IJCRR - 4(19), October, 2012
Pages: 168-173
Date of Publication: 15-Oct-2012
Print Article
Download XML Download PDF
HAND GRIP STRENGTH IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Author: Almas Sirguroh, Shakeel Ahmed
Category: Healthcare
Abstract:Purpose: Skeletal muscle dysfunction is common morbidity in patients suffering from chronic obstructive pulmonary disease (COPD) with quadriceps muscle being the most severely affected and hence most research focuses on the changes occurring in the thigh muscles. Consequently not much is known about involvement of other muscles especially the ones in the arm, forearm and the hand. Hence this study aims determine whether hand grip strength is affected in patients with COPD and whether it has any correlation with patients peak expiratory flow rate(PEFR) and body mass index(BMI). Methodology: 30 patients with COPD and 30 healthy age matched controls were selected. PEFR, hand grip strength and BMI were evaluated. Results: A poor non-significant correlation was found between PEFR and hand grip strength (r =-0.153) and between BMI and hand grip strength (r = -0.179) in patients with COPD. But hand grip strength was significantly lower in patients with COPD (17.4 +/- 4.49 kg force) compared to that in controls (28.43 +/- 8.35 kg force) (p =0.00). Similarly COPD patients had significantly lesser BMI (19.08+/- 4.08 kg/m2) compared to the controls (27.67+/- 4.15 kg/m2) (p =0.00). Conclusion: Hand grip strength is reduced in patients with COPD but does not correlate with severity of obstruction as measured by PEFR or with BMI.
Full Text:
INTRODUCTION
Chronic Obstructive Pulmonary Disease (COPD) is a major cause of health concern worldwide and one of the leading causes of death that is increasing in prevalence1. Prevalence of COPD is very high in India. In a study done across various centers where a total population of 35295 individuals was assessed, the prevalence was found to be 4.1%2. Along with impairments such as dyspnea, increased work of breathing, decreased efficiency of muscles of inspiration, COPD is also associated with various local and systemic complications including cachexia, weight loss, osteoporosis, skeletal muscle dysfunction, cardiac failure, atherosclerosis, dementia and depression3,4. A major reason for morbidities and mortality seen in patients with COPD are these extra pulmonary manifestations. Out of the above mentioned manifestations, skeletal muscle dysfunction is the most predominant complication contributing to early onset of fatigue and exercise intolerance. The consequences of exercise intolerance include increased difficulty in performing activities of daily living and difficulty participating in everyday events5 . Changes observed in the skeletal muscles include reductions in type I fibers, atrophy of type I and II fibers, reduced capillarity density, and altered metabolic enzymelevels3,4 . Various factors have been identified as contributing to skeletal muscle changes, which include hypoxia, hypercapnia, inflammation, nutrition, deconditioning, and steroid-induced myopathy5 . This systemic manifestation of muscle dysfunction is most commonly observed in large muscles, especially the quadriceps and the current literature suggests that quadriceps weakness is found in about 32% - 43% patients suffering from COPD7 . Most of the research focuses on changes occurring in the quadriceps and very less emphasis has been given to investigate changes occurring in other peripheral muscles especially the muscles of the upper extremity especially wrist and intrinsic muscles of the hand. Hence this study is aimed at determining whether hand grip strength is affected in patients suffering from COPD and whether the severity of airway obstruction correlates with the hand grip strength.
