IJCRR - 4(19), October, 2012
Pages: 78-82
Date of Publication: 15-Oct-2012
Print Article
Download XML Download PDF
A VARIANT DELTOID MUSCLE -A CASE REPORT
Author: Sharadkumar Pralhad Sawant, Shaguphta T. Shaikh, Rakhi Milind More
Category: Healthcare
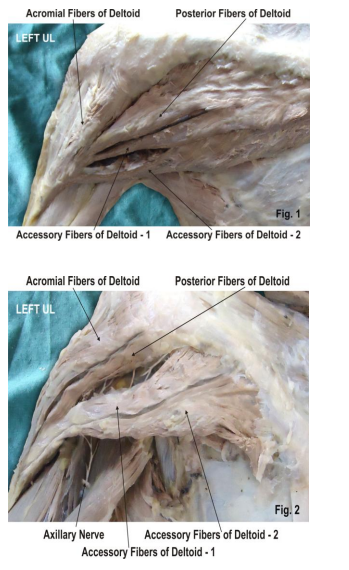
Abstract:During routine dissection for Ist MBBS students on 65 years donated embalmed male cadaver in the Department of Anatomy, K.J.Somaiya Medical College, we observed the multiple heads of the deltoid muscle in the left arm. The posterior fibers of the left deltoid muscle were enclosed in a distinct fascial sheet and the deltoid muscle was seen to arise from the middle 1/3 of the vertebral border of the scapula. However there was no variations in the blood supply and the nerve supply of the deltoid muscle. The photographs were taken for proper documentation. The existence of the multiple heads of the deltoid muscle should be kept in mind by surgeons operating on deltoid, posterior deltoid, or doing scapular flaps.
Keywords: Deltoid Muscle, Multiple Heads, Variations, Vertebral Border of Scapula, Scapular Flaps, Surgeons.
Full Text:
INTRODUCTION
In human anatomy, the deltoid muscle is the muscle forming the rounded contour of the shoulder. Anatomically, it appears to be made up of three distinct sets of fibers though electromyography suggests that it consists of at least seven groups that can be independently coordinated by the central nervous system (1). It was previously called the Deltoideus and the name is still used by some anatomists. It is called so because it is in the shape of the Greek letter Delta (triangle). It is also known as the common shoulder muscle, particularly in lower animals (e.g., in domestic cats). Deltoid is also further shortened in slang as "delt". The plural forms of all three incarnations are deltoidei, deltoids and delts. A study of 30 shoulders revealed an average weight of 191.9 grams (6.77 oz) (range 84 grams (3.0 oz)–366 grams (12.9 oz)) in humans (2). The deltoid originates in three distinct sets of fibers, often referred to as "heads" (3). The anterior or clavicular fibers arises from most of the anterior border and upper surface of the lateral third of the clavicle (4) The anterior origin lies adjacent to the lateral fibers of the pectoralis major muscle as do the end tendons of both muscles. These muscle fibers are closely related and only a small chiasmatic space, through which the cephalic vein passes, prevents the two muscles from forming a continuous muscle mass (5).The anterior deltoid are commonly called front delts for short. Lateral or acromial fibers arise from the superior surface of the acromion process (4). They are commonly called lateral deltoid. This muscle is also called middle delts, delts, side delts or outer delts for short. They are also mistakenly called medial deltoid, which is wrong, as their origin is the least medial portion of the deltoid. Posterior or spinal fibers arise from the lower lip of the posterior border of the spine of the scapula (4). They are commonly called posterior deltoid or rear deltoid (rear delts for short). Fick divided these three groups of fibers (6), often referred to as parts (Latin: pars) or bands, into seven functional components (7) ; the anterior part has two components (I and II); the lateral one (III); and the posterior four (IV, V, VI, and VII) components. In standard anatomical position (with the upper limb hanging alongside the body), the central components (II, III, and IV) lie lateral to the axis of abduction and therefore contribute to abduction from the start of the movement while the other components (I, V, VI, and VII) then act as adductors. During abduction most of these latter components (except VI and VII which always act as adductors) are displaced laterally and progressively start to abduct (7). From this extensive origin the fibers converge toward their insertion on the deltoid tuberosity on the middle of the lateral aspect of the shaft of the humerus; the middle fibers passing vertically, the anterior obliquely backward and laterally, and the posterior obliquely forward and laterally. Though traditionally described as a single insertion, the deltoid insertion is divided into two or three discernible areas corresponding to the muscle's three areas of origin. The insertion is an arch-like structure with strong anterior and posterior fascial connections flanking an intervening tissue bridge. It additionally give off extensions to the deep brachial fascia. Furthermore, the deltoid fascia contributes to the brachial fascia and is connected to the medial and lateral intermuscular septa (8). The deltoid is innervated by the axillary nerve. The axillary nerve originates from the ventral rami of the C5 and C6 cervical nerves, via the superior trunk, posterior division of the superior trunk, and the posterior cord of the brachial plexus. The axillary