IJCRR - 9(13), July, 2017
Pages: 50-53
Date of Publication: 03-Jul-2017
Print Article
Download XML Download PDF
Achondroplasia with Oral Lichen Planus - A Case Report
Author: Nivedita CKVS, Ajit D. Dinkar, Sonam Khurana
Category: Healthcare
Abstract:This article aims to highlight the occurrence of oral lichen planus in a patient with achondroplasia. The patient was treated with topical and systemic corticosteroids and showed significant improvement. Achondroplasia is the most common form of nonlethal skeletal dysplasia that manifests with stunted stature and disproportionate limb shortening. Clinical manifestations are mainly a result of mutations in fibroblast growth factor receptor-3 (FGFR3) gene. It is of special interest in the dental field because of its craniofacial features and dentists treating patients with achondroplasia should be well aware of the clinical features, risk factors and complications associated with this condition.
Keywords: Achondroplasia, Short stature, FGFR3 gene
DOI: 10.7324/IJCRR.2017.9139
Full Text:
Introduction:
Achondroplasia (OMIM 100800) was first described in 1878 and is the most common nonlethal skeletal dysplasia. It is inherited in an autosomal dominant fashion, the distinct clinical features of achondroplasia are evident at birth and primarily affect the skeleton, resulting in short-limbed dwarfism.1 The condition has been recognised for centuries, with examples seen in art from ancient Egypt, Greece, and Rome. However, it is estimated to occur in between one in 10,000 and one in 30,000 live births. The achondroplasia locus was mapped to chromosome 4p16.3 in 1994, and heterozygous mutations of FGFR3 were identified shortly afterwards.2
Increased incidence of sporadic mutations have also been associated with increasing paternalage.3 The present article depicts a rare case of achondroplasia with oral lichen planus in a 42 year old male patient.
Case Report:
A 42 year old male reported to Department of Oral Medicine and Radiology with the chief complaint of burning sensation in the oral mucosa on having hot and spicy food. Burning sensation started almost 2 months back which was insidious in nature and aggravated on having spicy food. He also gave a history of chronic irritation to the buccal mucosa due to entrapment of cheek between the teeth. The patient was born to non consanguineous parents, and was born full term. Postnatal history couldn’t be obtained since his parents have expired. Patient has an elder brother who is normal and two elder sisters who have short stature. Medical history revealed that he has epilepsy and is under sodium valproate. He attended school only till 5th standard. Cognitive and intelligence test (Binet Kamat Test and Bhattia’s battery of performance) performed by a clinical psychologist revealed that he had poor understanding capacity, poor eye contact, restlessness and delayed reactions for performance. IQ was 69-75 and was categorized as mild but normal. His observation capacity was good.
