IJCRR - 4(20), October, 2012
Pages: 170-176
Date of Publication: 20-Oct-2012
Print Article
Download XML Download PDF
VARIANT HEADS OF BICEPS BRACHII MUSCLE
Author: Sharadkumar Pralhad Sawant , Shaguphta T. Shaikh, Rakhi Milind More
Category: Healthcare
Abstract:Aim: To study the occurrence of the variant heads of biceps brachii muscle. Materials and Methods: The 50 specimens of the 25 donated embalmed cadavers (20 males and 5 females) were dissected and observed for variations in the origin and insertion of biceps brachii muscle bilaterally in the department of Anatomy at K.J.Somaiya Medical College, Sion, Mumbai, INDIA. The dissection of arm and forearm was done meticulously in all the 50 specimens. The photographs of the supernumerary head of biceps brachii muscle were taken for proper documentation and for ready reference. Results / Observations: Out of 50 specimens, the supernumerary head was found in six specimens. The humeral head was taking origin from the anteromedial surface of the shaft of the humerus in three specimens and from the anterolateral surface of the shaft of the humerus in three specimens. In all six specimens, the supernumerary head joined with the other two heads and form a common tendon which got inserted into the radial tuberosity of the radius and bicipital aponeurosis. In the present study the incidence of supernumerary head of biceps brachii was 12%. In all the six specimens, the supernumerary head was found unilaterally (5 males and 1female specimen). In three specimens (50%) the supernumerary head was supplied by median nerve, the musculocutaneous nerve was absent in that specimen while in all other specimens the muscles of front of arm were supplied as usual by musculocutaneous nerve. The blood supply of the supernumerary head was from the brachial artery and vein. There was no variations in the vascular pattern of arm and forearm in all the specimens. Conclusion: Topographical anatomy and variations in the heads of the biceps brachii muscle is clinically important for surgeons, orthopaedicians and radiologists.
Keywords: Biceps Brachii Muscle, Supernumerary Head, Musculocutaneous Nerve, Median Nerve, Surgeons, Orthopaedicians, Radiologists.
Full Text:
INTRODUCTION
The biceps brachii is the muscle of the anterior compartment of the arm having two heads of origin proximally, a long head originating from the supraglenoid tubercle and glenoid labrum and a short head from the coracoid process of the scapula. Distally these two heads unite to form a common tendon that inserts into the posterior rough part of the radial tuberosity and bicipital aponeurosis which merges with the deep fascia of the forearm (1). This mode of insertion makes it an efficient and important supinator of the forearm. It is the only flexor of the arm that crosses the shoulder as well as the elbow joint thereby acting on both joints. It is innervated by the musculocutaneous nerve and vascularized by brachial and anterior circumflex humeral arteries and brachial vein (1). Biceps brachii has been stated as one of the muscles that shows frequent anatomical variations (2, 3, 4, 5). Some of its reported anomalies have been manifested as supernumerary fascicles that originate from the coracoid process, tendon of pectoralis major, articular capsule and head of the humerus or from humerus itself (6). Among those variations, the presence of a supernumerary fascicle arising from the shaft of the humerus, which is known as the humeral head of biceps brachii, is known to be the most common anomaly (3, 7, 8). Multiple supernumerary heads of four to seven have also been reported to a lesser extent (1, 3, 4, 5). A large body of evidence suggests a wide range of racial variations in the occurrence of humeral head of biceps brachii muscle. It was shown to have an incidence of 7.1% in Indians, 8% in Chinese, 10% in European whites, 10 % in Sri Lankans, 12% in African Blacks, 15% in Turkish, 18% in Japanese, 21.5% in South African Blacks and 8.3% in South African Whites, and 37.5 % in Colombians (3, 8, 9, 10, 11,12, 13, 14, 15, 16). From a clinical standpoint of view, muscle anomalies are difficult to differentiate from soft tissue tumors (5). High median nerve compression around the elbow joint has been described as resulting from a number of clinical and anatomical entities. The existence of an anomalous muscle in and around the elbow region may cause high median nerve palsy and compression of the brachial artery (5). Further, knowledge of the incidence of humeral head of biceps brachii will facilitate preoperative diagnosis as well as the surgical procedures of the upper limb (5,9).
