaces. Conclusion: A thorough knowledge of the architectural variations of the liver will help the surgeons while planning for surgery.
Keywords: Liver Lobes, Hypoplasia, Fissures
Full Text:
INTRODUCTION
Liver is the most important and largest gland in the human body performing various metabolic functions. It occupies most of the right hypochondrium and epigastrium, and extends into the left hypochondrial quadrants as far as the left midclavicular line. The liver has superior, anterior, right, posterior and inferior surfaces, and has a distinct inferior border. The liver is divided into right and left anatomical lobes by the falciform ligament and the fissure for ligamentum venosum. The right lobe includes quadrate and caudate lobes which are demarcated by fissures for ligamentum venosum and ligamentum teres on right side and groove for inferior vena cava and the fossa for gall bladder on left side. [1] Congenital anomalies of the human liver are usually rare. [2] It could be very high in some populations but the reason why we do not notice them very often is that these cases are usually asymptomatic. [3] There are many kinds of congenital abnormalities of the liver which have been described in literature such as agenesis of its lobes, absence of lobes, lobar atrophy, hypoplastic lobes, transposition of gall bladder and Reidel‘s lobe. [3] The knowledge of anomalies of liver is very much important for surgeons during hepatectomy and oncologists especially when they handle liver tumors and during resection of the primary or metastatic tumors. The major fissures are important for interpretation of lobar anatomy and to help locate the lesions in the liver during hepatic imaging. [4] Any defect during organogenesis of liver by mutation of transcription gene factor leads to hepatic anomalies which are divided into 2 categories like Defective development, and Excessive development. [5] The study was carried out to categorize the variations of external architecture of liver.
MATERIALS AND METHODS
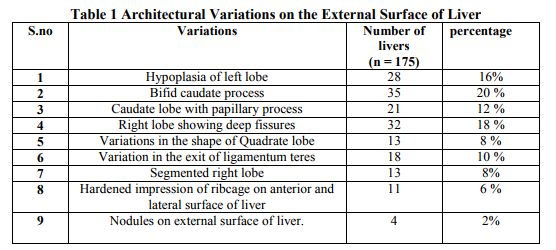
About 175 formalin fixed livers were utilized for the study with digital photographic equipment, dissecting instruments and measuring scale. During routine dissection, the abdomen was exposed, positions of the liver in all cadavers were noted, after which careful dissection was done and the liver was delivered out of the abdominal cavity and examined. Pathological specimens were excluded from the purpose of study. The liver was observed for architectural variations, variations in the size and shape of lobes, the papillary process of the liver was measured, accessory lobes, unusual fissures, unusual nodulated appearances were noted. The deep fissures were measured using a measuring scale and observed carefully for any peritoneal attachments and blood vessels deep inside these fissures. The observations were documented. RESULTS Varied shapes of both right and left lobe of liver were observed in this, hypoplasia of left lobe was 16%, bifid caudate process was 20 %, caudate lobe with papillary process was 12 %, right lobe showing deep fissures 18 %, variations in the shape of Quadrate lobe 8 is %, variation in the exit of ligamentum teres 10 %, segmented right lobe 8%, hardened impression of ribcage on anterior and lateral surface of liver 6 %, Nodules on external surface of liver 2% (Table 1).