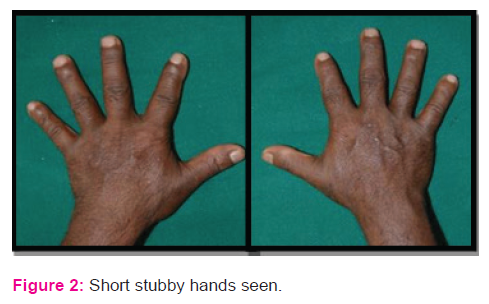
General physical examination showed short stature, lordotic lumbar spine, rhizomelic shortening of the arms and legs, short stubby trident hands. Prominent buttocks and protuberant abdomen
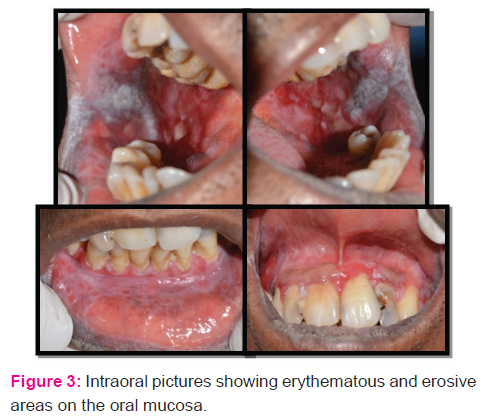
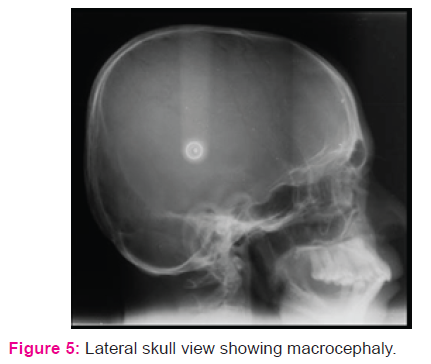
were also evident.Anthropometry revealed a height of 124.9 cms and weight of 35kgs, with upper limb to lower limb ratio of >1. The head circumference was 49.7 cms. His vital signs were within the normal limits. Systemic examination did not reveal any other abnormality. Extraoral examination revealed enlarged calvarium, brachycephaly, midfacial hypoplasia, widening of nasal bridge and competent lips. The chin was retruded and not prominent.On intraoral examination, there were diffuse erythematous and ulcerative areas on the right and left buccal mucosa with white prominent keratotic areas and pigmentation at retrocommisural region. White striae arranged in annular pattern were seen on the lower labial mucosa along with generalized erythema of the marginal and papillary gingiva and the lesion was non-tender on palpation. Other dental findings were increased anterior proclination of upper and lower anterior teeth, class 2 canine relationship and generalized recession of gingiva. Size, number and form of teeth were normal with few carious lesions.
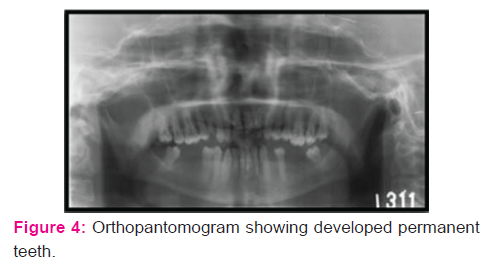
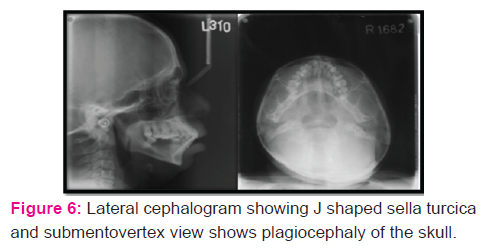
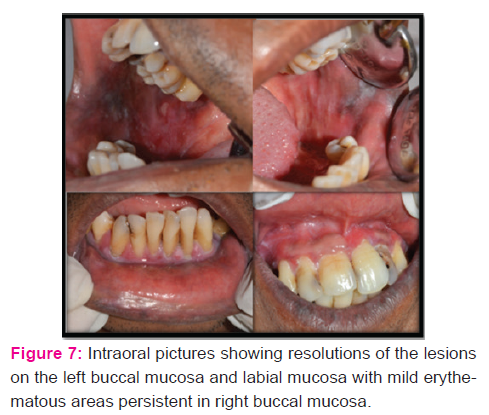
On radiographic examination, his orthopantomogram showed the presence of permanent teeth with missing 3-4, 3-6, 3-7, 4-6 and 4-7. Enlarged calvarium with an increase in the transverse diameter, J shaped sella, shortening of the skull base, retruded maxilla, Proclinedmaxillary and mandibular incisors were evident in the lateral cephalogram. Submentovertex view showed plagiocephaly. A final diagnosis of achondroplasia was made based on the history, clinical examination and radiological investigations. The patient was advised for biopsy and was subjected to routine blood investigations. Microscopic findings revealed fibro collagenous tissue covered by stratified squamous epithelium showing hyperkeratosis, acanthosis and formation of subepithelial bulla. The subepithelial tissue shows dense chronic inflammatory infiltrate. All these features were suggestive of oral lichen planus. During his treatment period, he was given topical steroids along with systemic steroids. Topical Clobetesol 0.01% along with systemic prednisolone 30mg in divided doses was prescribed to the patient. Initially, he was being reviewed at an interval of every 1-2 weeks for 2 months. When active lesions had stopped forming, the doses of the medications were being tapered and he was being reviewed after every 6 months period. Symptomatic improvement along with resolution of the lesions were noted. The patient was then referred for further dental treatment.