MATERIALS AND METHODS
This study was carried out on a total of 25 donated embalmed cadavers (20 males and 5 females) during routine gross anatomy dissections in the Department of Anatomy at K.J.Somaiya Medical College, Sion, Mumbai, INDIA. The cadavers were preserved in 10% formalin. The age group of the cadavers varied between 65-80 years. Te skin is reflected by making a longitudinal incision on the anterior aspect of the arm extending from the level of acromian process to a point 2.5 cm below the elbow joint and horizontal incisions on both proximal and distal ends of the longitudinal incision. The arms were then dissected carefully to expose the full length of the biceps brachii muscle from its proximal to distal attachment. The presence of supernumerary heads, their origins and insertions were recorded. The photographs of the supernumerary head of biceps brachii muscle were taken for proper documentation and for ready reference.
RESULTS / OBSERVATIONS
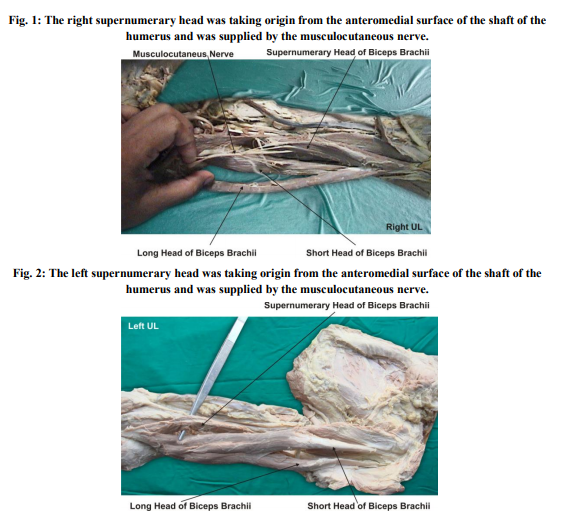
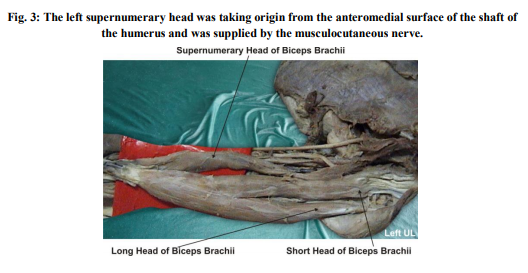
Out of 50 upper limbs of 25 cadavers, supernumerary heads of the biceps brachii were present in 6 specimens. The supernumerary head was taking origin from the anteromedial surface of the shaft of the humerus in three specimens and from the anterolateral surface of the shaft of the humerus in three specimens. In all the six specimens, the supernumerary head joined with the other two heads and form a common tendon which got inserted into the radial tuberosity of the radius and bicipital aponeurosis. In the present study the incidence of supernumerary head of biceps brachii was 12%. In all the six specimens, the supernumerary head was found unilaterally (3 male and 3 female specimens). In three specimens (50%) the supernumerary head was supplied by median nerve, the musculocutaneous nerve was absent in that specimen while in all other specimens the muscles of front of arm were supplied as usual by musculocutaneous nerve. The blood supply of the supernumerary head was from the brachial artery and vein. There were no variations in the vascular pattern of arm and forearm in all the specimens.