nerve is sometimes damaged during operations on the axilla, such as for breast cancer. It may also be injured by anterior dislocation of the head of the humerus. The deltoid is supplied by the posterior circumflex humeral artery. When all its fibers contract simultaneously, the deltoid is the prime mover of arm abduction along the frontal plane. The arm must be medially rotated for the deltoid to have maximum effect. This makes the deltoid an antagonist muscle of the pectoralis major and latissimus dorsi during arm adduction. The anterior fibers are involved in shoulder abduction when the shoulder is externally rotated. The anterior deltoid is weak in strict transverse flexion but assists the pectoralis major during shoulder transverse flexion / shoulder flexion (elbow slightly inferior to shoulders). The anterior deltoid also works in tandem with the subscapularis, pecs and lats to internally (medially) rotate the humerus. he posterior fibers are strongly involved in transverse extension particularly as the latissimus dorsi is very weak in strict transverse extension. Other transverse extensors, the infraspinatus and teres minor, also work in tandem with the posterior deltoid as external (lateral) rotators, antagonists to strong internal rotators like the pecs and lats. The posterior deltoid is also the primary shoulder hyperextensor, moreso than the long head of the triceps which also assists in this function. The lateral fibers perform basic shoulder abduction when the shoulder is internally rotated, and perform shoulder transverse abduction when the shoulder is externally rotated. They are not utilized significantly during strict transverse extension (shoulder internally rotated) such as in rowing movements, which use the posterior fibers. An important function of the deltoid in humans is preventing the dislocation of the humeral head when a person carries heavy loads. The function of abduction also means that it would help keep carried objects a safer distance away from the thighs to avoid hitting them, such as during afarmer's walk. It also ensures a precise and rapid movement of the glenohumeral joint needed for hand and arm manipulation (2). The lateral fibers are in the most efficient position to perform this role, though like basic abduction movements (such as lateral raise) it is assisted by simultaneous contraction of anterior/posterior fibers. In both the carrying of heavy loads and in lateral raises, the deltoid often contracts in tandem with scapular elevators such as the levator scapulae, upper trapezius or serratus anterior. By pulling the clavicle and scapulae up, it reduces compression and possibly impingement on the inferior borders so it doesn't press as much against the uppermost ribs. The deltoid is responsible for elevating the arm in the scapular plane and its contraction in doing this also elevates the humeral head. To stop this compressing against the under surface of the acromion the humeral head and injuring the supraspinatus tendon, there is a simultaneous contraction of some of the muscles of the rotator cuff: the infraspinatus and subscapularis primarily perform this role. In spite of this there may be still a 1–3 mm upward movement of the head of the humerus during the first 30° to 60° of arm elevation (2). Large variations uncommon. More or less splitting common. Continuation into the Trapezius; fusion with the Pectoralis major; additional slips from the vertebral border of the scapula, infraspinous fascia and axillary border of scapula not uncommon. Insertion varies in extent or rarely is prolonged to origin of Brachioradialis (11). The deltoid muscle derives from the dorsal muscle mass of the limb bud which is formed by somatic mesoderm during the fifth intrauterine week (9). Variations and anomalies of the deltoid muscle are uncommon. We report a very rare variation of the multiple heads of the deltoid muscle because of its clinical and anatomical relevance. Bilateral separation of the posterior fibers with a fascia has been described in 1993 (10). Such type of unilateral separations of the multiple heads of the posterior fibers of the deltoid muscle has not been found in literature. Case Report During routine dissection for Ist MBBS students on 65 years donated embalmed male cadaver in the Department of Anatomy, K.J.Somaiya Medical College, we observed the multiple heads of the deltoid muscle in the left arm. The posterior fibers of the left deltoid muscle were enclosed in a distinct fascial sheet and the deltoid muscle was seen to arise from the middle 1/3 of the vertebral border of the scapula (Fig.1) However there was no variations in the blood supply and the nerve supply of the deltoid muscle (Fig.2). The photographs were taken for proper documentation. No other associated neuro-vascular variations were observed in the same upper limb. The right upper limb of the same cadaver was also normal.
