IJCRR - 4(19), October, 2012
Pages: 137-145
Print Article
Download XML Download PDF
A CADAVERIC STUDY ON THE VARIATIONS IN THE ORIGIN, COURSE AND BRANCHING PATTERN OF THE PROFUNDA FEMORIS ARTERY
Author: Mamatha H., Jessica S., Suhani S., Antony Sylvan D souza
Category: Healthcare
Abstract:Introduction: The profunda femoris artery which is the largest deep branch of femoral artery provides the principal supply to the extensor, adductor and flexor muscles of the thigh. This large artery arises from the posterolateral side of the femoral artery about 3.5-5cm from the mid-inguinal point and gives lateral and medial circumflex femoral branches and three perforating branches. The study of the femoral artery and its branching pattern has been a great interest among the anatomists and the surgeons because of its major implication in the clinical as well as radiological interventions. Material and Methods: This artery is easily accessible to catheterization and thereby to investigation of any arterial system in the body. In the present study, twenty (40 limbs) formaldehyde embalmed cadavers without malformations were dissected during the educational dissection in the Department of Anatomy, Kasturba Medical College. Results: We got the results like higher origin of the profunda femoris artery was seen in one specimen, the descending branch of the circumflex femoral artery arising from the femoral artery, descending branch of lateral circumflex femoral artery arising as a separate trunk from the profunda femoris. MCFA arising from the femoral artery about 3.2cm proximal to the origin of profunda femoris, the ascending circumflex femoral artery from the profunda femoris artery. Taking into consideration about the importance of the femoral artery and the profunda femoris artery primary attention has been given for the accurate anatomical knowledge about the aforementioned vessels. Hence, this present cadaveric study has been undertaken to study the prevalence of origin of the profunda femoris artery along with its circumflex branches.
Keywords: Femoral artery, Profunda femoris artery, Medial circumflex artery
Full Text:
INTRODUCTION
Femoral artery is the continuation of the external iliac artery and enters the femoral triangle behind the inguinal ligament midway between the Anterior Superior Iliac Spine and the symphysis pubis. A cluster of four small branches – superficial epigastric artery, superficial circumflex iliac artery, superficial external pudendal artery and the deep external pudendal artery originate from the femoral artery in the femoral artery and supply cutaneous regions of the upper thigh, lower abdomen and perineum.1The profunda femoris artery which is the largest deep branch of femoral artery provides the principal supply to the extensor, adductor and flexor muscles of the thigh. This large artery arises from the posterolateral side of the femoral artery about 3.5-5cm from the midinguinal point. The deep artery of the thigh has lateral and medial circumflex femoral branches and three perforating branches. The former artery arises from the lateral side of the profunda femoris artery and the latter arises from the posteromedial aspect of the profunda femoris artery. The head and neck of the femur are supplied by both the circumflex branches. The greater trochanter, vastus lateralis and the knee is supplies by the lateral circumflex femora artery whereas the medial circumflex femoral artery supplies to the fatty tissue in the acetabular fossa and to the adductor muscles.2, 3The study of the femoral artery and its branching pattern has been a great interest among the anatomists and the surgeons because of its major implication in the clinical as well as radiological interventions. This artery is easily accessible to catheterization and thereby to investigation of any arterial system in the body. The profunda femoris artery is used for arteriography, ultrasound and Doppler imaging, digital subtraction angiography and magnetic resonance imaging.4Taking into consideration about the importance of the femoral artery and the profunda femoris artery primary attention has been given for the accurate anatomical knowledge about the aforementioned vessels. Hence, this present cadaveric study has been undertaken to study the prevalence of origin of the profunda femoris artery along with its circumflex branches.
MATERIALS AND METHODS
In the present study, twenty (40 limbs) formalin fixed cadavers without malformations were dissected during the educational dissection in the Department of Anatomy, Kasturba Medical College. The femoral triangle was dissected meticulously, femoral sheath was identifies and its compartments were dissected to expose the femoral artery. The profunda femoris artery along with its medial and lateral branches was identified and its origin and course were studied. The origin of the profunda femoris artery from the midinguinal point was measured with a scale and a caliper in centimeters and noted for the study.