DISCUSSION
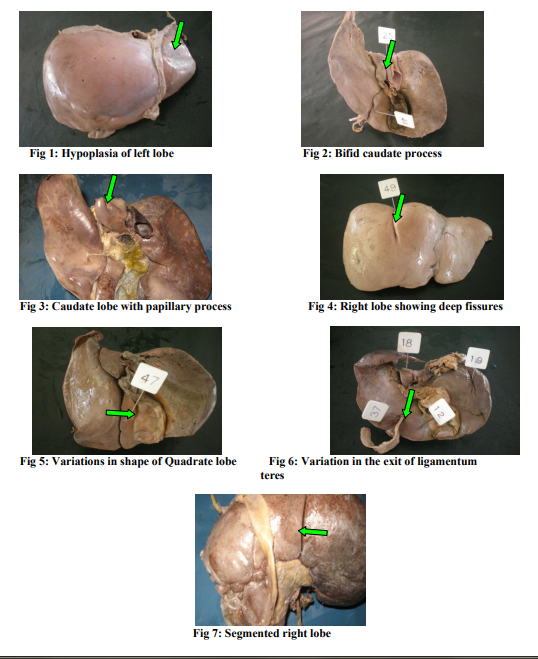
Very rarely the hepatic lobe is absent in liver which can be noticed only during the cadaveric dissection, autopsy, or on the operating table during surgery. The hepatic lobe anomalies are not always congenital. Congenital agenesis of liver lobes affect left lobe more than the right lobe of liver. [6, 7, 8] In this study the left lobe of the liver shows hypoplasia in about 16% of the dissected specimens (Fig 1) but absence of lobes was not observed during the present study. In about 20% of dissected livers bifid caudate process was observed (Fig 2). The caudate lobe has two separate portions which are intervened by inferior vena cava, one to the left is called as Spiegel‘s lobe and the other to the right extending as caudate process is called as the paracaval portion, both parts are bridged by the caudate isthmus. Kogure et al noted the presence of notch on the inferior border of the liver in many patients undergoing hepatectomy. [9] The existence of external notch between Spiegel‘s lobe and the paracaval portion was taken as an index to separate both the portions of the caudate lobe. Sahni et al found out that the prevalence of a notch appearing decreases with advancing age. [10] The presence of an external notch continuing as vertical fissure on the caudate lobe gives a bifid appearance of the caudate process. Joshi et al reported that 33% of livers showed prominent papillary process. [4] In the present study only 12% of the dissected livers the caudate lobe showed prominent papillary process (Fig 3). The Papillary process was measured which was in a range of 4 to 5 cm. Auh et al reported that on a computed tomography even normal size or small papillary process can be misinterpreted with an enlarged hepatic lymph node whereas an enlarged papillary process mimics a pancreatic body mass when it extends to the left and displaces the body of stomach anteriorly. [11] 18% of dissected livers showed accessory deep fissures which were 3 to 4 in number on the inferior surface of the right lobe (Fig 4). Joshi et al reported that 2 to 5 accessory fissures with veins in the depth of fissure were seen on the inferior surface of the right lobe of liver. [4] In our study no such veins were observed in the depth of the fissures. Some accessory fissures were also seen prominently in the quadrate lobe. The presences of accessory fissures are a potential source of diagnostic errors during imaging. [11] The quadrate lobe showed variations in shape (8%). The various shapes included pear shape, rectangular, triangular, pointing tongue like process as reported by joshi et al. [4] In the present study, the shape varied from being pear shapes to triangular shapes (Fig 5). Some quadrate lobes showed prominent fissures and tongue like processes measuring about 1 - 2 cm which was directed towards the fossa for gall bladder. A narrow or buried or a small quadrate lobe creates confusion during radiological investigation, which can be mistaken as the fissure for ligamentum teres which will be nearer to the left margin of the fossa for gall bladder. [4] The fissure for the ligamentum teres is considered to be an important landmark for measuring the right and the left lobes. The Pons hepatis usually bridges the fissure for the ligamentum teres by joining the quadrate lobe with the left lobe. Joshi et al reported that the Pons hepatis can be seen bridging the upper third of fissure, present in depth of fissure, and completely bridging the fissure. [4] In all our cases the pons hepatis was bridging the upper two thirds of the fissure and gave the appearance as if the ligamentum teres was exiting from a tunnel (10%), and was hanging down freely which was not usually normal (Fig 6). In about 8% of dissected livers it was observed that 2 to 3 segmentations of the right lobe of liver which was due to the presence of accessory fissure on the right lobes (Fig 7) which can give rise to a false interpretation about the lobes of liver during radiological investigations. 6% of dissected livers showed hardened impressions which looked like prominent vertical grooves on the anterosuperior surface. A higher incidence of such grooves was observed by Macchi et al and Auh et al. [12, 13] According to Schafer and Symington and De Burlet (as quoted by Macchi et al), prominent vertical grooves are called as diaphragmatic sulci which results from an uneven growth of hepatic parenchyma due to variable resistance offered by different bundles of diaphragmatic muscle tissue. [12] But radiological and corrosion cast studies have attributed the formation of sulci due to the existence of weak zones of hepatic parenchyma which represent the portal fissures between adjacent portal territories. Thus these weak portions exert lower resistance to external pressure exerted by the diaphragm which can be accentuated by a prominent rib cage. These tend to be a landmark for surface projections of portal fissures and hepatic veins and its tributaries which run through them. [12] Collection of fluid in these fissures can be mistaken for liver cysts, intrahepatic hematomas or as a liver abscess [14] Nodules were also observed on the external surface of liver (2%) which has been hitherto unreported (Table 1).
