IJCRR - 4(14), July, 2012
Pages: 56-59
Date of Publication: 31-Jul-2012
Print Article
Download XML Download PDF
OSTEOMA OF EXTERNAL AUDITORY CANAL - A CASE REPORT
Author: Gunvanti B. Rathod, Pragnesh Parmar, R. N. Gonsai
Category: Healthcare
Abstract:Osteoma is a rare, benign, bone forming tumour which can arise from various sites in the cranial vault including temporal bone. It is a slow growing tumour. In external auditory canal, normally it is asymptomatic although it may cause cosmetic deformities. Large size osteoma of external auditory canal causes obstruction of external auditory canal along with pressure symptoms such as headache. It must be distinguished from exostosis in external auditory canal, a much common condition in that site, since there is ample clinical and histopathological evidence that these two lesions are separate entities. The purpose of the present study is to present a review of literature about external auditory canal osteoma and to report in details the case of a 10 years old female patient with the lesion and focusing on differentiating features between osteoma of external
auditory canal and exostosis.
Keywords: Osteoma, External auditory canal
Full Text:
INTRODUCTION
Osteoma of external auditory canal is a benign tumour which is often symptomless, although it may cause cosmetic deformities. Large size osteoma of external auditory canal causes obstruction of external auditory canal along with pressure symptoms such as headache. [1] Incidence of external auditory canal osteoma is 0.05 % of all otologic surgeries. Osteoma is a new bone forming tumour located within bones of cranial vault including temporal bone. In the external auditory canal, it must be distinguished from exostosis, a much more common condition in that site, since there is ample clinical and histopathological evidence that these two lesions are separate entities. [2]
Case report
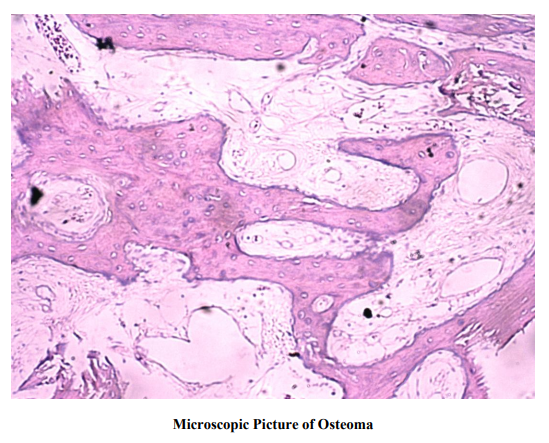
A 10 years old female patient reported with a swelling in the right external auditory canal since 1 year. It was gradually increasing in size. The patient gave history of right ear discharge since 1 month. There was no history of earache, decrease in hearing, headache, vomiting, giddiness, tinnitus, visual disturbance and neurological deficit. On examination, the swelling was found to arise from the posterior wall of the right external auditory canal. It was about 1x1 cm2 in size, smooth, bony hard, non tender swelling. Right external auditory canal was occluded by the swelling, so otoscopic examination was not possible. X-ray of chest and mastoid both were normal. The patient was undergone procedure for the excision of the tumor under local anesthesia. It was attached to bony external auditory canal and light blows were applied using a mallet on all sides of tumour to separate it and the mass was sent for histopathological examination. On gross examination, received specimen consisted of one whitish, skin covered bony hard nodular tissue, measuring 0.8 x 0.6 cm2 . It was kept for decalcification procedure and after 2 days tissue was processed for routine paraffin embedding. Then Haematoxylin and Eosin (H&E) stained sections were prepared. Microscopic examination revealed mature lamellar bony tissue with presence of intervening fibrovascular connective tissue. Bony tissue was covered by stratified squamous epithelium and overall histology was suggestive of diagnosis of osteoma. (Figure I)
DISCUSSION
Osteoma of external auditory canal is a rare benign lesion which is slowly growing and kept stable for years. [1] Osteoma has often incidental findings at examination but may cause pressure symptom such as headache. [3] It predisposes to wax collection & external otitis and hence causes a conductive hearing loss by direct or indirect meatal occlusion. [4] Important complications of osteoma in external auditory canal are mainly related to treatment and include recurrence, facial nerve affection, sigmoid sinus damage and sensorineural hearing loss, by nerve compression. [5, 6, 7, 8] During removal of anterior lesions the temporo-mandibular joint can be violated resulting in temporomandibular joint prolapse and subcutaneous emphysema secondary to air entry into the joint through a bony defect. Other complications include canal stenosis and tympanic membrane perforation. [9] Microscopically there are four types. 1) Compact: the most frequent one, comprising of dense, compact and lamellar bone, with few vessels and haversian canals. 2) Cartilaginous: It comprising of bone and cartilaginous elements. 