MATERIALS AND METHODS
This was a case control study with a sample size of 60 which included 30 patients suffering from COPD and 30 age matched controls selected. Cases of the study were patients suffering from Chronic Obstructive Pulmonary Disease (COPD) admitted in the respiratory medicine ward of Sassoon General Hospital, Pune. Ethical clearance to conduct the study was obtained and subjects were recruited using convenience sampling. The Controls were also selected by convenience sampling and matched using individual matching. Patients and controls of both genders were included. In the group of COPD Patients, patients requiring supplemental oxygen or mechanical ventilatory support, Patients in acute exacerbation of COPD, patients with history of inflammatory joint disease affecting the dominant upper limb, neurological disorders affecting the upper extremities, History of fracture of the dominant upper limb, History of pain radiating from neck to fingers of dominant upper extremity and history of diabetes mellitus were excluded. Similarly, in the control group, individuals, with known history of respiratory disease, history of diabetes mellitus, history of trauma to the dominant upper limb and individuals with a history of neurological disorders affecting the upper limb were excluded. Outcome Measures 1. Hand Grip strength in Kg force 2. Peak Expiratory Flow Rate (PEFR) in liters/min 3. Body Mass Index (BMI) in Kg/m2 Procedure Prior to evaluation, each Subject’s written Informed Consent to participate in the study was obtained. Patient’s weight and height were checked. The PEFR of COPD patients was measured using a Wright’s Peak flow meter as per the guidelines prescribed by the American Thoracic Society8 . Hand grip strength was measured in all sixty subjects using a Jamar Hand held dynamometer. Prior to testing, the procedure was explained to the subjects followed by a demonstration of the technique. Grip strength of the dominant hand was evaluated. The Subjects were asked to sit on a chair with the back erect, with feet flat on the floor and were asked to look forward. The dynamometer was secured to the patient’s hand using a wrist strap. The test position had the subjects placing their arms by their side with elbow flexed to 90 degrees, forearm in mid prone and the wrist in neutral position. The Subjects were asked to hold the dynamometer in the hand and were instructed to attempt squeezing with maximal effort following which the hand grip in Kg force was noted down. Subjects were instructed to maintain their position during testing and advised not to brace the arm against their side or recruit other muscle groups by flexing or extending the elbow beyond 90 degrees or move the arm and do any trick movements. Three trials were taken with a rest period of one minute between each trial and the best of the three values was used for data analysis.
DATA ANALYSIS
Data was analyzed using SPSS version 18. Pearson’s correlation was used to correlate PEFR with hand grip strength and BMI with hand grip strength in patients with COPD. Paired T test was used to compare hand grip strength and BMI between patients with COPD and controls.
RESULTS
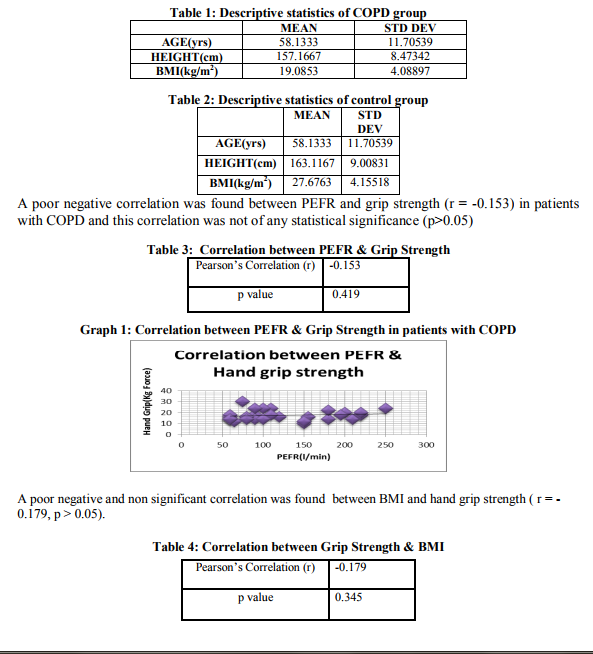
Descriptive statistics of COPD group and controls are given in table 1 and table 2.