DISCUSSION
The deltoid muscle arises from the anterior border and upper surface of the lateral third of the clavicle, the lateral margin and upper surface of the acromion, and the lower edge of the posterior border of the spine of the scapula. The insertion is into the deltoid tubercle on the middle of the lateral side of the body of the humerus (11). It is innervated by the fifth and sixth cervical spinal nerves through the axillary nerve. Its vascular supply is through the acromial and deltoid branches of the thoracoacromial artery, the anterior and posterior circumflex humeral arteries, and the deltoid branch of the profunda brachii (11). The continuation of the fibers of the deltoid muscle into the trapezius; fusion with the pectoralis major; and the presence of additional slips from the vertebral border of the scapula, infraspinous fascia, and the axillary border of scapula are the commonly reported variations of the deltoid muscle (11). The myogenic cells coalesce into two muscle masses during the fifth intrauterine week (9). One is the precursor of the flexor muscles the other is the precursor of the extensor muscles. These common muscle masses then split into anatomically recognizable precursors of the definitive muscles of the limb. There is little data about the mechanism of this splitting (12). The deltoid muscle derives from the dorsal muscle mass (9). The multiple heads of the deltoid may be developed because of incorrect splitting of the dorsal muscle mass. Comparative anatomy The deltoid is found in apes other than humans. The human deltoid is of similar proportionate size as the muscles of the rotator cuff in apes like the orangutan. These apes engage inbrachiation and possess the muscle mass needed to support the body weight by the shoulders. In other apes, like the common chimpanzee, the deltoid is much larger than in humans, weighing an average of 383.3g compared to 191.9g in humans. This reflects the need to strengthen the shoulders, particularly the rotatory cuff, in knuckle walking apes for the purpose of supporting the entire body weight (2). Clinical anatomy Clinically fasciocutaneus, musculocutaneus or muscular deltoid and posterior deltoid flaps are especially used in; tetraplegia (by a transfer to triceps), radionecrotic defects situated over the glenohumeral joint, reconstruction of extremity, rotator cuff tears, and oral cavity. While elevating musculocutaneus or muscular deltoid and posterior deltoid flaps, the surgeon must be alert to the possibility of this variation's presence because it may cause confusion when dissecting the borders. Similarly, while elevating fasciocutaneus deltoid and posterior deltoid flaps or a scapular flap (either transverse or parascapular), an accessory deltoid may be confused with the teres major muscle because of its location and its distinct fascia and as a result of this the dissection of the pedicle can be much more difficult.
CONCLUSION
The existence of such variation of the deltoid muscle should be kept in mind by surgeons operating on deltoid, posterior deltoid, shoulder joint or doing scapular flaps. Competing Interests: The authors declare that they have no competing interest. Authors' contributions: SPS wrote the case report, performed the literature review & obtained the photograph for the study. RMM performed the literature search and assisted with writing the paper. STS conceived the study and helped to draft the manuscript. All authors have read and approved the final version manuscript.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. All the authors are thankful to Dr. Arif A. Faruqui for his support. Authors are also thankful to Mr. M. Murugan typing the article .
References:
1. Brown JM, Wickham JB, McAndrew DJ, Huang XF. (2007). Muscles within muscles: Coordination of 19 muscle segments within three shoulder muscles during isometric motor tasks. J Electromyogr Kinesiol. 17(1):57-73.
2. Potau JM, Bardina X, Ciurana N, Camprubí D. Pastor JF, de Paz F. Barbosa M. (2009). Quantitative Analysis of the Deltoid and Rotator Cuff Muscles in Humans and Great Apes. Int J Primatol 30:697–708.
3. The Anatomy of the Shoulder Muscles: "The Deltoid is a three-headed muscle that caps the shoulder. The three heads of the Deltoid are the Anterior, Lateral, and Posterior."
4. "Deltoid Muscle". Wheeless' Textbook of Orthopaedics. December 2011. Retrieved January 2012.
5. Leijnse, J N A L; Han, S-H; Kwon, Y H (December 2008). "Morphology of deltoid origin and end tendons – a generic model". J Anat 213 (6): 733–742.
6. Fick, R. (1911). Handbuch der Anatomie und Mekanik der Gelenke. Jena: Gustav Fischer.
7. Kapandji, Ibrahim Adalbert (1982). The Physiology of the Joints: Volume One Upper Limb (5th ed.). New York: Churchill Livingstone.
8. Rispoli, Damian M.; Athwal, George S.; Sperling, John W.; Cofield, Robert H. (2009). "The anatomy of the deltoid insertion". J Shoulder Elbow Surg 18: 386– 390.
9. Larsen WJ. Human embryology. 3rd ed. Churchill Livingstone; 2001. p. 324.
10. Kayikcioglu A, Celik HH, Yilmaz E. An anatomic variation of the deltoid muscle (case report) Bull Assoc Anat (Nancy) 1993; 77:15–6.
11. Standring S, editor. The anatomical basis of clinical practice. International 39th ed. Churchill Livingstone; 2005. Gray's Anatomy; p. 836.
12. Carlson BM. Human embryology and developmental biology. 3rd ed. C.V. Mosby; 2004. p. 224.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