RESULTS
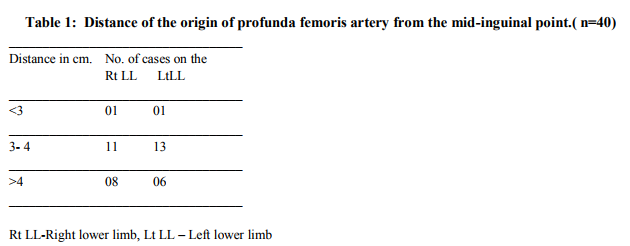
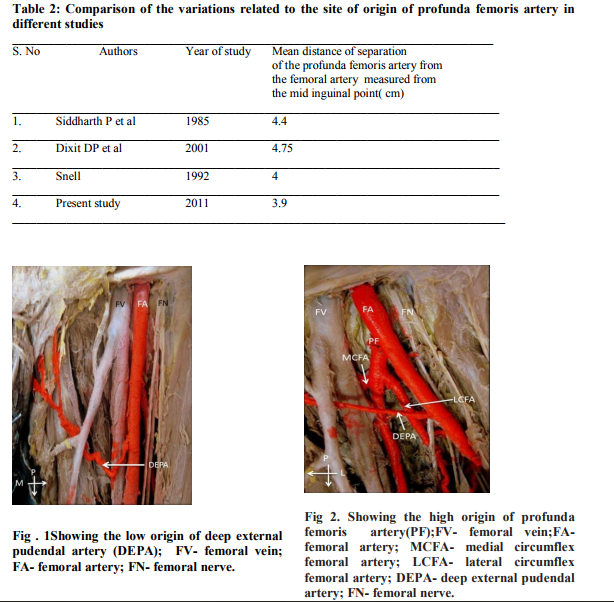
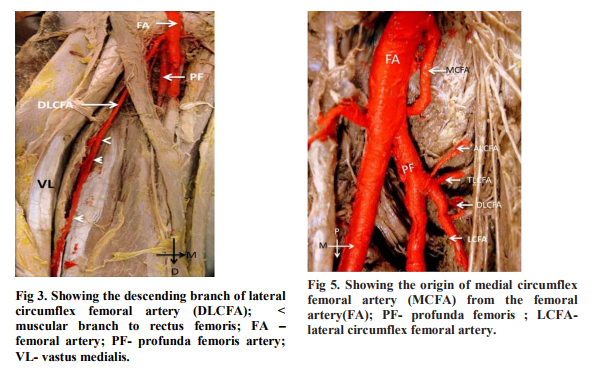
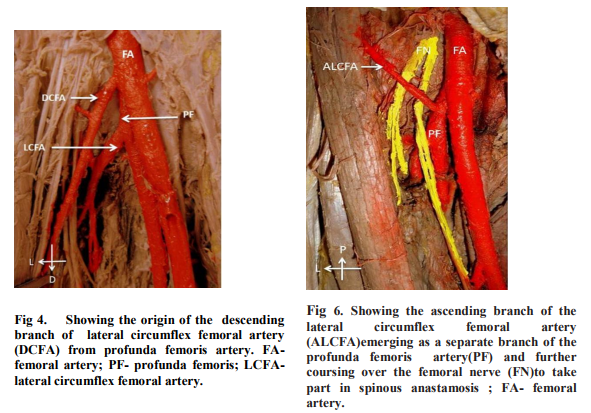
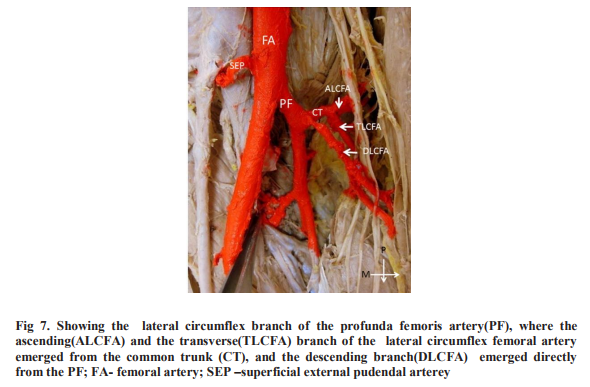
The higher origin of the profunda femoris artery was seen in 5% of the cases (Table.1), while deep external pudendal artery was arising at distance of 5cm from the mid-inguinal point (Fig.1and fig .2). In 2.5 % of the cases the descending branch of the circumflex femoral artery was found to origin from the femoral artery which after giving muscular branches to vastus lateralis (Fig.3) continued below to take part in genicular anastomosis. In2.5 % of the cases the descending branch of lateral circumflex femoral artery arising as a separate trunk from the profunda femoris artery. The artery gave muscular branches to the rectus femoris and ran along the nerve to vastus lateralis (Fig. 4) and descended down to give its contribution for the genicular anastomosis around knee joint. In 2.5% of the cases the medial circumflex femoral artery was arising from the femoral artery about 3.2cm proximal to the origin of profunda femoris artery( Fig. 5). After its origin the artery took its normal course of passing between the pectineus and psoas major muscle and eventually divided into its three terminal branches. The PFA also originated at about 4.5 cm from the mid-inguinal point( Fig. 6) and the ascending circumflex femoral artery was found to arise from the profunda femoris artery which coursed in front of the femoral nerve to take part in the spinous anastomosis. In 2.5 % of the cases ascending and transverse branches of the lateral circumflex femoral artery was found to emerge from the common trunk originating from the profunda femoris artery. However descending branch of the lateral circumflex femoral artery was found to descend as a separate branch form the profunda femoris artery (Fig. 7).