DISCUSSION
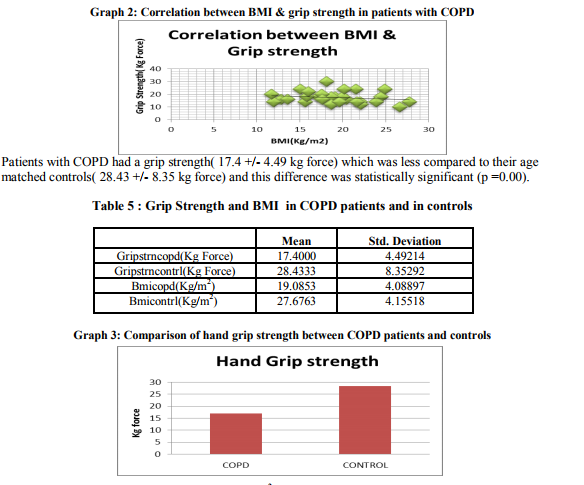
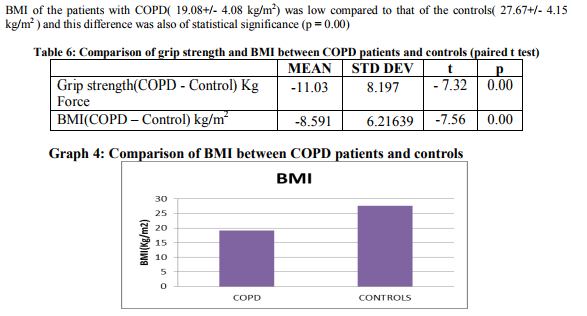
In this study we found a very weak negative correlation between severity of airway obstruction as measured by PEFR and hand grip strength and between BMI and hand grip strength. The fact that muscles of the upper extremity are not subject to the effects of physical inactivity as demonstrated by earlier done research on muscles such as the deltoid, adductor pollicis which did not show biopsy changes found in quadriceps muscles3,9,10,11 supports the weak insignificant correlation between severity of the disease and outcomes like BMI and hand grip strength. Peripheral muscle dysfunction is probably the most extensively studied systemic effect of COPD with emphasis mainly on the involvement of the thigh muscles. Along with the structural changes in the muscles, physical inactivity is also found to play a role in augmenting the dysfunction. Though these changes have the most pronounced effects on the quadriceps, it has been found that even muscles of the upper extremity in patients with COPD demonstrate considerable weakness compared to the muscles of their healthy counterparts12. But muscles such as adductor pollicis, the pectoralis major and latissimus dorsi which are recruited in almost every activity of daily living are not as weak as the inactive muscles, such as quadriceps & vastus lateralis3,9,10,11,12 . Though hand grip evaluation is primarily an assessment of the muscles of the hand and the wrist, muscles of the shoulder girdle are recruited during the maneuver to stabilize the shoulder girdle 13,14.Hand grip was also found to be significantly reduced in patients with COPD. This is supported by the findings of Sarah Bernard et al, who found that muscles of the upper extremity in patients with COPD are weak compared to healthy individuals12 . BMI of COPD patients was significantly lesser compared to the controls. Patients with COPD often lose weight during the course of their disease. It is hypothesized that this may be due to skeletal muscle apoptosis15 .Loss of skeletal muscle mass is reflected by the reduction in fat-free mass (FFM) observed in 20–40% of patients with COPD 15, 16, 17.
CONCLUSION
We conclude that though hand grip strength is affected in patients with COPD, it does not correlate with severity of airway obstruction and body composition of the patients.
LIMITATIONS OF THE STUDY
The limitations of the study were that the controls were not selected by random sampling and outcomes assessing the strength and specific functions of the muscles of the upper extremity were not used.
RECOMMENDATIONS
Though hand grip strength did not correlate with airway obstruction in patients suffering from chronic obstructive pulmonary disease, it was much weaker compared to that of healthy individuals. Hence on the basis of this study we recommend addition of hand grip strengthening exercises in pulmonary rehabilitation programs devised for patients with chronic obstructive pulmonary disease.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all articles, journals and books from where the literature for this article has been reviewed and discussed. Authors would also like to thank the Department of Respiratory Medicine, Sassoon Hospital, Pune, for granting them permission to conduct this study in their premises and M.A Rangoonwala College of Physiotherapy and Research, Pune for providing access to their peak flow meter and hand held dynamometer.
