IJCRR - 4(20), October, 2012
Pages: 125-126
Date of Publication: 20-Oct-2012
Print Article
Download XML Download PDF
UNILATERAL INCOMPLETE SUPERFICIAL PALMAR ARCH- A CASE REPORT
Author: Ch. Roja Rani, B. Narasinga Rao, M. Pramila Padmini
Category: Healthcare
Abstract:Superficial palmar arch (SPA) is an arterial arcade and a dominant vascular structure of the palm. In hand surgeries like vascular graft applications arterial repairs, free and pedicled flaps, clinicians should be aware of these variations, because in most of the traumatic events and the surgical procedures of the hand the SPA plays an important role. In the present case, the superficial palmar arch is incomplete and there is no communication between the superficial branches of radial and ulnar arteries. The ulnar artery is giving a proper digital and two common palmar digital branches and the superficial branch of radial artery is giving a common palmar digital branch to supply the half of radial side of middle finger and ulnar side of index finger and radialis indicis supplying the radial side of index finger.
Keywords: anastomosis, arteria princeps pollicis, flexor retinaculum, radialis indicis, superficial palmar arch
Full Text:
INTRODUCTION
Superficial palmar arch (SPA) is an arterial arcade and a dominant vascular structure of the palm. Superficial palmar arch is localized just deep to palmar aponeurosis and is superficial to digital branches of the median nerve, long flexor tendons of the forearm and lumbricals of the palm. The arch is formed by the superficial terminal branch of the ulnar artery with superficial palmar branch of the radial artery or arteria princeps pollicis (APP) or arteria radialis indicis (ARI) from the radial artery. An incomplete arch exists due to absence of anastomosis between the vessels constituting the arch. Knowledge in variations of vascular pattern in hand surgeries like vascular graft applications, arterial repairs, free and pedicled flaps is important, and clinicians should be aware of these variations. In most of the traumatic events and the surgical procedures of the hand the SPA plays an important role.
MATERIAL AND METHODS
Anatomical variations of the vessels of the palm region are carried out on 20 cadavers (18 male and 02 female during the years 2009-2012.
CASE REPORT
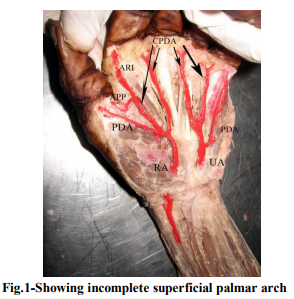
The present variation is observed in an adult male cadaver during routine dissection in the Department of Anatomy, MIMS, and Vizianagaram. In the present case, there is a unilateral variation of superficial palmar arch seen in the left hand. There is no anastomosis between the superficial branches of Radial artery & Ulnar artery in the left hand. The superficial branch of ulnar artery entered the palm superficial to flexor retinaculum and divide into two common and one proper palmar digital braches supplying the ulnar side of middle & radial side of ring finger, ulnar side of ring & radial side of little finger and proper branch supplying ulnar side of little finger. The superficial branch of radial artery entered the hand deep to thenar muscles and dividing into two common palmar digital braches and one proper palmar digital branch supplying the adjacent sides of thumb & index finger, index and middle finger and proper palmar digital branch supplying radial side of the thumb (fig.1). In the right hand the SPA is having a normal course.
DISCUSSION
The superficial arteries of the hand formed several diversified patterns that permitted into welldefined categories. According to Coleman’1 (1961) classification, in type A: Both superficial palmar branches of UA and RA take part in supplying the palm and fingers, but in doing so fail to anastomose and seen in 3.6% of cases. In the present case also there is a similar observation. Ikeda et al. conducted stereoscopic arteriography of 220 cadaver hands and reported complete SPA in 96.4% of cases and 3.6% as incomplete arch. Gellman et al2 .2001 reported 84.4% of cases as complete SPA and 15.5% of cases as incomplete SPA. Al Turk and Metcalf 3 (1984) showed complete SPA in 84% of cases and incomplete in 16% using Doppler flow meter. Harvesting RA for use as arterial by-pass conduits needs to look specifically for variation in collateral circulation like presence of incomplete SPA (Ruengsakulrach P 4 2001).
CONCLUSION
Patients with coronary artery disease should be screened before RA harvesting to confirm the presence of viable collateral circulation. Currently the methods of assessing hand circulation include the modified Allen test, Doppler ultrasonography, photoplethysmography. Doppler study is a useful tool in preoperative screening for RA harvesting for myocardial revascularization (Pola P5 1996)
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Coleman SS, Anson BJ. Arterial patterns in the hand based upon a study of 650 specimens. Surg Gynecol Obstet. 1961; 113: 409–424.
2. Gellman H, Botte MJ, Shankwiler J, Gelberman RH. Arterial patterns of the deep and superficial palmar arches. Clin Orthop Relat Res. 2001; 383: 41–46.
3. Al-Turk M, Metcalf WK. A study of the superficial palmar arteries using the Doppler Ultrasonic Flowmeter. J Anat. 1984; 138: 27– 32.
4. Ruengsakulrach P, Brooks M, Hare DL, Gordon I, Buxton BF. Preoperative assessment of hand circulation by means of Doppler ultrasonography and the modified Allen test. J Thorac Cardiovasc Surg. 2001; 121: 526–531.
5. Pola P, Serricchio M, Flore R, Manasse E, Favuzzi A, Possati GF. Safe removal of the radial artery for myocardial revascularization: a Doppler study to prevent ischemic complications to the hand. J Thorac Cardiovasc Surg. 1996; 112: 737–744.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