Discussion:
Achondroplasia is part of a spectrum of disorders caused by different mutations in FGFR3, which includes hypochondroplasia, severe achondroplasia with developmental delay and acanthosis nigricans (SADDAN), and thanatophoric dysplasia, of which two types can be distinguished by radiograph and molecular analysis (thanatophoric dysplasia I and thanatophoric dysplasia II).2 The common mutation causes a gain offunction of the fibroblast growth factor receptor-3 (FGFR3) gene, resulting in decreased endochondral ossification, inhibited proliferation of chondrocytes in growth plate cartilage, decreased cellular hypertrophy and decreasedcartilage matrix production; leading to a variety of manifestations and complications.4 More than 99% of people with achondroplasia carry a point mutation at nucleotide 1138 in one copy of the fibroblast growth factor receptor-3 (FGFR3) gene: most commonly, a G→A transition, although G→C transversion has also been reported. Both mutations result in the substitution of arginine for glycine at residue 380 (G380R) in the transmembrane region of the fibroblast growth factor receptor-3 (FGFR3) protein. Chondrocyte proliferation and differentiation are inhibited, decreasing bone growth rates. Although the word achondroplasia literally means ‘without cartilage formation’, in this disorder the problem is not in cartilage formation but in converting cartilage to bone, particularly in the long bones of the arms and legs, the spine, and the skull. FGFR3 mutations alter the cartilage growth plate architecture; endochondral boneformation is therefore affected.1
In heterozygous state, achondroplasia isnon-lethal with normal life span and normal intelligence. However, they are at risk like cervicomedullary compression, spinal stenosis, obesity, obstructive sleep problem. Inhomozygous state, achondroplasia is a lethalcondition in the early few months of life because of severe rib cage deformity that results in respiratory insufficiency.5
Affected babies are short at birth and grow slowly throughout childhood; the average final height for women is 123 cm and 130 cm for men.4 Clinical features include long, narrow trunk and short limbs, especially in a proximal(rhizomelic) segment. The head is large with frontal bossing, but the midface is hypoplastic, a result of the endochondral origin of the base of the skull. Hyperextensibility of joints, especially the knees and hands, is common, but full extension and rotation of the elbow is usually restricted. The hands are short and broad with fingers exhibiting a three-pronged (trident) appearance at birth due to an inability to fully oppose the third and fourth digits. Thoracolumbar gibbus might be present at birth and usually develops by 4 months. Mild to moderate hypotonia is common in infancy, often secondary to spinal cord compression at the cervical medullary junction, and contributes to motor milestone delay. Newborns usually lie with hips abducted after their mother lays them down.2
Essential radiological features include (1) Symmetric shortening of all long bones, with proximal portions being more affected and lower limb involvement being more than the upper limb (rhizomelia). There’s relative flaring and splaying of metaphyses with normal epiphyses. (2) In children, the two limbs of the V of metaphysic appear to embrace the epiphysis giving rise to a ball and socket relationship/chevron deformity (3) The hand bones appear thick and tubular with widely separated 2ndand 3rddigits of the hands and inability to approximate them in extension, leading to appearance of trident hand (4) The pelvic cavity is short and broad, also called as champagne-glass appearance. There's squaring of iliac wings with some rounding of corners on afrontal projection (elephant ear shaped iliac wings). (5) In spine,there is progressive decrease in the interpedicular distance cranio-caudally in the lumbar spine. Posterior scalloping of vertebral bodies is also common while anteriorly they may appear rounded giving rise to a bullet-shaped configuration. (6) The skull shows narrowed skull base with narrowing of foramen magnum. There is compensatory over-expansion of the skull vault and frontal regions to accommodate the expanding brain. There’s relative mid-face hypoplasia and depressed nasal bones.3 As the condylar cartilage is the product of periosteal chondrogenesis, mandibular growth is not affected.6