References:
1. Hurd S. The impact of COPD in lung health worldwide: Epidemiology and incidence. Chest 2000; 117: 1S-4S.
2. Jindal SK, Aggarwal AN, Chaudhry K, Chhabra SK,D’Souza GA, Gupta D, et al. Asthma Epidemiology Study Group. A multi centric study on epidemiology of chronic obstructive pulmonary disease and its relationship with tobacco smoking and environmental tobacco smoke exposure. Indian J Chest Dis Allied Sci 2006; 48: 23-7.
3. P.J. Barnesand B.R. Celli Systemic manifestations and co morbidities of COPD,Eur Respir J 2009; 33: 1165–1185
4. M Jeffery Mador and Erkan Bozkanat Skeletal muscle dysfunction in chronic obstructive pulmonary disease Respir Res 2001, 2:216–224
5. Gosselink R, Troosters T, Decramer M. Exercise training in COPD patients: the basic questions. Eur Respir J 1997; 10:2884–2891
6. C. Coronel, M. Orozco-Levi, R. Mendez, A. Ramirez-Sarmiento, J.B. Galdiz,J. Gea; Relevance of assessing quadriceps endurance in patients with COPD. Eur Respir J 2004; 24: 129–136
7. J.M. Seymour, M.A. Spruit, N.S. Hopkinson, S.A. Natanek. The prevalence of quadriceps weakness in COPD and the relationship with disease Severity. Eur Respir J 2010; 36: 81– 88
8. M.R. Miller, J. Hankinson, V. Brusasco, F. Burgos, R. Casaburi, A. Coates,et al, Standardisation of spirometry, Eur Respir J 2005; 26: 319–338
9. W D-C Man, N S Hopkinson, F Harraf, D Nikoletou, M I Polkey, J Moxham: Abdominal muscle and quadriceps strength in chronic obstructive pulmonary disease. Thorax 2005; 60:718–722
10. W D C Man, M G G Soliman, D Nikoletou, M L Harris, G F Rafferty, N Mustfa, M I Polkey,J Moxham. Non Volitional assessment of skeletal muscle strength in patients with COPD. Thorax 2003; 58:665-666
11. Gea JG, Pasto M, Carmona MA, Orozco-Levi M Palomeque J, Broquetas J.Metabolic characteristics of the deltoid muscle in patients with chronic obstructive pulmonary disease. Eur Respir J 2001; 17: 939–945
12. Sarah Bernard, Pierre le Blanc, Francois Whittom, Guy Carrier,Jean Jobin, Roger Belleau, Francois Maltais, Peripheral muscle weakness in patients with COPD, Am J Respir Crit Care Med 1998;158: 629 -634
13. Sporrong H Palmerud G, Herberts P. Hand grip increases shoulder muscle activity, An EMG analysis with static hand contractions in 9 subjects. Acta Orthop Scand 1996 Oct; 67(5):485-90
14. O.Alizadehkhaiyat, A.C. Fisher, G.J. Kemp, Karthik Vishwanathan, S.P. Frostick,Shoulder muscle activation and fatigue during a controlled forceful hand grip task Journal of Electromyography and Kinesiology;21(3):478-482, June 2011
15. Alvar G. N. Agustí, Jaume Sauleda, Cristina Miralles, Cristina Gomez Bernat Togores, Ernest Sala, Santiago Batle,and Xavier Busquets. Skeletal Muscle Apoptosis and Weight Loss in Chronic Obstructive Pulmonary DiseaseAm J Respir Crit Care Med Vol 166. pp 485–489, 2002
16. Schols AMWJ, Soeters PB, Dingemans AMC, Mostert R,Frantzen PJ, Wouters EFMPrevalence and characteristic of nutritional depletion in patients with stable COPD eligible for pulmonary rehabilitation. Am Rev Respir Dis1993; 147: 1151–1156.
17. P.J. Barnes and B.R. Celli Systemic manifestations and co morbidities of COPDEur Respir J 2009; 33:1165–1168.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





