IJCRR - 8(21), November, 2016
Pages: 01-05
Print Article
Download XML Download PDF
CONCENTRATED GROWTH FACTOR MEMBRANE - A NOVEL BARRIER FOR ACCELERATED REPAIR OF GINGIVAL DEFECT ALONG WITH SLIDING FLAP TECHNIQUE
Author: Ramakrishnan T., Shobana P., VidyaSekhar, Nirmala J.I., Ebenezer, Sivaranjani K.
Category: Healthcare
Abstract:Aim: Periodontal regenerative procedures like root coverage procedures are still a valid treatment option for exposed root surfaces caused by gingival recession. So far, many alloplastic as well as autologous materials were used for regeneration; of which platelet was found to be having greater regenerative potentiality and several platelet aggregates were developed recently in the field of regeneration. The concentrated growth factor (CGF) is the new generation platelet aggregate; this CGF may be a valuable aid in the field of regeneration to speed up the process of healing.
Case Report: This case report elaborates the use of CGF as a barrier membrane, along with laterally displaced procedure to accelerate soft tissue healing, in lower anterior tooth (31) with class II gingival recession in a 20 years old female patient.
Discussion: Many studies about concentrated growth factor showed a great regenerative properties and versatility. Its use has been proposed in various procedures like filling the extraction socket, sinus lift procedures, moreover it can also be combined with bone grafts to accelerate bone formation.
Conclusion: The result of this case report suggested that the CGF barrier membrane has the potential to accelerate the soft tissue healing which when combined with the root coverage procedures like sliding flap technique, thus results in achieving the expected gain in the width of the attached gingival in class II Gingival recession defects.
Keywords: Concentrated Growth Factor, Gingival recession, Laterally Displaced flap
Full Text:
INTRODUCTION:
Location of the gingival margin apical to cemento-enamel junction is called Gingival recession.1 The most common cause of such mucogingival deformity is abrasive and traumatic tooth brushing habit. The recession may also be associated with high frenal attachment, minimal width or absence of attached gingiva, persistent inflammation, or root hypersensitivity which might require some form of mucogingival surgery.2 Periodontal inflammation and the resultant loss of attachment results in reduced attached gingiva, the problem is more common on the facial surfaces, but it may also occur on the lingual surface. There are various periodontal plastic surgical techniques available till date to treat these defects in order to increase the width of the attached gingiva and to improve the aesthetics. Generally treating these defects and associated mucogingival problems, by means of surgery may be best accomplished by the reestablishment of a functional zone of attached gingiva.2 Healing studies have confirmed that plastic repair of denuded root surfaces is possible when the laterally positioned flap is used, where the “bridging” phenomenon is effected by new connective tissue and epithelial attachment to the previously exposed cementum.3 The displaced pedicle flap technique was originally described by Grupe and Warren in 1956.4 This can be used to cover isolated, denuded root surfaces that have adequate donor tissue laterally. Prini Prato et al. 1992 described a technique where pedicle soft tissue graft procedures can be combined with a barrier membrane, in order to create space for tissue formation between the facial root surface and the membrane. The main objective of our procedure is to evaluate the accelerated healing efficacy of CGF membrane when combined with laterally displaced flap operation in treating a single tooth with denuded gingiva in the facial aspect. Growth factors are proteins which regulate in the complex processes of wound healing. Growth factors play a main role on cell migration, cell proliferation and angiogenesis in tissue regeneration therapy. Concentrated growth factor (CGF) was first developed by Sacco (2006). According to Professor Rodella at University of Brescia, Department of Biomedical Sciences and Biotechnologies, CGF shows higher tensile strength, more growth factors, higher viscosity and higher adhesive strength than early generation platelet concentrates like PRF (platelet rich fibrin).5
CASE REPORT:
A patient named Ms. Ranjitha 20 years old female came to our college with a chief complaint of irregularly placed front teeth and wants to align it. Patient was referred to the Department of Periodontics for oral prophylaxis. On intra oral examination 31 was found with Miller’s class II gingival recession. Coronoplasty and intentional RCT was done, Root coverage procedure in 31 was planned. The treatment plan for gingival recession was Lateral Sliding flap operation combined with CGF as the barrier membrane a novel approach.