DISCUSSION
Normally anatomy explains the femoral artery to be a continuation of the external iliac artery giving off superficial and deep branches among which the profunda femoris is the largest from which two circumflex and four perforating braches emerges. According to Bergman et al the femoral artery may give rise to the inferior epigastric artery, deep circumflex iliac, lateral femoral circumflex, medial femoral circumflex, iliolumbar, accessory femoral circumflex (medial and lateral), descending branch of the lateral femoral circumflex and fourth or lowest perforating artery (general femoral nutrient or arteria femoris magna)”5 .Anatomical variations reported at the level of the division of the femoral artery can be explained as follows. In the lower animals, the profunda femoris artery is a branch of the internal iliac artery. During course of evolution, the origin shifted distally from the femoral artery. Ontogeny recapitulates phylogeny. Hence, developmental arrest at different stages may lead to anatomical variations related to the division of the femoral artery.6 In the present study, there are numerous variations observed which will be hereby considered in the discussion. (Table. 2) In 430, Quain found that the distance from the inguinal ligament of the origin of the profunda was between 2.5 and 5.1 in 68%; of these it was between 2.5 and 3.8 in 42.6%. This distance was less than 2.5 cm in 24.6% and more than 5.1 cm in only 7.4%.5 In our study, there was a prevalence of higher origin of profunda femoris artery which was measured about 1.3 cm from the mid- inguinal point. Literatures say that when the origin of profunda femoris is high, it will emerge from the lateral side of the femoral artery. But in our study there was no such case for the lateral origin, however the artery had its own normal posterolateral origin .Additionally, there was a lower origin of the Profunda Femoris Artery in which Medial Circumflex Femoral artery was arising at distance of 3cm proximal to the origin of Profund Femoris. In the higher origin of the same artery, the deep external pudendal artery was arising at a distance of 5.2cm from the midinguinal point. MCFA, which shows different branching patterns is an important artery in supplying blood to the head and neck of the femur, to the adductor muscles and to fatty tissue in the acetabular fossa.7,8 Because of its close relationship with this area there is a high risk of severing the artery after trauma or during operations such as total hip arthroplasty.9,10,11,12 It also has great importance in plastic surgery operations as the vascular pedicle of grafts such as the transverse upper gracilis (TUG) flap, the superomedial thigh flap and the medial circumflex femoral (gracilis) perforator free flap.13,14,15 It is used in selective arteriography in idiopathic ischaemic necrosis of the femoral head to determine the arterial supply of the femoral head. 16 Comprehensive knowledge of the extracapsular anatomy of the MCFA would safeguard against avascular necrosis of the femoral head when the posterior approach is required n procedures such as reconstructive surgery of hip and acetabular fracture fixation. 17 Normally, the medial circumflex femoral artery is a branch of profunda femoris artery. In our study, the normal pattern of origin of medial circumflex femoral artery was seen in 87.5%. We compared this data to the various studies done till now Tanyeli et al.3 (2006) found in 79% cases, Dixit DP et al.4 (2001) in 62.5%, Siddharth et al.18(1985) in 63% , Massoud and Fletcher19 in 81%, LIpshutz 20(1916) in 59% and Clark and Colborn21 (1993) in 53%.Our results are therefore closest to those of Massoud and Fletcher. The medial circumflex femoral artery can also arise from the femoral artery. In the previous literatures, the origin of medial circumflex from femoral artery was found to be 26% in Siddharth27 ,6.4% in Massoud and Fletcher24, 21% in Tanyeli E et al.3 , 36% in LIpshutz25 and 40% in Clark and Colborn26 .Therefore our result was in consistent to Tanyeli E et al. Bergman et al have found the ascending and descending branches of the lateral circumflex artery to be arising from the femoral artery and the profunda femoris artery respectively in 2 cases (1.8%).5 Similary, our study also showed the prevalence of ascending branch of lateral circumflex femoral artery from the profunda femoris unilaterally in one out of 40 limbs i.e. in 2.5%. This ascending branch can be used as a supply for vascularized iliac transplantation.22 The descending branch of the lateral circumflex femoral artery also originated from the femoral artery in 2.5%. This also was not of much clinical importance but literatures have found that descending branch can act as collateral in obstructed superficial femoral artery and can be used in Coronary Artery bypass surgery. 