DISCUSSION
Anatomy is a morphological science which cannot fail to interest the clinicians. The present study documents the incidence and morphological characteristics of supernumerary heads of biceps brachii. The standard Anatomy text states the incidence of this variation as 10% (1). Although this is based on some European populations (10), it ignores a large body of evidence with reference to other populations (3, 8, 9, 11, 12, 13, 14, 15, 16). Furthermore, racial variation of the incidence of the supernumerary head of biceps brachii has been clearly demonstrated by comparative studies between Brazilian whites and black subjects. The incidence of supernumerary head of biceps brachii in blacks was found to be significantly lower than in whites (17). The variations of the incidence of the third head of biceps brachii were attributed to evolutionary or racial trends (8). In the present study the incidence of occurrence of supernumerary head of the biceps brachii was 12%. It was also interesting to note the gender differences of the occurrence of humeral heads of this muscle. The gender comparison of the incidence implies that the supernumerary head of the biceps brachii is a predominantly male condition (3, 10). The results of the present study disagree with the gender comparison documented in literature. In the present study the supernumerary head was found in 3 female specimens out of 10 female specimens (30%) and in 3 male specimens out of 40 male specimens (7.5%). Embryologically it has been stated that the third head of biceps brachii arises from the brachialis muscle and in such instances its distal insertion has been translocated from ulna to the radius (2). The innervation and vascularization of the third head of biceps brachii were from musculocutaneous nerve and brachial artery. This agrees with the normal embryologic development of the related dermatomes and myotomes. It is presumed that the development of the biceps brachii muscle is likely to influence the course and the branching pattern of musculocutaneous nerve (13,18). The median nerve supplying the supernumerary head was rare and not found in literature. In the past many variations have been described regarding the course of the musculocutaneous and median nerves. Le Minor (19) described five types of variations: Type 1: There is no communication between the median and musculocutaneous nerve. Type 2: The fibers of medial root of median nerve pass through the musculocutaneous nerve and join the median nerve in the middle of the arm. Type3: The lateral root fibers of medial root of median nerve pass through the musculocutaneous nerve and after some distance, leave it to form the root of the median nerve. Type 4: The musculocutaneous fibres join the lateral root of the median nerve and after some distance the musculocutaneous arise from the median nerve. Type 5: The musculocutaneous nerve is absent and the entire fibres of musculocutaneous pass through lateral root and fibres to the muscles supplied by musculocutaneous nerve branch out directly from median nerve. Venieratos and Anagnostopoulou (20) also described three different types of communication between musculocutaneous and median nerve in relation to coracobrachialis muscle. Type 1: communication between musculocutaneous and median nerve is proximal to the entrance of musculocutaneous into coracobrachialis. Type 2: communication between the two nerves is distal to the muscle. Type 3: neither the nerve nor its communicating branch pierced the muscle. In the present study the three specimens (50%) of supernumerary head of biceps brachii muscle were supplied by median nerve. The absence of musculocutaneous nerve was coincided with type 5 of Lee Minor but did not coincide with any of Venieratos's classification (19, 20). The knowledge of such variations is important during surgical corrections of the arm as well as in diagnosing the nerve impairments. Furthermore, it has been mentioned that any variant nerve with an abnormal origin, course and distribution is prone to accidental injuries and impairments (21). This is further proved by the fact that supernumerary heads of the biceps brachii muscle have been reported to compress the surrounding neurovascular structures leading to erroneous interpretations during surgical procedures (18). The biceps brachii is known for its powerful elbow flexion and supination of the forearm. It can be argued that the presence of supernumerary heads of biceps brachii muscle increase its kinematics. Therefore, from anatomical standpoint of view it can be presumed that the presence of a third head may increase the power of flexion and supination of the forearm (13). In addition to allowing the elbow flexion irrespective of the shoulder joint position, the supernumerary head of biceps brachii may enhance the strength of elbow flexion (16). Competing interests: The authors declare that they have no competing interests. Authors' contributions: SPS wrote the case report, performed the literature review and obtained the photograph for the study. RMM performed the literature search and assisted with writing the paper. STS conceived the study and helped to draft the manuscript. All authors have read and approved the final version manuscript.
ACKNOWLEDGEMENT
All the authors wish to convey our sincere thanks to Dr. Arif A. Faruqui for his valuable help, support and inspiration. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
1. Standring S, Ellis H, Healy JC, Johnson D et al. Gray’s Anatomy. In: General organisation and surface anatomy of the upper limb.39th ed. Philadelphia Elsevier Churchill Livingstone, 2005: 803-4.