CONCLUSION
Liver transplantations are being performed from blood relatives only and very rarely the donor is not a relative. The era of cadaveric liver transplantations is not far away. A thorough knowledge of architectural variations of the liver like the present study will serve as an eye opener for endocrine surgeons and surgical gastroenterologists in future.
References:
1. Standring S, Healy JC, et al. Liver. In: Standring S, ed. Gray‘s Anatomy: The Anatomical Basis of Clinical Practice. 39th ed. London: Elsevier Churchill Livingstone, 2005: 1213-25
2. Abdullahi D Zagga, Azziz A Tadros, Jibrin D Usman, Abubakar Bello. Absence of the left lobe of liver in cadaver: case report 2010; 12: 45-47.
3. Aktan ZA, Savas R, Pinar Y, Arslan O. Lobe and segment anomalies of the liver. J Anat Soc India 2001; 50: 15-16.
4. Joshi SD, Joshi SS, Anthavale SA. Some interesting observations on the surface features of the liver and their clinical implications. Singapore Med J 2009; 202(pt 3): 715-19
5. Chiba S, Suzuki T. A tongue- like projection of the left lobe in human liver, accompanied with lienorenal venous shunt and intrahepatic arterial anastomosis. Okajimas Folia Anatomica Japonica; 68(1): 51-56.
6. Demirici I, Diren HB. Computed tomography in agenesis of the right lobe of liver. Acta Radiologica 1990; 31: 105-6.
7. Kakitsubata Y, Kakitsubata S. Anomalous right lobe of the liver: Ct appearance. Gastrointest. Radiol 1991; 16: 326-28.
8. Radin DR, Colleti YF. Agenesis of the right lobe of the liver. Radiology 1987; 164: 639- 42.
9. Kogure K, Kuwano H, Fujimaki N, Makuuchi M. Relation among portal segmentation, proper hepatic vein and external notch of the caudate lobe in the human liver. Ann Surg 2000; 231: 223-28.
10. Sahni D, Jit I, Sodhi L. Gross anatomy of the caudate lobe of the liver. J Anat Soc India 2000; 49: 123-26.
11. Auh YH, Rosen A Rubenstein WA, et al. CT of the papillary process of caudate lobe of the liver. Am J Roentgenol 1984; 142: 535-38.
12. Macchi V, Feltrin G, Parenti A, De Caro R. Diaphragmatic sulci and portal fissures. J Anat 2003; 202 (pt 3): 303-8.
13. Auh YH, Rubenstein WA, Zinnsky K et al. Accessory fissures of the liver: CT and sonographic appearance. AM J Roentgenol 1984; 142: 562-72.
14. Auh YH, Lim JH, Kmim KW, et al. Loculated fluid collections in hepatic fissures and recesses: CT appearance and potential pitfalls. Radiographics 1994; 14: 529-40.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