24The descending branch of the lateral circumflex femoral artery has been used as a high flow conduit for extra cranial intracranial bypass surgery successfully.25 Another anomaly to report was the descending branch of the lateral circumflex femoral artery arising as a separate trunk from the profunda femoris artery which was not reviewed in the literatures to the date of present study. In our study, the lateral circumflex femoral arteries were all arising from the profunda femoris artery. Yasuhiko Sugawara et al have reported the successful utilization of the lateral circumflex femoral artery as a midway out flow for aortolateral circumflex femoropopliteal artery sequential bypass on a patient with total occlusion of all major arteries in the unilateral iliofemoral region.26 Lateral circumflex femoral artery is used as a perforator flap in the reconstruction of gunshot wounds. It can be used as an anterolateral thigh flap. Its branches are used for aortopopliteal bypass, coronary artery bypass surgery. Anatomical variations reported are due to the developmental arrest at different stages of the arterial network of the lower limb in the embryo27 . Very early in the developmental process the, anastomosis cab be found between the dorsal sciatic artery and ventral femoral artery. Later capillary plexus in front of the pelvis and thigh form complex vascular networks, named rete pelvicum and rete femorale. It is generally accepted that an increase of blood-flow determines the final mature arterial pattern. Thus the most appropriate channels enlarge while others contract and disappear, thereby establishing the final arterial ramification.28.
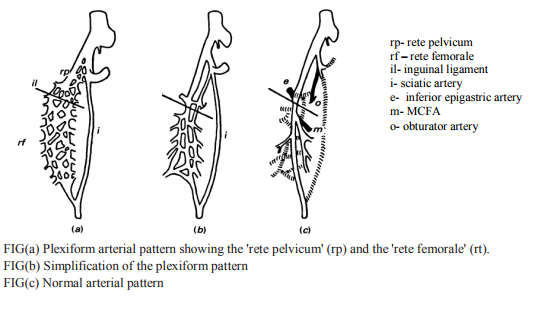
Ontogenetic interpretations of the anomalies in our study are as follows: 1) Before the MCFA appear as an independent blood vessels from the ‘rete femorale’ the blood flow designed for their territory make an unusual choice of some channels and instead arising from the profunda femoris, it arises from the femoral artery. 2) We can also speculate that one possible reason for the higher origin of the profunda femoris artery could be due to increased blood flow in the rete femoral vessels.
CONCLUSION
The existence of embryological variations of the arteries of the lower limb often results from unexpected developmental defects of the embryological arterial network. Knowledge of prevalence of the aforementioned anatomical variations is important to prevent iatrogenic injury to these vessels while undertaking clinical procedures within the femoral region. Before the catheterization of femoral vessels and operations in the femoral triangle, high-resolution ultrasonic imaging can provide anatomical and functional information about the femoral vessels and would be of assistance in planning catheterization29
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Susan Standring, Gray’s Anatomy; The Anatomical Basis of Clinical practice, 40th edition, Elsivier Churchill Livingstone; 2005
2. Uzel M,Tanyeli E, Yildirim M. Anatomical study of the origin of the lateral circumflex femoral artery in the Turkish population, Folia Morphol, 2008,67(4):226-30.
3. Tanyeli E, Uzel M, Yildirim M, Celik HH. An anatomical study of the origins of the medial circumflex femoral artery in the Turkish population, Folia Morphol( warsz), 2006,65(3):209 -12.
4 . Dixit DP, Mehta LA, Kothari ML. Variation in the origin and course of profunda femoris, J Anat. Soc. India, 2001 50(1)6-7.
5. Compendium of human anatomic variation. Ronald A bergman, pg.86.
6. Prakash, Jyoti Kumari, Kumar Bharadwaj A, Betty Anna Jose, Kumar Yadav S, Sing G. Variations in the origins of the profunda femoris, medial and lateral femoral circumflex arteries: a cadaver study in the Indian population, RJME , 2010,51(1):161-170.