2. Testut, L. and Latarjet, A. Compendio de anatomia descriptive. 22nd Ed. Buenos Aires, Salvat, 1981.
3. Asvat, R.; Candler, P. and Sarmiento, E. E. High incidence of the third head of biceps brachii in South African populations. J. Anat., 182:101-4, 1993.
4. Nakatani, T.; Tanaka, S. and Mizukami, S. Bilateral fourheaded biceps brachii muscles: the median nerve and brachial artery passing through a tunnel formed by a muscle slip from the supernumerary head. Clin. Anat., 11:209-12, 1998.
5. Nayak, S. R.; Ashwin, K.; Madhan, K. S. J.; Latha, V. P.; Vasudha, S. and Merin, M. T. Four-headed biceps and triceps brachii muscles with neurovascular variation.Anat. Sci. Intl., 83:107-11, 2008.
6. Sargon, M. F.; Tuncali, D. and Celik, H. H. An unusual origin for the supernumerary head of biceps brachii muscle. Clin. Anat., 9:160-2, 1996.
7. Khaledpour, C. Anomalies of the biceps muscle of the arm. Anat. Anz., 158:79-85, 1985
8. Kopuz, C.; Sancack, B. and Ozbenli, S. On the incidence of the third head of biceps brachii in Turkish neonates and adults. Acta. Anat. Nippon., 74:301-5, 1999
9. Rai, R.; Ranade, A. V.; Prabhu, L. V. and Prakash, M. M. P. Third head of Biceps brachii: A study in Indian population. Singapore Med. J., 48:929-31, 2007.
10. Bergman, R. A.; Thompson, S. A.; Afifi, A. K. and Saadeh, FA. Compendium of human anatomic variation. 1st Ed. Baltimore, Urban and Schwarzenberg, 1988.
11. Torre, F. R. L.; Cegarra, J. N. and Berruezo, J. P. Biceps brachii muscle attached to the extensor carpii radialis brevis muscle: an unreported anatomical variation in humans. Anat. Anz., 176:319-21, 1994.
12. Kosugi, K.; Shibata, S. and Yamashita, H. Supernumerary head of biceps brachii and branching pattern of the musculocutaneous nerve in Japanese. Surg. Rad. Anat., 14:175- 85, 1992.
13. Kumar, H.; Das, S. and Rath, G. An anatomical insight into the third head of biceps brachii muscle. Bratisl. Lek. Listy., 109:76-8, 2008.
14. Tountas, C. P. and Bergman, R. A. Anatomic variations of the upper extremity. New York, Churchill Livingstone, 1993.
15. Rincon, F.; Rodriquez, I. Z. and Sanchez A. The anatomic characteristics of the third head of biceps brachii muscle in Colombian population. Rev. Chil. Anat., 20:197-200, 2002.
16. Swieter, M. G. and Carmichael, S. W. Bilateral three-headed biceps brachii muscles. Anat. Anz., 148:346-9, 1980.
17. Santo Neto, H.; Camilli, J. A.; Andrade, J. C.; Meciano, F. J. and Marques, M. J. On the incidence of the biceps brachii third head in Brazilian white and blacks. Anat. Anz., 180:69-71, 1998.
18. Warner, J. P.; Palleta, G. A. and Warren, R. F. Supernumerary Head of the Biceps brachii, Case report demonstrating clinical relevance. Clin. Ortho. Res., 280:179-81, 1992.
19. Le Minor JM. A rare variant of the median and musculocutaneous nerves in man. Archieves Anatomy Histology Embryology 1992; 73: 33-42.
20. Venierators D and Anangnastopoulou S classification of communication between the musculocutaneous and median nerves. Clincal Anatomy. 1998; 11: 327-331.
21. Roberts, W. H. Anomalous course of the median nerve medial to the trochlea and anterior to the medial epicondyle of the humans. Anat. Anz., 174:309-11, 1992.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