3) Spongy: It is a rare type, comprised of spongy bone with marrow and fibrous tissue with tendency to expand the diploe and involving the internal and external lamina of the affected bone. 4) Mixed: It is mixture of spongy and compact types. [6, 10, 11, 12] Graham reported histological findings of osteoma i.e. osteoma is covered by a dense squamous epithelium with an underlying periosteum. The internal structure is characterized by a great abundance of discrete fibrovascular channels surrounded by lamellated bone. The appearance of bone between these channels varies considerably, being primarily dense and oriented in different directions. [2] The histogenesis of osteoma has still not been defined. According to congenital theory, presence of embryonic cartilage results in intensified bone growth after puberty. Friedberg suggested trauma with consequent periostitis as a predisposing factor. [13] According to hormonal theory, there is increase of the periosteal osteoblastic activity, stimulated by endocrine mechanisms which results in increased bone growth. [11] The differential diagnosis should include exostosis, osteoid osteoma, osteoblastic metastasis, eosinophilic granuloma, giant cell tumour, monostotic fibrous dysplasia. [14] Osteoid osteoma is differentiated by central nidus composed of calcified osteoid lined by plump osteoblast and growing within highly vascularized connective tissue. Giant cell tumour can be differentiated from osteoma by presence of stromal cells and osteoclast like giant cells. Monostotic fibrous dysplasia is differentiated by narrow, curved and misshaped bone trabeculae, often having characteristic fish hook configuration. Eosinophilic granuloma is characterized by presence of variable admixture of eosinophils, giant cells, neutrophils, foamy cells and areas of fibrosis. [15] It is important to differentiate osteoma from exostosis as both can produce similar clinical picture and differentiating points are as follows: Osteoma is usually solitary pedunculated lesion attached to the tympanosquamous or tympanomastoid suture lines, where as exostosis is usually multiple, bilateral broad based elevations of bone. Exostosis is thought to be a reactive condition secondary to multiple cold water immersions, or recurrent otitis externa. Ears with exostosis have been called surfer‘s ear or Australian ears as prevalence rate of 73.5% of exostosis is reported in surfing population. [16] Exostosis, in contrast to osteoma, shows parallel concentric layers of subperiosteal bone with numerous osteocytes and absent fibrovascular channels. [2, 17] Treatment for small lesions of osteoma is frequent cleaning of debris from the external auditory canal, while large lesions causing external auditory canal obstruction and hearing impairment require surgical removal.
CONCLUSION
Osteoma of external auditory canal is benign and very rare tumour having incidence rate of 0.05%. If it is small, often not producing any symptoms and purpose of surgical removal is only cosmetic deformities. Large size osteoma of external auditory canal causes obstruction of external auditory canal long with pressure symptoms such as headache. Osteoma of external auditory canal must be differentiated from exostosis. Both have only clinical similarity but incidence, prevalence, etiopathogenesis and microscopic examination all are different.
References:
1. Friedmann I, Pathological lesions of the external auditory meatus: a review, Journal of the Royal Society of Medicine, 1990, 83: 34-37.
2. Graham M.D, Osteoma and exostosis of the external auditory canal: A clinical, histopathological and scanning electron microscopic study, Annals of Otology, 1979, 88: 566-572.
3. Shenoy P., Paulose K.O., Khalifa S.A., Sharma R., Osteoma of the ear canal presenting with headache, Journal of Laryngology and Otology, 1989, 103: 683-684.
4. Phelps P.O., Scott-Brown‘s Otolaryngology, Vol. 3, Otology, 5th Edition, Butterworths, London, 1987, Page 40.
5. Camacho RR, Vicente J, Cajal SR., Imaging quis case 2, Archives of Otolaryngology, Head and Neck Surgery, 1999; 125 (3): 349, 251-352.
6. Burton DM, Gonzalez C., Mastoid osteoma, Ear Nose Throat Journal, 1991; 70(3): 161 - 162.
7. Denia A, Perez F, Canalis RR, Graham MD, Extracanalicular osteomas of the temporal bone, Archives of Otolaryngology, 1979; 105(12): 706- 709.
8. Tutor EG, Osteoma de mastoids, Anales Otorhinolaryngologicos Ibero Americanos, 1991; 18(4): 325 -330.
9. Sheehy JJ, Diffuse exostoses and osteomata of the external auditory canal: a report of 100 operations, Otolaryngology, Head and Neck Surgery, 1982; 90: 337-342.
10. Fleming JP, Osteoma of the mastoid, Canadian Journal of Surgery, 1966; 9(4): 402-405.
11. Singh I, Sanasam JC, Bhatia PL, Singh LS, Giant osteoma of the mastoid, Ear Nose throat Journal, 1979; 58(6): 243 - 245.
12. Guerin N, Chauveau E, Julien M, Dumont JM, Merignargues G., Osteome de la mastoide, A propos de deux cas, 1996; 11 (2): 127 - 132.
13. Friedberg SA, Osteoma of mastoid process, Archives of Otolaryngology, 1938; 28: 20-26.
14. Probst LE, Shankar L, Fox R., Osteoma of the mastoid bone, Journal of Otolaryngology, 1991; 20(3): 228 - 230.
15. Rosai and Ackerman, Surgical Pathology, 9th edition, Mosby, Edinburgh, 2005, Page 2137-2236.
16. Wong BJ, Cervantis W, Doyle KJ, Karamzadeh AM, Boys P, Brauel G et al., Prevalence of external auditory canal exostoses in surfers, Archives of Otolaryngology, Head and Neck Surgery, 1999; 125: 969 - 972.
17. Kemink, J.L, Graham, M.D., Osteoma and exostosis of the external auditory canal – medical and surgical management, Journal of Otolaryngology, 1982, 11(2): 101-106.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