7. Moore KL (1999) Clinically oriented anatomy. 3rd ed.Williams and Wilkins, Baltimore, pp. 188, 545.
8. Williams PL, Warwick R, Dyson M, Bannister LH Gray’s anatomy, 37th ed. Churchill and Livingston, London, 1989,pp. 781–783.
9. Aust JC, Bredenberg CE, Murray DG, Mechanisms of arterial injuries associated with total hip replacement.Arch Surg, 1981, 116: 345–349.
10. Langer R, Langer M, Scholz A, Astinet F, Schwetlick G,Felix R ,Femoral head perfusion in patients with femoral neck fracture and femoral head necrosis, J Belge Rad,1993, 76: 145–149.
11. Nachbur B, Meyer RP, Verkkala K, Zurcher R,The mechanisms of severe arterial injury in surgery of the hip joint. Clin Orthop Relat Res, 1979,141: 122–133.
12. Pai VS, Compartment syndrome of the buttock following a total hip arthroplasty. J Artroplast, 1996, 11: 609–610.
13. Arnez ZM, Pogorelec D, Planinsek F, Ahean U, Breast reconstruction by the free transverse gracilis (TUG) flap. Br J Plast Surg, 2004, 57: 20–26.
14. Hallock GG , The medial circumflex femoral (gracilis) local perforator flap — a local medial groin perforator flap. Ann Plast Surg, 2003,51: 460–464.
15. Har-Shai Y, Hirshowitz B, Marcovich A, Eliachar I, Peretz BA, Blood supply and innervation of the superomedial thigh flap employed in one-stage reconstruction of the scrotum and vulva — an anatomical study, Ann Plas Surg, 1984,13: 504–510.
16. Oide T , Selective medial circumflex femoral arteriography in idiopathic ischemic necrosis of the femoral head in adults. Nippon Seikeigeka Gakkai Zasshi, 1979,53: 293–305.
17. Gautier E, Ganz K, Krugel N, Gill T, Ganz R , Anatomy of the medial femoral circumflex artery and its surgical implications, 2000,J Bone Joint Surg Br, 82: 679–683.
18. Siddharth P, Smith NL, Mason RA, Giron F, Variational anatomy of the deep femoral artery, Anat Rec, 1985, 212(2):206–209
19. Massoud TF, Fletcher EWL , Anatomical variants of the profunda femoris artery: an angiographic study,Surg Radiol Anat,1997, 19: 99–103.
20. Lipchutz BB, Studies on the blood vascular tree, A composite study of the femoral artery, Anatomical Record, 1961,10: 361-70.
21. Clark SM, and Colborn GL,The medial femoral artery: its clinical anatomy and nomenclature, Clinical Anatomy, 1993, 6: 94- 105.
22. Siddharth P, Smith NL, Mason RA, Giron F,Variational anatomy of the deep femoral artery, Anat Rec, 1985, 212: 206–209.
23. Xu DC, Kong JM, Zhong SZ, The ascending branch of the lateral circumflex femoral artery. A new supply for vascularized iliac transplantation, Surg Radiol Anat, 1989,11: 263–264.
24. Fukuda H, Ashida M, Ishii R, Abe S, Ibukuro, Anatomical variants of the lateral femoral circumflex artery: an angiographic study. Surg Radiol Anat, 2005, 27:260–264.
25. Baskaya M K, Kiehn M W, Ahmed A S, Ates O, Niemann D B; Alternative vascular graft forextracranial-intracranial bypass surgery: descending branch of the lateral circumflex femoral artery, Neurosurgical Focus,2008, 24(2):E8.
26. Yasuhiko Sugawara et al Utilization of Lateral circumflex artery as Midway Outflow for Aortopopliteal grafting: Report of a case Surgery Today, 1998,28 (9) :967-970.
27. Sanudo JR, Roig M, Rodriguez A, Ferreira B, Domenech JM.Rare origin of the obturator, inferior epigastric and medial circumflex femoral arteries from a common trunk, JAnat , 1993, 183(1):161-163.
28. Bunyamin Sahin, Ahmet Uzun, Mehmet Emirzeoglu, Rengin Kosif, Sait Bilgic. A deep femoral artery passing in front of the femoral vein, Folia Morphol, 2003,62(2):143- 146.
29. Sahn DJ, Goldenberg SJ, Allen HD, ValdesCruz LM, Canale JM, Lange L, Friedman MJ (1982) A new technique for noninvasive evaluation of femoral arterial and venous anatomy before and after percutaneous cardiac catheterization in children and infants. Am J Cardiol, 49: 349–355.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