Several dental manifestations have also been previously reported in the literature which includes skeletal and dental class III malocclusion, a narrow maxilla, macroglossia, and an open bite between the posterior teeth.7
Chawla K(2012) reported periodontal manifestations in achondroplasia and stated that the possible reason for periodontal disease could be that defective fibroblast growth factor receptor-3 (FGFR3) might hamper the growth and function of fibroblasts, which are the predominant cells found in the periodontal ligament. A missense mutation in FGFR3 gene leads to impaired formation ofFGFR3 protein, which can hamper the growth and function of periodontal fibroblasts.8
The differential diagnosis of achondroplasia includes other chondrodystrophies including hypochondroplasia and chondroectodermal dysplasia. Although hypochondroplasiais associated with dwarfism, it can be differentiated from achondroplasia by milder clinical features. Brachycephalyis much less pronounced in hypochondroplasia and also the trident hand configuration is not seen in hypochondroplasia.4 Prenatal diagnosis of homozygous achondroplasia can be made by mutation detection at 10-12 week of gestation as against 16-20 week by ultrasonographic examination. Ultrasonographic examination can detect shortening of long bones only in late pregnancy (third trimester). Prenatal diagnosis can be provided early in pregnancy by DNA based methods on chorionic villi.9 Genetic counseling regarding prenatal testing options is important so that families can understand their reproductive options.1 There have been several trials of human growth hormone treatment in children with achondroplasia, mostly using pharmacological doses comparable with those used in Turner syndrome Surgical limb lengthening is another approach that has been used to increase stature.2
Special precautions in head control during dental intervention are essential in children, due to the possible presence of cranio-cervical instability, foramen magnum stenosis and limited neck extension, as it might result in respiratorycomplications.5 It is also important for dental professionals, including pediatric dentists, orthodontists and oral surgeons treating these patients, to recognize risk factors and potential complications before sedation or anaesthesia. When dental treatment is decided to be under GA, it is recommended to do radiologic evaluation of foramen magnum, preoxygenation before anesthesia, using appropriate endotracheal tube size, oral intubation and administration of oxygen after extubation.6
Conclusion:
In conclusion, dentists treating patients with achondroplasia should be well aware of the clinical features, risk factors and complications associated with this condition. Psychological management during dental treatment is also essential as presence of short stature can pose a number of psychosocial and social problems.
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
- Erin M. Carter, Jessica G. Davis, Cathleen L. Raggio. Advances in understanding etiology of achondroplasia and review of management. Curr Opin Pediatr 19:32–37, 2007
- William A Horton, Judith G Hall, Jacqueline T Hecht. Achondroplasia. Lancet 2007; 370: 162–72
- Ananya Panda, Shivanand Gamanagatti, Manisha Jana, Arun Kumar Gupta. Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias. World J Radiol2014; 6(10): 808-825.
- Lata Kale, Neha Khambete, Sonia Sodhi, Rahul Kumar. Achondroplasia with oligodontia: Report of a rare case. Journal of Oral and Maxillofacial Pathology, 2013:17(3): 452-54.
- Rohilla S, Kaushik A, Vinod V, Tanwar R, Kumar M. Orofacial manifestations of achondroplasia. EXCLI J 2012;11:538-54.
- Afnan Al-Saleem, Asma Al-Jobair. Achondroplasia: Craniofacial manifestationsand considerations in dental management. The Saudi Dental Journal 2010; 22:195–199.
- Celenk P, Arici S, Celenk C. Oral findings in a typical case of achondroplasia. J Int Med Res 2003;31:236-8.
- Chawla K, Lamba AK, Faraz F, Tandon S. Achondroplasia and periodontal disease. J Indian Soc Periodontol 2012;16:138-40.
- Sethi RS, Kumar L, Chaurasiya OS, Gorakh R. Achondroplasia: A case report. Curr Pediatr Res 2011;15:137-42.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