PREPARATION OF CGF:
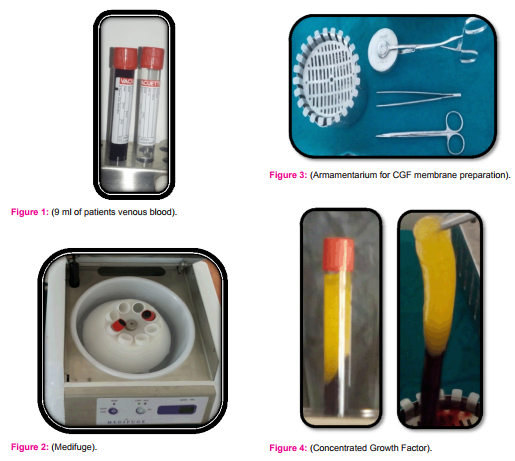
An autologous CGF material can be prepared by obtaining the patient’s venous blood samples without any anticoagulant and immediately centrifuged in a special centrifuge device (“MEDIFUGE”), at variable rpm from 2400-2700 for 12 minutes to separate the cells in the blood which results in fibrin rich blocks that are much larger, denser and richer in Growth Factor. CGF can be used as barrier membrane to accelerate soft tissue healing or can be mixed with bone graft to accelerate new bone formation.5
OPERATIVE PROCEDURE:
Patient’s venous blood of 9 ml was collected without anticoagulant [fig.1] and kept for centrifugation; [fig.2]. Later patient was immediately taken for surgery. 12 minutes after centrifugation CGF was obtained [fig.4] and it was separated from the RBC layer and kept in between the compressing disc [fig.3, 5] to get as a membrane [fig.6]. Meanwhile Patient’s recipient site preparation was done [fig.7]. The de-epithelialisation was done around the root surface. With #15 blade a vertical incision was given from the distal gingival margin of 32 including the interdental papilla extending beyond mucogingival junction and a full thickness flap was raised. The flap has to be sufficiently wider than the recipient site. A releasing incision may be needed to avoid tension on the base of the flap. Now the flap is ready to slide laterally onto the adjacent root [fig.8]. The prepared CGF membrane was placed first on the denuded root surface as a barrier membrane; [fig.9] above which the lateral pedicle flap was positioned [fig.10] and suturing done covering the CGF membrane. Aluminium foil and periodontal dressing was placed finally.
RESULT:
Three days after patient was recalled, [fig.11] no sign of infection was seen. One week post operatively suture removal was done [fig.12]. There was significant increase in the width of the attached gingiva. Evidence of Healing was good and root coverage was satisfactory at one month post operative period [fig.13].
DISCUSSION:
The advantage of sliding flap technique is that the flap has enough blood supply which paves way for better healing. With respect to the use of CGF membrane the dual coverage was provided to the exposed root surface. Concentrated growth factor was first developed by Sacco (2006).6 Platelet’s regenerative potentiality was introduced in the year 1974. Rose et al were first to describe that platelet has growth factors.7 Periodontal surgical procedures using biomaterial like platelet concentrates is a new way to accelerate and enhance the natural wound healing mechanism.8 There are some clinical and anatomic factors limiting the treatment outcome for gingival recession, so even when there is no loss of interproximal attachment and bone complete root coverage is not always achievable.9 In this case CGF membrane was exposed in certain areas which might be the reason for not achieving 100% root coverage.But healing was accelerated without any complication in unexposed areas and increase in the width of attached gingival was also achieved.
CONCLUSION
Within the limits of this present case report, the utilisation of CGF barrier membrane can be best accomplished along with lateral sliding flap technique in managing the gingival defects. This novel barrier membrane accelerates the soft tissue healing and better results can be achieved if used properly. Further studies with sufficient sample size are necessary to support this result.
ACKNOWLEDGEMENT
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.


References:
- American Academy of Periodontology. Glossary of Periodontal Terms. Chicago: American Academy of Periodontology; 2001;(4):47.
- Guinard A E, Caffesse G R. Treatment of localized gingival recessions. J Periodontol1978; 49(9):457-61.
- Smuckler H. Laterally positioned Mucoperiosteal pedicle grafts in the treatment of denuded roots. J Periodontol 1976; 47(10):590-5.
- Carranza F, Newman M, Takei H, Klokevold P. Periodontal plastic and esthetic surgery. Clinical periodontology.2015; 11:919-23.
- Sohn DS. The effect of concentrated growth factors on ridge augmentation. Implant Journal. 2009; 34-40.
- Sacco L. Lecture. International academy of Implant prosthesis and osteoconnection. 2006.12.4
- Naik B, Karunakar P, Jayadev M, Marshal RV. Role of platelet rich fibrin in wound healing: A critical review. Journal of Conservative Dentistry 2013; 16(4): 284-93.
- Khiste SV, Naik R. Platelet- Rich fibrin as a Biofuel for Tissue regeneration. ISRN Biomaterials. 2013:1-6.
- Zuchelli G, Testori T, Sanctis De M. Clinical and anatomical factors limiting treatment outcomes of gingival recession: A new method to predetermine the line of root coverage. J Periodontol2006;77(4): 714-21.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





